1607
Sex Differences in Control of
Cutaneous Blood Flow
John P. Cooke, MD, PhD, Mark A. Creager, MD,
Philip J. Osmundson, MD, and John T. Shepherd, MD, DSc
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
Women are far more likely than men to suffer from Raynaud's disease. The purpose of this
study was to determine whether there are gender differences in local or central control of
cutaneous blood flow that could account for the increased incidence of Raynaud's disease in
women. To assess cutaneous blood flow, hand blood flow (HBF), finger blood flow (FBF), or
skin perfusion (SP) was measured by fluid plethysmography, mercury strain-gauge plethysmography, or laser Doppler spectroscopy, respectively, in 47 volunteers. Basal HBF in men
exceeded that of women (12.1±2.0 versus 6.2±1.5 mlU100 ml/min). Likewise, FBF in men
surpassed that of women (19.5±4.1 versus 7.7±1.8 ml/100 mlVmin). Similarly, SP in men was
greater than that of women (270±42 versus 81±16 perfusion units). However, after total body
warming (to induce a thermal sympatholysis), HBF in women exceeded that of men, suggesting
that the lower basal HBF in women was due to increased sympathetic outflow to the extremities.
Mental stress and deep inspiration reduced HBF and SP in men. Paradoxically, both of these
maneuvers increased HBF and SP in women. To determine whether these paradoxical
responses in women were due to the women's elevated basal sympathetic tone, these experiments were repeated after total body cooling in men to increase sympathetic tone and after total
body warming in women to reduce sympathetic tone. Total body cooling reduced HBF and SP
in men. Under these conditions, mental stress and deep inspiration induced vasodilation. In
women, total body warming for 10 minutes increased HBF. Under these conditions, mental
stress and deep inspiration induced vasoconstriction. In conclusion, basal cutaneous blood flow
is reduced in women. This appears to be due to a basal increase in sympathetic tone rather than
to a local structural or functional difference in the cutaneous circulation. In addition, a
paradoxical vasodilation in response to mental arithmetic and deep inspiration is unmasked at
high levels of sympathetic tone. The gender differences in cutaneous blood flow may account for
the increased incidence of Raynaud's disease in young women. (Circulation 1990;82:1607-1615)
R aynaud's disease is a vasospastic disorder
characterized by excessive vasoconstriction
of the cutaneous circulation of the extremities.' Attacks of Raynaud's disease are precipitated
by ambient cold or mental stress and are thought to
be mediated by increases in sympathetic nervous
outflow to the cutaneous vasculature. A "local fault"
in the digital circulation is thought to predispose
From the Division of Vascular Medicine (J.P.C., M.A.C.),
Brigham and Women's Hospital and Harvard Medical School,
Boston, and the Departments of Physiology and Biophysics
(J.T.S.) and Internal Medicine (P.J.O.), Mayo Clinic and Mayo
Foundation, Rochester, Minn.
Supported in part by National Institutes of Health grant HL05883 (J.T.S.) and by an American Heart Association Grant-inAid (J.P.C.). J.P.C. was supported by an American College of
Cardiology Merck Fellowship grant.
Address for correspondence: John P. Cooke, MD, PhD, Division of Cardiovascular Medicine, Stanford University School of
Medicine, 300 Pasteur Drive, Stanford, CA 94305.
Received February 5, 1990; revision accepted June 19, 1990.
subjects to excessive vasoconstriction during elevations in sympathetic tone. Women are far more likely
than men to suffer from Raynaud's disease.2 It is not
known if this increased incidence in women is due to
local structural or functional differences in the cutaneous circulation or if increased sympathetic tone to
the limbs predisposes women to this disorder. Thus,
the purpose of this study was to determine if there
are gender differences in local or central control of
cutaneous blood flow that could account for the
increased incidence of Raynaud's disease in women.
Methods
Subjects
Informed consent was obtained from the 23 men
and 26 women who participated in this investigation,
which was approved by the institutional review board
of the Mayo Clinic. The participants (age range,
22-38 years) were in good health and, with one
1608
Circulation Vol 82 No 5, November 1990
exception, did not use tobacco. On the day of the
study, they were asked to refrain from consuming
vasoactive substances, including caffeine.* Subjects
were studied in a postprandial state and were lightly
clothed in hospital scrub suits. Subjects rested quietly
in a supine position in the laboratory (room temperature, 23° C) for 20 minutes before data were collected. External stimuli were reduced to a minimum.
