Analysis of Creatine Kinase,CK-MB, Myoglobin, and Troponin T
advertisement

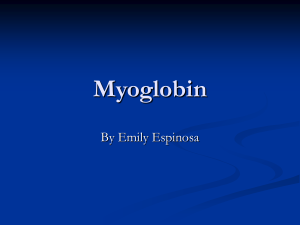
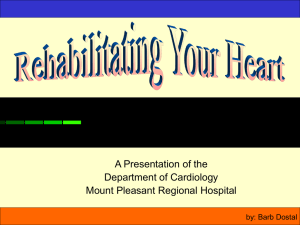
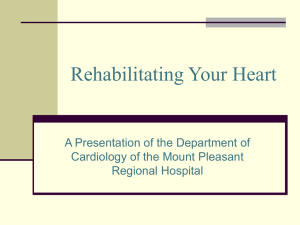
1542 Analysis of Creatine Kinase, CK-MB, Myoglobin, and Troponin T Time-Activit Curves for Early Assessment of Coronary Artery Reperfusion After Intravenous Thrombolysis Markus Zabel, MD; Stefan H. Hohnloser, MD; Wolfgang Koster, MD; Martina Prinz, MD; Wolfgang Kasper, MD; and Hanjorg Just, MD Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 Background. Thrombolysis has become the standard therapeutic approach in patients with acute myocardial infarction. To identify patients who may benefit from early invasive procedures, reliable noninvasive assessment of success or failure of thrombolytic therapy is mandatory. Methods and Results. In a prospective study in 63 consecutive patients undergoing thrombolysis for their first myocardial infarction, serial measurements of creatine kinase (CK), its isoenzyme CK-MB, myoglobin, and troponin T were done to determine their value for noninvasive prediction of coronary artery patency. Blood samples were drawn every 15 minutes during the first 90 minutes, every 30 minutes during the first 4 hours, every 4 hours during the first 24 hours, and every 8 hours during the first 72 hours. The perfusion status of the infarct-related artery was assessed angiographically 90 minutes after initiation of thrombolysis. For each marker, time to its peak concentration and its early initial slope (start of thrombolysis to 90 minutes thereafter) were determined. Areas under receiver operator characteristic (ROC) curves were 0.83, 0.76, 0.82, and 0.80 for maxima of CK, CK-MB, myoglobin, and troponin T, respectively (p=NS by univariate Z test). The corresponding values for early slopes of CK, CK-MB, myoglobin, and troponin T were 0.79, 0.82, 0.89, and 0.80 (p =0.23 for comparison between myoglobin and CK-MB;p=0.07 between myoglobin and CK). Sensitivity, specificity, and positive and negative predictive values regarding noninvasive prediction of coronary artery patency after 90 minutes were 80%o, 82%, 95%, and 61% for time to CK maximum; 91%, 77%, 91%, and 77% for time to myoglobin maximum; 87%, 71%, 89%o, and 67% for early CK slope; and 94%, 88%, 94%, and 82% for myoglobin slope, respectively. When myoglobin slope was assessed together with other clinical reperfusion markers (resolution of chest pain or ST segment elevation, occurrence of reperfusion arrhythmias) by logistic regression analysis, only the myoglobin slope was an independent predictor of coronary artery patency (p<0.0001). Conclusions. With regard to noninvasive prediction of coronary artery patency after thrombolytic therapy, measurement of the early initial slopes of the serum markers within only 90 minutes after the initiation of therapy is as accurate as the determination of the time to their peak concentration. Compared with the other markers examined, myoglobin appears to have advantages because of its earlier rise, yielding a better negative predictive value and a higher area under the ROC curve for determination of its early initial slopes. (Circulation 1993;87:1542-1550) KEY WORDs * myocardial infarction, acute * thrombolysis * reperfusion T he value of coronary artery reperfusion by means of intravenous thrombolysis in patients with evolving myocardial infarction has been rigorously evaluated.'-4 An impressive improvement in survival rates has been demonstrated in patients with successful reopening of the infarct-related artery. In addition, left ventricular function has been shown to be superior in patients treated with thrombolysis compared with placebo-treated patients.5 It is evident from both From the University Hospital, Department of Cardiology and Department of Clinical Chemistry (W.K.), Freiburg, Germany. Supported by a grant from the Deutsche Gesellschaft fur Herzund Kreislaufforschung, Bad Nauheim, Germany (M.Z.). Address for correspondence: Stefan H. Hohnloser, MD, University Hospital, Department of Cardiology, Hugstetter Str. 55, 7800 Freiburg, FRG. Received June 15, 1992; revision accepted January 14, 1993. laboratory and clinical studies that the benefits of thrombolytic therapy are conferred by restoration of patency of the infarct-related