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
Techniques
Three complementary techniques were used to
assess cutaneous blood flow: 1) volume plethysmography of the hand, 2) mercury strain-gauge plethysmography of the finger, and 3) laser Doppler spectroscopy of the finger. Volume plethysmography of
the hand provides highly accurate and reproducible
measurements of hand blood flow over a wide range
of flow. A disadvantage of this technique is that
although hand blood flow predominantly reflects
cutaneous blood flow, a portion of the total value is
contributed by skeletal muscle.3 Conversely, finger
blood flow almost exclusively represents cutaneous
blood flow, and this is the strength of using finger
plethysmography.3 However, mercury strain-gauge
plethysmography of the finger is not as accurate or
reliable as the former technique, particularly at
higher values of flow. Laser Doppler spectroscopy
measures skin perfusion of a small volume of tissue
(a hemisphere with a radius of 1 mm) beneath the
probe head. It therefore exclusively reflects cutaneous blood flow. An additional advantage is the short
time constant of this technique; however, measurements are only semiquantitative.4
To measure hand blood flow, a water-filled
plethysmograph was used. The water temperature of
the plethysmograph was thermostatically controlled
and continuously monitored and could be adjusted to
warm or cool the hand. The outlet of the plethysmographic chamber was connected by stiff plastic tubing
to a pressure transducer. Before each experiment,
the transducer was calibrated volumetrically. With
the subject supine, the hand was inserted into a
loosely fitting surgical glove affixed to the plethysmograph. The position of the plethysmograph was then
adjusted to maintain the hand at a level above the
right atrium. The upper extremity was supported by a
padded arm board, and the patient's position was
adjusted to maximize comfort and minimize respiratory artifact. A collecting cuff was applied to the
wrist, and its position was adjusted to reduce inflation artifact; pressures of 40-70 mm Hg were used to
impede venous return, and were delivered automatically by a servosystem (Periflow, Janssen Scientific
Instruments). The minimal pressure evoking the
greatest rate of increase in hand volume was deter*One female subject used oral contraceptives, and another was
on thyroid hormone replacement therapy. Their responses were
not different from those of the other female subjects and are thus
included in the study. One male subject was an occasional smoker,
but he refrained from tobacco on the day of the study.
mined for each subject. Hand volume was determined volumetrically, and hand blood flow was
expressed in milliliters per 100 milliliters of tissue per
minute. Each blood flow determination is the average
of five successive blood flow recordings made at
10-second intervals. The effect of a deep inspiration
on hand blood flow is transitory, and only the first
recording of hand blood flow after this maneuver was
analyzed.
To measure finger blood flow, mercury straingauge plethysmography was used. The strain gauge
was calibrated, placed circumferentially around the
distal phalanx of the second or third digit, and
connected to a Hokansen plethysmograph. A 2.5 -cm
cuff was placed at the base of the finger and inflated
to the lowest venous occlusion pressure (30-50 mm
Hg) required to produce the maximum increase in
finger circumference for each subject. Finger blood
flow was derived from the rate of change in finger
circumference during acute venous occlusion and was
expressed in milliliters per 100 milliliters of tissue per
minute. Each measurement of finger blood flow
comprised 10 serial blood flow determinations.
Skin perfusion was assessed by laser Doppler
spectroscopy (laser Doppler Flowmeter Periflux 3).
The probe head was fixed to the volar aspect of the
thumb by an adhesive ring. Movement artifact was
made negligible by the use of a rigid arm support.
The analog output from the flowmeter (as well as
that from the plethysmograph) was continuously
monitored with a strip-chart recorder. A reference
baseline for the flowmeter recordings corresponding
to zero perfusion was obtained by inflating an arm
cuff to supraphysiological pressures and recording
the Doppler signal during this time. Each skin perfusion value is the average of 10 measurements at
5-second intervals. In some experiments, blood pressure was measured by sphygmomanometry.
Specific Protocols
Changes in cutaneous blood flow in response to
regional temperature changes may be under central
control (i.e., changes in sympathetic nervous actMity)
or local control (i.e., changes in affinity of the
adrenoceptors in the vessel wall). To study the gender differences in local and central control of cutaneous blood flow, the following protocols were followed.
Gender differences in basal cutaneous bloodflow. To
determine if there were gender differences in basal
cutaneous blood flow at room temperature (23° C),
hand blood flow, finger blood flow, or finger skin
perfusion was measured in 49 subjects (23 men and
26 women).
Gender differences in the interaction of central and
local control. To study the interaction of central and
local control of cutaneous blood flow in response to
local temperature changes, the following study was
performed. Hand blood flow was measured simultaneously in both extremities at 320 C. The temperature in one plethysmograph was maintained at 320 C.
Cooke et al Cutaneous Blood Flow
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
The temperature in the other plethysmograph was
increased to 42° C (local warming) and thereafter
reduced by decrements of 40 C every 5 minutes to a
final temperature of 220 C (local cooling) while continuously monitoring flow in both hands. Any
changes occurring in flow to the hand maintained at
320 C are due to central effects (i.e., changes in
sympathetic outflow to the extremities). Any additional change in flow of the warmed or cooled hand is
then due to local superimposed effects of the temperature change.
Gender differences in local control. The following
experiment was performed to examine local control
of cutaneous blood flow in the absence of central
control. Hand blood flow was measured simultaneously in both extremities at 320 C. One plethysmograph was then heated to 420 C (local warming), and
the other was cooled to 220 C (regional cooling).
Subsequently, subjects were placed between two
hypothermia blankets with fluid inflow temperatures
of 450 C. Total body warming was performed for 40
minutes to abolish sympathetic tone ("thermal
sympatholysis").5 This way, the local control of cutaneous blood flow in response to regional temperature
changes could be evaluated in the absence of sympathetic tone. Hand blood flow, blood pressure, and
oral temperature were measured every 10 minutes.
To determine the effectiveness of the thermal
sympatholysis, the flow responses to mental stress as
well as to deep inspiration were observed at 10minute intervals. Mental stress was induced by asking
subjects to perform mental arithmetic using standardized sums. After performing mental arithmetic,
the subjects were asked to take a deep breath to
maximal inspiratory capacity and then exhale passively.
Gender differences in central control. First, the initial
protocol was designed to assess central control of
cutaneous blood flow in the absence of local changes
in temperature that might affect local control. Therefore, while local temperature was held constant
(plethysmograph temperature, 320 C), hand blood
flow was examined during reflex activation of sympathetic tone (mental stress and deep inspiration).
Second, the above protocol revealed paradoxical
vasodilation to mental stress and deep inspiration in
women. To determine if the paradoxical responses
were associated with an elevated basal sympathetic
tone, the following experiment was performed. Hand
blood flow and skin perfusion were measured in five
men at rest and during mental stress and deep
breath. Subsequently, the men were placed between
hypothermia blankets for 5 minutes of total body
cooling (inflow temperature, 50 C) to elevate sympathetic tone, and the flow measurements were
repeated. Similarly, eight women were placed
between hypothermia blankets (inflow temperature,
450 C), and hand blood flow response to mental
arithmetic (n=8) and deep inspiration (n=5) were
assessed before and after total body warming (to
reduce sympathetic tone).
1609
TABLE 1. Effect of Deep Inspiration on Skin Perfusion
Skin perfusion (perfusion units)*
Basal
After deep inspiration
270±42
130±42t
Women
81±16t
177±30t
Cooled men§
106±22t
202±34
*Arbitrary perfusion units, as measured by laser Doppler spectroscopy.
tp<0.05, significantly different from basal value obtained under
standard environmental conditions.
tp<0.05, significantly different from value observed in men.
§Men were subjected to total body cooling for 5 minutes.
Subjects
Men
n
5
5
5
Hormonal effects on control ofcutaneous bloodflow.
To determine if the gender differences were phasically affected by the estrous cycle, the following
experiments were performed. Oral temperature,
blood pressure, and hand blood flow were measured
twice weekly for 1 month in six women and three
men. The female volunteers recorded their rectal
temperature daily as well as the onset and duration
of menses. After completing the hand blood flow
measurements, 7 ml of venous blood was obtained on
each experimental day from each female subject for
measurement of estradiol and progesterone.
Statistics
Most of the 49 subjects participated in several of
the experimental protocols during a period of 6
months and had measurements obtained on as many
as 12 different occasions.
Values are given as mean±SEM. Statistical evaluation of the data was by Student's t test for paired or
unpaired observations. Where multiple comparisons
were made, an analysis of variance was used, followed by a Newman-Keuls test. Ap value of less than
0.05 was considered significantly different.
Results
Basal Cutaneous Blood Flow
Basal hand blood flow in men (n=13) exceeded
that of women (n = 14) at a plethysmograph temperature of 32° C (12.1+2.0 versus 6.2±1.5 ml!100 ml/
min, p<0.02). * Likewise, at room temperature, basal
finger blood flow in men (n =8) exceeded that of
women (n=11) (16.9+4.8 versus 7.7±1.8 ml/100 ml!
min). Similarly, skin perfusion in men was greater
than that in women under standard environmental
conditions (Table 1). These differences in cutaneous
blood flow were due to differences in vascular resistance; hand vascular resistance in men (n = 8) was less
than that in women (n=8) (4.7±0.6 versus 21.4+6.8
Wood units, p=0.02).
Interaction of Central and Local Control
Warming the hand (plethysmograph temperature,
420 C) caused hand blood flow to increase in both
*Where multiple determinations of basal hand blood flow were
made in one individual under the same conditions, these results
were averaged and expressed as one value.
Circulation Vol 82 No 5, November 1990
1610
1!
WA RMED CONTROL COOLED
HAND
HAND
HAND
CONTROL
HAND
40
E 30
0
E
20
E
X~5
0
\
m
l
Total
0
-10
T
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
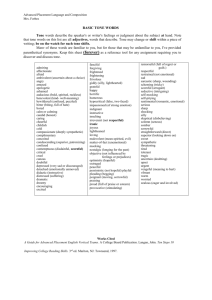
FIGURE 1. Bargraph ofchange in hand bloodflow (A HBF)
induced by local temperature changes in men (n=9) and
women (n=9). Local warming (warmed hand) causes hand
blood flow to increase in both women (open columns) and
men (dark columns). During local warming, HBF does not
change in the contralateral hand maintained at 320 C (control
hand). Local cooling (cooled hand) causes a greater reduction
in HBF in men than in women (p=0.02). During local
cooling, flow also drops in the contralateral hand maintained
at 32° C (control hand) to a greater degree in men (p= O0. 7).
groups (men: 15.6±+1.9 to 20.7±+1.9 ml/100 ml/min,
n=9, p=0.04; women: 9.2+2.7 to 16.9+2.5 ml/100
ml/min, n=9, p =0.03). During local warming, blood
flow in the contralateral hand (control, maintained at
320 C) did not change in either group (Figure 1).
Therefore, the increased flow in the warmed hand is
not due to withdrawal of sympathetic tone to the
extremity but probably is due to local antagonism of
adrenergic responsiveness.6
Cooling the hand (plethysmograph temperature,
220 C) caused blood flow to decrease significantly in
both groups (men: 15.6±1.9 to 2.3±0.6 ml/100 ml!
min, n=9, p=0.006; women: 9.2±2.7 to 2.4±1.0
ml/100 ml/min, n=9, p =0.02). The reduction in flow
was greater in men than in women (Figure 1).
During local cooling, blood flow in the contralateral hand (control, maintained at 320 C) decreased in
each of the men (n=9) (15.8±1.9 to 6.7±1.3 ml/100
ml/min, p=0.009). Paradoxically, in three of the
women (n=9), the contralateral hand vasodilated;
for this reason, in women the reduction in flow in the
contralateral (control) hand did not reach significance (8.9±2.2 to 6.8±1.4 ml/100 ml/min, p=NS).