artery.6-9 Recently, Abbottsmith and coworkers10 have reported that salvage angioplasty after failed thrombolysis improves outcome in these patients. Thus, invasive means are valuable in selected patients to establish coronary artery patency.11,2 Rescue thrombolysis with readministration of the same or a different thrombolytic agent may also have a role after failed initial thrombolytic therapy.13 On the other hand, acute routine angiography in all patients receiving thrombolytic therapy for acute infarction is unnecessary and may eventually cause harm to some.14-16 Hence, reliable methods other than angiography are needed to detect coronary reperfusion early during the hospital course. In previous studies, the normalization of ST segment elevation in the surface Zabel et al Serum Markers for Prediction of Reperfusion Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 ECG,17-21 the occurrence of reperfusion arrhythmias,19,22-24 the resolution of infarct-related chest pain,25,26 and various cardiac enzymes have been used for this purpose. For example, a short time to peak creatine kinase (CK)27 or CK-MB concentration28,29 has been proposed as an indicator of reperfusion. More recently, new serum markers such as myoglobin,28'30 CK-MB isoforms,31 and the specific cardiac antigen troponin T32 have become available and have been examined in small groups of patients with acute myocardial infarction. Up to now, however, the value of these new reperfusion markers has not been vigorously evaluated, and they have not been compared with each other in a reasonably large cohort of patients undergoing thrombolysis. The aims of the present prospective study, therefore, were 1) to develop simple indexes for success or failure of reperfusion therapy according to the initial CK and CK-MB time-activity curves and 2) to evaluate whether new reperfusion markers such as myoglobin and troponin T yield a higher diagnostic accuracy in prediction of thrombolysis-induced reopening of the infarct-related artery compared with conventional serum markers. Particular attention was paid to the question of whether analysis of early increases in enzyme or protein concentrations (within 120 minutes after start of thrombolysis) is as accurate regarding prediction of coronary artery patency as the determination of the time to their peak concentration, since this would be of marked clinical utility. Methods Patient Population Sixty-three consecutive patients with acute myocardial infarction treated with thrombolysis were studied prospectively between May 1990 and October 1991. Patients with typical chest pain of .30 minutes' duration, unresponsive to nitrates, and with ECG ST segment elevation of .0.1 mV in at least two limb leads or >0.2 mV in at least two precordial (V) leads were eligible for the study. Patients with cardiogenic shock were excluded. Thrombolytic therapy had to be initiated within 6 hours after onset of symptoms. The thrombolytic agent used was prourokinase in 32 patients combined with recombinant tissue plasminogen activator (rt-PA) in 20 patients and anisoylated plasminogen streptokinase activator complex (APSAC) in 31 patients. After thrombolysis, all patients received a bolus of 7,500 to 10,000 units of heparin followed by a continuous infusion of 1.250 units/hr for the next 72-96 hours (partial thromboplastin time adjusted to two times the upper normal). All patients gave their informed consent to the study. The usual exclusion criteria for thrombolysis were applied. Coronary Angiography Coronary angiography was performed within 90 minutes after onset of thrombolytic therapy and repeated 24 hours later. The angiographic findings were assessed according to the Thrombolysis in Myocardial Infarction (TIMI) criteria for reperfusion.4 For this purpose, the first injection of contrast was taken as the patency assessment. TIMI grades 2 and 3 were defined as coronary artery patency. For statistical analysis, early 1543 patency within the first 90 minutes was considered successful coronary artery opening. Serum Markers Blood samples (10 mL) were taken before initiation of thrombolysis, every 15 minutes for the first 90 minutes after start of therapy, every 30 minutes for the first 4 hours, every 4 hours up to 24 hours, and every 8 hours up to 72 hours. The samples were stored