The reduction in hand blood flow in the contralateral
(control) hand was greater in men than in women
(Figure 1). The reduction of flow in the contralateral
hand is due to activation of sympathetic nervous
outflow. Since basal sympathetic tone appears to be
increased in women, further elevation of sympathetic
tone may be limited. This would explain the reduced
response to cooling in women. If basal sympathetic
tone is elevated in women, maneuvers to reduce
sympathetic tone should cause female hand blood
flow to increase to a greater degree. To test this
hypothesis, blood flow was measured during thermal
/I0 Wormed hond
*Cooled hand
E
E MALE_
C]O FEMALE
*
-
Body
Worming
10
20
TIME (min)
30
40
60 FEMALES
0
E
403020
n8)
E20
m
0 Wormed hand
Cooled
1
0L
Total
Body
Wormning 30
10
20
TIME (min)
hand
40
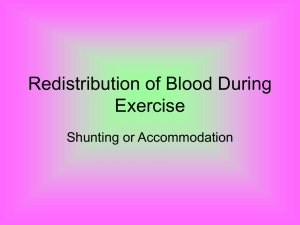
FIGURE 2. Plots of effects on hand blood flow (HBF) of
local cooling or warming before and during "thermal sympatholysis" (total body warming) in men (top panel) and
women (bottom panel). In both men and women, local
cooling reduces and local warming increases HBF. The
difference in blood flow between the warmed and cooled
hands is in part mediated by local effects because the difference in flow between the warmed and cooled hands is
maintained after thermal sympatholysis. After local and total
body warming, HBF in women exceeds that of men; this
suggests that under standard environmental conditions, the
lower HBF in women is due to increased sympathetic tone
rather than to local functional or structural differences in the
cutaneous vascular bed. Top panel: *p=0.04, **p=0.008;
bottom panel: *p=0.02, **p=0.006.
sympatholysis. In addition, during total body warming, one hand was cooled and the other was warmed
to determine if local temperature changes had effects
on flow in the absence of sympathetic tone.
Local Control of Hand Blood Flow
Total body warming induced a significant and
identical increase in core temperature in both groups
(men: 36.8+0.10 to 37.7±+0.10 C, n=8, p=0.03;
women: 36.9 ±0.1° to 37.7+0.20 C, n=8, p =0.04). In
both groups, this increase in core temperature
induced a "thermal sympatholysis" as evidenced by
an increase in hand blood flow (Figure 2) and
abolition of the vasoconstriction with mental stress
after 40 minutes of body warming (data not shown).
After total body warming, hand blood flow in women
(n=9) exceeded that of men (n=9) (54.2+4.2 versus
42.8+±3.2 ml/100 ml/min, p<0.001).
Despite the attenuation of central control, there
remained a persistent difference in flow between the
I
Cooke et al Cutaneous Blood Flow
1611
(Male Subject)
Blood Flow
(left hand)
Baseline
Mental Arithmetic
(Female Subject)
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
Mental Arithmetic
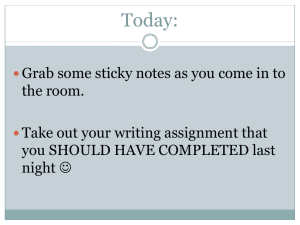
FIGURE 3. Tracings of original records of hand blood flow (measured
by venous impedance plethysmography) and skin perfusion (measured by
laser Doppler spectroscopy) before
and during mental arithmetic in a
male and a female subject. In the
male subject (upper panel), blood
flow (upper tracing) decreases during
mental arithmetic (note that the
slopes of the blood flow recordings
are reduced during mental arithmetic). Simultaneously, skin perfusion (lower tracing) decreases during
mental arithmetic (note the reduced
distance of the tracing from the baseline, which represents zero perfusion).
In the female subject (lower panel),
blood flow is less than that of the
male subject under basal conditions
(note the reduced slope of the blood
flow recordings). During mental
arithmetic, hand bloodflow paradoxically increases. Similarly, skin perfusion (lower tracing) is less than that
of the male subject (note the reduced
distance of this tracing from the baseline). During mental arithmetic, skin
perfusion paradoxically increases in
the female subject.
~ ~ ~ ~ ~ ~ ~ ~ ~|\_~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~1
Blood Flow
(lef t hand)
Skin Perfusion
(right thumb)
30 seconds
Baseline
warmed and the cooled hands (46.5 ± 1.6 versus
34.4±2.4 ml/100 ml/min,p<0.001, n=15). The difference in flow between warmed and cooled hands was
similar in men and women (men: 12.6±1.7 mlI100
ml/min, n=8; women: 11.6±5.1 ml/100 ml/min, n=7)
after total body warming for 40 minutes (Figures 2A
and 2B).
These experiments suggest that in both men and
women, there appear to be local mechanisms mediating hand blood flow responses to temperature
changes in the absence of sympathetic control. Furthermore, the lower basal hand blood flow in women
appears to be due to enhanced sympathetic activity
rather than to local functional or structural differences in the vascular bed. The subsequent experimental protocol was designed to determine whether
the increase in basal sympathetic tone to the cutaneous vasculature altered reflex vasomotor responses.
Central Control of Hand Blood Flow
Mental stress reduced hand blood flow and skin
perfusion in men (Figures 3 and 4A). Deep inspiration had the same effect in men (Figure SA and Table
1). Paradoxically, both of these maneuvers caused an
increase in hand blood flow and skin perfusion in
women (Figures 3, 4B, and 5B and Tables 1 and 2).
In a subset of subjects, measurements of arterial
pressure were also obtained during these maneuvers
to calculate hand vascular resistance. These measurements revealed that during these maneuvers, the
observed decrease in hand blood flow in men was due
to increased hand vascular resistance (Table 2).
Conversely, the increase in hand blood flow in
due to a decrease in hand vascular
resistance (Table 2).
To determine if these paradoxical responses in
women were due to their elevated basal sympathetic
tone, these experiments were repeated after total
body cooling in men (for 5 minutes) to increase
sympathetic tone and total body warming (for 10
minutes) in women to reduce sympathetic tone.
Total body cooling caused a reduction in hand
blood flow and skin perfusion in men. Under these
conditions, the responses to mental stress and deep
inspiration were qualitatively different from those in
men during basal conditions. Mental stress now
increased hand blood flow (Figure 4C). Similarly,
deep inspiration increased skin perfusion (Table 1).
women was
Circulation Vol 82, No 5, November 1990
1612
B.
A.
2 30
.E 24
0 18
0
12
ULL
I
20
E
a
Basal1
E
a]
P
<
o
Bosa
Post MA
D.
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
c 60
48 o 36
o
24\
112
at o
8
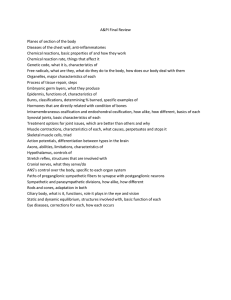
Panel C: After total body cooling
p=O.0l).
(TBC), HBF in men is reduced. Under these
o
conditions, MA induces a vasodilation
E
E_.
E
6
0
0
4
UI
>
5
I
C.
c
A
8 10 10
6
0'
2
f
0
-1-
Basoa
(after TBC)
(2.4±0.7 to 3.2±0.6 ml/100 ml/min,
D: Total
p=0.003).
body causes
warming
10 minutes
in women
an
(TBW) for Panel
increase in HBF. Under these conditions, MA4
tends to induce a vasoconstriction (40.8±2.8
to 34.7±4.1 ml/100 ml/min, p=NS).
'0
Post MA
Basoa
(after TBW)
In women, total body warming for 10 minutes
increased hand blood flow. Under these conditions,
the responses to mental stress and deep inspiration
were qualitatively different from those of women
during basal conditions. Deep inspiration now
reduced hand blood flow, and mental stress no longer
induced vasodilation (Figures 4D and 5D). To summarize, in a setting of reduced sympathetic tone
(basal conditions for men, or warmed women), vasoconstriction is observed during deep inspiration.
A.
18
0
12
E
6
UL.
m
Ir
0
0
E
i
Hormonal Effects on Control of Hand Blood Flow
Basal hand blood flow and the response to mental
stress or deep inspiration remained stable in men and
women over time (Figures 6A and 6B). There was no
15
o
*
lo
10
5
Efi
o
I
Post Dl
C.
Bosol
D.
_
60
8
6
Ef
4
o
2
E
0
m
I
U-
m
Conversely, with increased sympathetic tone (basal
conditions for women, or cooled men), a paradoxical
vasodilation is observed during deep inspiration and
mental arithmetic.
20
E
Bosal
E
0
0
Post MA
B.
30
c
E 24
._c
FIGURE 4. Plots of effects of mental arith* metic (MA) on hand blood flow (HBF) in
male (0) and female (o) subjects. Panel A:
.
MAreduces HBF in male subjects (1 9.3 +-2.2
to 12.4±2.2 ml/100 mllmin, p=0.02). Panel
B: In female subjects, HBF under basal conditions is less than that in men. Paradoxically,
Post MA MA induces a vasodilation in female subjects
(4.7±0.7 to 10.2±1.7 ml/100 ml/min,
l5
::
Basal
(ofter TBC)
Post DI
48
36
3
12
0
osel
(of ter TBW)
,
FIGURE 5. Plots of effects of deep inspiration (DI) on hand blood flow (HBF) in
male (a) and female (o) subjects. Panel
A: DI reduces HBF in male subjects
(19.9±2.5 to 8.6±1.3 ml/100 mllmin,
p=O.02). Panel B: In female subjects,
HBF under basal conditions is less than
I
that in men. Paradoaically DI tends to
Post Dl induce a vasodilation in female subjects
(5.6±0.7 to 9.6+1.4 ml/100 ml/min,
p=NS). Panel C: After total body cooling
(TBC), HBF in men is reduced. Under
these conditions, DI tends to induce a
vasodilation (2.8+0.9 to 4.0±0.8 ml/100
mlmin, p=NS). Panel D: Total body
* warming (TBW) for 10 minutes in women
7Z 24 -causes an increase in HBF. Under these
conditions, deep inspiration now induces a
vasoconstiction (44.7+3.4 to 26.1±2.5
ml/i 00 ml/min, p=0. 009).
Post DB
Cooke et al Cutaneous Blood Flow
TABLE 2. Hemodynamic Effects of Mental Stress or Deep Inspiration
During mental arithmetic
Basal
MAP
HR
HR
HBF
HVR
HBF
HVR
MAP
Men
10±2.4*
12±4
95+5 67+5*
(n=4) 20±4.4 5.2+1.0 92±4 62±5
Women
(n=5) 2.9±0.8
40±11
70±7
84±2
6.9±1.6*
18±6*
88±3
77±6*
HBF
1613
During deep inspiration
MAP
HVR
HR
5.5±0.9*
18+3*
90±4
60+4
4.6±0.6
19±4
80±3*
62±6
HBF, hand blood flow; HVR, hand vascular resistance; MAP, mean arterial pressure; HR, heart rate.