at room temperature to allow clotting and frozen at -20°C after centrifugation until analysis. Samples were analyzed by investigators who were unaware of the angiographic results. Plasma total CK activity was assayed according to the method of Rosalki.33 The mass of the CK-MB isoenzyme was determined by means of a rapid fluorometric enzyme immunoassay based on a two-site sandwich immunoassay methodology (Baxter Stratus, Miami, Fla.).34 Units are given in nanograms per milliliter. Myoglobin was determined nephelometrically by a quantitative latex agglutination test developed from an earlier-described semiquantitative test (Behring Werke, Marburg, Germany).35 Assay times are 15-30 minutes. The test was validated against the commonly used radioimmunoassay determination of myoglobin30 (Behring Werke; data on file). Troponin T was measured with a recently developed enzyme immunoassay (Bohringer Mannheim, Germany) that has been described in detail elsewhere.3236,37 The upper limits of the normal range were 70 units/L for creatine kinase, 5.6 ng/mL for CK-MB (mass), 85 ng/mL for myoglobin, and 0.2 ng/mL for troponin T. For each of these serum markers, time to peak concentration after start of therapy was calculated. In addition, the slope of each serum marker within the first 90 minutes was calculated and expressed in units per liter per hour or nanograms per milliliter per hour by dividing the difference of the corresponding values at initiation of therapy and 90 minutes thereafter by 1.5. In Figure 1, raw data from a patient with successful reperfusion and from another without reperfusion are shown to illustrate the technique of slope determinations. Clinical Reperfusion Markers Resolution of maximal ST segment elevation was judged from two surface ECGs taken before and 120 minutes after start of thrombolysis. In addition, Holter monitoring was started before injection of the thrombolytic agent for assessment of reperfusion arrhythmias within the first 90 minutes. Accelerated idioventricular rhythm (AIVR) was defined by a heart rate of < 100 beats per minute, a long coupling interval, a regular configuration and rate, and termination by sinus escape. Sinus bradycardia was defined by a heart rate of <55 beats per minute. Patients were also interviewed for the severity of chest pain on a subjective scale ranging from 0 to 10 before and 90 minutes after thrombolysis. Statistical Methods Values are given as mean±+SD. The calculation of sensitivity, specificity, positive predictive value, and negative predictive value was performed according to the formulas described in our previous report.19 A x2 test was used to test the univariate correlation of noninvasive markers to patency of the infarct artery as well as differences of numerical parameters between Circulation Vol 87, No S May 1993 1544 CK (U/ll 3000 - _~ 2750 2500 2250 2000 1750 1500 1250 1000 ; 750 500 250 0 t t Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 FIGURE 1. Graphs showing raw data from two representative patients with (TIMI grade 3) and without (TIMI grade 0) successful thrombolysisinduced reperfusion. Upper panel: Creatine kinase (CK) values. Lower panel: Myoglobin (Myo) values. The two arrows indicate the points of time used for determination of the early slopes in CK and myoglobin concentration increases (90-minute value minus 0-minute value divided by 1.5). Minutes after sart of thrombolysis Myo [nglmq 5500 - 5000. 4500 4000 3500 3000 2500 2000 1500 1000 500 _ Ad 0 30 60 90 120 150 180 210 240 400 800 1200 1 60 2000 2400 2800 3200 Minutes after start of thronmbolysis Linear regression analysis was performed for related parameters, and coefficients of correlations were calculated and tested for significance. The independent correlation of serum and clinical markers to coronary artery patency was determined by means of logistic regression analysis with coronary artery patency as the outcome variable. Markers were entered as categorical variables (positive or negative) by use of their respective cutoff values (see below). For statistical purposes, the following definitions of positive reperfusion markers were applied. According to two previous studies at our institution,19,38 a maximum of CK activity within the first 12 hours after start of thrombolysis was prospectively defined as