*Significantly different from basal value.
correlation between female hand blood flow and
levels of serum estrogen or progesterone (Figure 7).
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
Discussion
The major findings of this study were that 1) cutaneous blood flow in women is less than that in men,
2) this gender difference is due to differences in
central, rather than local, control mechanisms,
3) maneuvers generally believed to increase sympathetic outflow to the extremities induce cutaneous
vasoconstriction in men but a paradoxical vasodilation
in women, and 4) this paradoxical vasodilation is
unmasked in men under conditions in which sympathetic tone is elevated.
The control of hand blood flow is complex, and
both local and central forces are operative. Mental
stress, deep inspiration, or local cooling are generally
believed to increase sympathetic outflow, resulting in
10
ternaie moie
0
0 Basal HBF
13
M Post MA
.E
0
9 5
m
I
u'
n
7
14
21
28
DAY
10[
cutaneous vasoconstriction. Conversely, elevation of
core temperature reduces basal sympathetic outflow
and attenuates the vasoconstriction to mental stress
and deep inspiration -thermal sympatholysis.5 Thus,
the central nervous system, through sympathetic
effects, exerts a strong influence on cutaneous vasomotion.
The cutaneous vasoconstriction induced by increased
sympathetic tone is due in part to the release of
norepinephrine from sympathetic nerve endings. More
recently, it has become apparent that other cotransmitters may be released with norepinephrine from sympathetic nerve endings, including neuropeptide Y, ATP,
and 5-hydroxytryptamine.7-9 Both ATP and norepinephrine are released from sympathetic nerve endings
in canine cutaneous vessels, and together they are
responsible for cold-induced vasoconstriction.8 In
humans, 5-hydroxytryptamine probably plays a significant role in cold-induced vasoconstriction. Serotonergic
receptors have been demonstrated in human digital
arteries.10 Furthermore, the reflex reduction in finger
blood flow induced by body cooling is attenuated but
not abolished by a-adrenergic antagonists; the remaining vasoconstriction is reversed by ketanserin, the 5HT2 antagonist."1
However, local changes in the temperature of the
hand also induce regional effects that are not mediated by the central nervous system.'2 Local changes
in temperature alter vascular smooth muscle contractility through effects on calcium permeability and by
feae rnkmole
0,
°
O,
2
.E
a
Basal HBF
Post DI
JF
31
0
5
m
I
U,
|~~-7
21
14
28
DAY
FIGURE 6. Plots of hand blood flow (HBF) over the course
of 1 month under basal conditions and after (top panel)
mental arithmetic (MA) or (bottom panel) deep inspiration
(DI). HBF under basal conditions and the response to MA4 or
DI are fairly stable over the course of 1 month in male (n=3)
and female (n=6) subjects. Note that the HBF response to MA
and DI is qualitatively different between the two groups.
9
c
0E
E
2J
0~
8
Ii_
E
:X
z
0
1
cL
h
LLI
LL
0
I
15
DAYS
30
Itiunt)
W
FIGURE 7. Plot of hand blood flow (HBF, A), serum
estradiol (o), and serum progesterone (c) levels over the
course of 1 month in one representative female subject. There
was no cyclic fluctuation in HBF related to hormonal levels in
the six women studied.
1614
Circulation Vol 82, No 5, November 1990
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
influencing the sequestration, release, and disposition of endogenous norepinephrine.13-16 Furthermore, temperature may influence receptor-agonist
interactions to augment the vascular response to
adrenergic or serotonergic stimulation.11'17-19 Therefore, the predisposition of women to Raynaud's
disease could be due to gender differences in central
control of hand blood flow (i.e., elevated sympathetic
tone) or differences in local effects of temperature.
Thus, the purpose of this study was to determine if
there are gender differences in local or central control of hand blood flow that might account for the
increased incidence of Raynaud's disease in women.
This investigation uncovered gender differences in
control of cutaneous blood flow. Under standard
environmental conditions, hand blood flow, finger
blood flow, and skin perfusion in women were half
those of men. This difference appears to be due to an
increase in sympathetic outflow to the cutaneous
circulation in women. This is suggested by the observation that after total body warming (to induce
thermal sympatholysis), hand blood flow increased to
a greater degree in women.
In fact, after abrogation of sympathetic tone, hand
blood flow in women exceeded that of men. Therefore, local structural or functional differences in the
cutaneous circulation cannot account for the reduced
basal cutaneous blood flow in women. Results of this
study suggest that maximal achievable hand blood
flow is greater in women. This observation parallels
that made in the forearm, in which hyperemic blood
flow is greater in women.20 Thus, maximal blood flow
in both the cutaneous and muscular circulations of
the upper extremity appears to be greater in women.
If basal sympathetic outflow to the extremities is
tonically increased in women, one might expect a
downregulation of postjunctional a-adrenoceptors.
In women, there is a reduced response of finger
blood flow to intra-arterial infusion of adrenergic
agonists.21 One might also expect maneuvers that
further increase sympathetic tone to have less effect
on men. In the present study, maneuvers to increase
sympathetic tone caused blood flow to decrease to a
greater degree in men. For example, cooling the
hand activates sympathetic nervous outflow. This
maneuver induced a greater reduction in blood flow
in the contralateral hand in men. In three of the nine
women, this maneuver paradoxically induced vasodilation in the contralateral hand.
Mental stress and deep inspiration are also known
to activate sympathetic nervous outflow. Under standard environmental conditions, men responded to
these maneuvers with a cutaneous vasoconstriction.
Paradoxically, in women these maneuvers increased
hand blood flow. Hand blood flow primarily reflects
cutaneous blood flow, but a smaller fraction of the
total value is secondary to skeletal muscle blood flow.
Thus, a possible explanation of the paradoxical
increase in hand blood flow is an augmentation of
skeletal muscle blood flow. However, the increase in
skin perfusion detected by laser Doppler spectros-
copy exclusively represents a change in cutaneous
blood flow. It would therefore appear that the paradoxical vasodilation is due to cutaneous vasodilation.
A paradoxical vasodilation with mental stress has
also been reported in patients with Raynaud's
disease.22 In these subjects (all of whom were women), the performance of mental arithmetic induced
an increase in finger blood flow. The increase in
finger blood flow observed in this study was undoubtedly due to an augmentation of cutaneous blood flow,
as muscle and bone blood flow do not contribute
significantly to finger blood flow.
Because of the rapid onset of the paradoxical
vasodilation, it is not of humoral origin. The time
course of the response suggests a neurogenic
response. However, the paradoxical vasodilation
observed in Raynaud's patients was not blocked by
atropine, propranolol, or digital nerve anesthesia.22
More recently, Blumberg and Wallin23 described a
reflex cutaneous vasodilation to painful intraneural
stimulation in the foot. This vasodilation was
enhanced by body cooling and was not blocked by
atropine or propranolol but was abolished by local
nerve block. This vasodilation may in part be mediated by a local axonal reflex, possibly involving
release of a peptidergic neurotransmitter, since local
application of capsaicin abolished the response. Possible candidates for peptidergic vasodilation include
substance P (endothelium-dependent vasodilation)
and vasoactive intestinal peptide (endotheliumindependent vasodilation), both of which have been
demonstrated in other circulations.7,24
The paradoxical vasodilation is probably manifested in women and patients with Raynaud's disease
because of their elevated sympathetic tone. When
sympathetic tone was increased in men by total body
cooling, mental arithmetic and deep inspiration
induced a paradoxical vasodilation. Conversely, when
sympathetic outflow was reduced in women by total
body warming, deep inspiration induced vasoconstriction. It therefore appears that a vasodilatory
response as well as sympathetic vasoconstriction are
activated by mental arithmetic or deep inspiration.
When sympathetic tone is low, vasoconstriction predominates with these maneuvers. Conversely, against
a background of high sympathetic tone, the paradoxical vasodilation is unmasked. In support of this
hypothesis, Oberle and colleagues25 recently demonstrated that the reflex cutaneous vasomotor response
to deep inspiration, mental arithmetic, and painful
stimuli was dependent on the ambient temperature;
cooled subjects vasodilated and warmed subjects
vasoconstricted in response to these stimuli.
It is possible that opposing neurogenic impulses
are responsible for cold-induced vasodilation.26 This
phenomenon is observed during extreme local cooling of the hand. Under this condition, arteriolar
vasoconstriction is transiently interrupted by episodic
vasodilation. Indeed, some of our female subjects
exhibited cold-induced vasodilation during moderate
local cooling. The physiological role of cold-induced
Cooke et al Cutaneous Blood Flow
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
vasodilation may be to preserve episodic nutritive
flow during states of excessive vasoconstriction. Coldinduced vasodilation may be due to opposing neurogenic impulses, intermittent abrogation of local
adrenergic neurotransmission, or direct effects of
cold on the vascular smooth muscle.6,13-'9,27-29
To determine if the elevated sympathetic tone in
women was phasically influenced by the estrous cycle,
we made serial measurements of hand blood flow as
well as of plasma estradiol and progesterone. There
was no apparent relation between hormonal changes
and hand blood flow. It is therefore more likely that
the gender differences in sympathetic control of hand
blood flow are due to a tonic effect of estrogen and/or
progesterone. This is supported by the observation
that finger blood flow in women increases after
menopause.30 Furthermore, the manifestations of
Raynaud's disease are also attenuated with aging.31
Finally, a reduction in estrogenic influence (as evidenced by increases in levels of luteinizing hormone)
is associated with the vasomotor phenomenon ("hot
flashes") of menopause.32
Conclusion
We found that basal hand blood flow is reduced in
women. This appears to be due to a basal increase in
sympathetic tone. Furthermore, we describe a paradoxical neurogenic vasodilation to mental arithmetic
and deep inspiration that is unmasked at high levels
of sympathetic tone. The gender differences in control of hand blood flow may account for the increased
incidence of Raynaud's disease in young women.
References
1. Coffinan JD: Raynaud's Phenomenon. Oxford, Oxford University Press, 1989
2. Hines EA, Christensen NA: Raynaud's disease among men.
JAM4 1945;129:1
3. Shepherd JT: Measurement of blood flow in the extremities of
man, in Walters W (ed): Lewis-Walters Practice of Surgery, Vol
XI. Hagerstown, Md, WF Prior, Inc, 1964, pp 71-77
4. Johnson JM, Taylor WF, Shepherd AP, Park MK: LaserDoppler measurement of skin blood flow: Comparison with
plethysmography. JAppl Physiol 1984;56(Respirat Environ Exer
Physiol):798-803
5. Zitnik RS, Ambrosioni E, Shepherd JT: Effect of temperature
on cutaneous venomotor reflexes in man. J Appl Physiol
1971;31:507-512
6. Cooke JP: Alpha adrenergic receptors in vascular smooth
muscle: Characterization of subtypes and modulation of
response by alteration in temperature and calcium availability
(thesis). Rochester, Minn, Mayo Graduate School of Medicine
7. Hokfelt T, Johansson 0, Ljungdahl A, Lundberg JM,
Schultzberg M: Peptidergic neurones. Nature 1980;284:515-521
8. Flavahan MA, Vanhoutte PM: Sympathetic purinergic vasoconstriction and thermosensitivity in a canine cutaneous vein.
J Phartnacol Exp Ther 1986;239:784-789
9. Cohen RA: Platelet-induced neurogenic coronary contractions due to accumulation of the false neurotransmitter,
5-hydroxytryptamine. J Clin Invest 1985;75:286-292
10. Arneklo-Nobin B, Owman C: Adrenergic and serotonergic
mechanisms in human hand arteries and veins studied by
fluorescence histochemistry and in vitro pharmacology. Blood
Vessels 1985;22:1-12
1615
11. Coffman JD, Cohen RA: Serotonergic vasoconstriction in
human fingers during reflex sympathetic response to cooling.
Am J Physiol 1988;254(Heart Circ Physiol 23):H889-H893
12. Roddie IC, Shepherd JT: The blood flow through the hand
during local heating, release of sympathetic vasomotor tone by
indirect heating, and a combination of both. J Physiol (Lond)
1956;131:657-664
13. Suko J: The effect of temperature on calcium uptake and
calcium activated ATP hydrolysis by cardiac sarcoplasmic
reticulum. Experientia 1973;29:396
14. Somlyo AP, Devine CE, Somlyo AV, North SR: Sarcoplasmic
reticulum and the temperature dependent contraction of
smooth muscle in calcium-free solutions. J Cell Biol 1971;
51:722-741
15. Vanhoutte PM, Verbeuren TJ: Depression by local cooling of
3H-norepinephrine release evoked by nerve stimulation in
cutaneous veins. Blood Vessels 1976;13:92
16. Brimijoin S: Stop-flow: A new technique for measuring axonal
transport, and its application to the transport of dopamine-bhydroxylase. J Neurobiol 1975;6:379
17. Janssens WJ, Vanhoutte PM: Instantaneous changes of alphaadrenoceptor affinity caused by moderate cooling in canine
cutaneous veins. Am J Physiol 1978;3(suppl 4):H330
18. Cooke JP, Shepherd JT, Vanhoutte PM: The effect of warming on adrenergic neurotransmission in canine cutaneous vein.
Circ Res 1984;54:547-553
19. Vanhoutte PM, Cooke JP, Lindblad L-E, Shepherd JT, Flavahan NA: Modulation of postjunctional alpha-adrenergic
responsiveness by local changes in temperature. Clin Sci
1985;68(suppl 10):121s-123s
20. Webb RC, Rusch NJ, Vanhoutte PM: Influence of sex difference and oral contraceptives on forearm reactive hyperemia.
Blood Vessels 1981;18:161-170
21. Freedman RR, Savharwal SC, Desai N: Sex differences in
peripheral vascular adrenergic receptors. Circ Res 1987;
61:581-585
22. Halperin JL, Cohen RA, Coffman JD: Digital vasodilatation
during mental stress in patients with Raynaud's disease.
Cardiovasc Res 1983;17:671-677
23. Blumberg H, Wallin BG: Direct evidence of neurally mediated
vasodilatation in hairy skin of the human foot. J Physiol
1987;382:105-121
24. Brum JM, Bove AA, Sufan Q, Reilly W, Go V[LW: Action and
localization of vasoactive intestinal peptide in the coronary
circulation: Evidence for nonadrenergic, noncholinergic coronary regulation. JAm Coll Cardiol 1986;7:406-413
25. Oberle J, Elam M, Karlsson T, Wallin BG: Temperaturedependent interaction between vasoconstrictor and vasodilator mechanisms in human skin. Acta Physiol Scand 1988;
132:459-469
26. Greenfield ADM, Shepherd JT, Whelan RF: Cold vasoconstriction and vasodilation. Irish J Med Sci 1951;309:415-419
27. Rusch NJ, Shepherd JT, Vanhoutte PM: The effect of profound cooling on adrenergic neurotransmission in canine
cutaneous veins. J Physiol (Lond) 1981;311:57-65
28. Shepherd JT, Vanhoutte PM: Cold vasoconstriction and cold
vasodilation, in Vanhoutte PM, Leusen I (eds). Vasodilation.
New York, Raven Press, 1981, pp 263-271
29. Gardner CA, Webb RC: Cold-induced vasodilation in isolated
perfused rat tail artery. Am J Physiol 1986;25:H176-H181
30. Bollinger A, Schlumpf M: Finger blood flow in healthy subjects of different age and sex and in patients with primary
Raynaud's disease. Acta Chir Scand (Suppl) 1976;465:42-47
31. Gifford RW, Hines EA Jr: Raynaud's disease among women
and girls. Circulation 1951;16:1012-1021
32. Kronenberg F, Cote LJ, Linkie DM, Dyrenfurth I, Downey
JA: Menopausal hot flashes: Thermoregulatory, cardiovascular, and circulating catecholamine and LH changes. Maturitas
1984;6:31-43
KEY WORDS * thermoregulation
vasospasm * autonomic control
*
Raynaud's disease
Sex differences in control of cutaneous blood flow.
J P Cooke, M A Creager, P J Osmundson and J T Shepherd
Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016
Circulation. 1990;82:1607-1615
doi: 10.1161/01.CIR.82.5.1607
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1990 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/82/5/1607
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/