a positive marker of coronary artery patency. For the CK slope, a cutoff of 40 units. L`. hr-' was prospectively derived from the report of Lewis et al.39 As reported by Hogg et al17 and a previous study from our institution,'9 a positive ST marker was defined as a reduction of ST segment elevation of 250%. With respect to pain score, a decrease of at least two points was considered suggestive of reperfusion.26 AIVR19,23 and sinus bradycardia <55 beats per minute19,22 within the first 90 minutes (only in patients with inferior infarctions) were prospectively defined as reperfusion arrhythmias. The cutoffs groups. for the time to peak CK-MB, myoglobin, and troponin T retrospectively defined at 10, 3, and 15 hours after start of thrombolysis, respectively, since no previously described cutoff values were available from the literature. Accordingly, the cutoffs for the absolute rise of each marker over the first 90 minutes of therapy were chosen as 10, 150, and 0.2 ng* mL-'* hr-' for CK-MB, myoglobin, and troponin T, respectively. To allow comparison with the CK data, these numbers were chosen to represent similarly good but not optimal cutoffs. Since potential bias concerning the choice of a single cutoff cannot be excluded (even if prospectively defined), sensitivity and specificity data are represented over the entire cutoff range in the applicable figure (Figure 2). Furthermore, receiver operator characteristic (ROC) curve analysis as an objective means for determination of the utility of the various markers for noninvasive prediction of coronary artery patency was applied. The major advantage of this technique is provided by its independence of definitions of cutoff values. This statistical method was initially developed in the field of signal detection theory and provides a powerful tool to assess the predictive quality of a given test.40-42 With this technique, sensitivity (true positives) is plotted against 1-specificity (true negatives) for the possible were Zabel et al Serum Markers for Prediction of Reperfusion CKMB maximum [cutoff In hi CK maximum [cutoff in hi lolp 4~ *w~ lone lvv- *-^ a^^- Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 so 80 60 60 40 40 20 20 0 100 200 300 r _ 000 400 1545 600 700 800 40 20 M CK slope 0-90 min [cutoff In U/l/hi - - - 426 100 12 14 80 120 140 60 100 160 CKMB slope 0-90 min [cutoff in ng/mil/hl 100 [%] D m m % 80 60 40 20'ff -- n 4 10 6 12 14 H v 0 10 Myoglobin maximum [cutoff in hi 20 30 40 60 Do-0 600 1000 Myoglobin '- 1600 slope sensitivity 2000 2600 70 60 Troponin T maximum Icutoff in hi 3000 3600 0 Icutoff in ng/mil/hl ---rf 2 4 6 8 10 12 14 Troponin T slope Icutoff in ng/ml/hl --& + specificity sensitivity + specificity FIGURE 2. Graphs. PanelsA: Sensitivity and specificityforprediction of coronary artery patency at various cutoffpoints for time to creatine kinase (CK) maximum and of CK slopes for the first 90 minutes after initiation of thrombolysis. Panels B: CK-MB maximum and slope. Panels C: Myoglobin maximum and slope. Panels D: Troponin T maximum and slope. range of cutoff points of a specific marker.40-42 The area under the ROC curve represents a single number for the predictive quality of the test, with a maximum of 1.0 representing an ideal test (100% accuracy) compared with an area of 0.5 indicating that the test is no better than chance.40-42 Thus, ROC curve analysis yields a single value for each marker evaluated. To compare the different areas under the ROC curves of several markers (i.e., to compare the predictive quality of tests), a univariate Z-test has been described in detail by Hanley and McNeil.41 Significance was considered at a value of pS0.05. 1546 Circulation Vol 87, No S May 1993 TABLE 1. Sensitivity, Specificity, Positive and Negative Predictive Values, Univariate x2, and Area of ROC Curve for Noninvasive Prediction of Coronary Patency by Means of Peak and Slope Analysis of Various Serum Markers Negative Positive Area under predictive predictive Specificity Sensitivity ROC curve value (%) value (%) (%) (%) Marker X2 18.5 0.83 61 95 82 80 Time to CK maximum 17.4 0.79 87 71 67 89 CK slope Time to CK-MB 8.5 0.76 52 86 78 65 maximum 71 15.5 0.79 63 85 96 CK-MB slope Time to myoglobin 25.6 0.82 77 77 91 91 maximum 94 88 94 82 36.7 0.89 Myoglobin slope Time to troponin T 74 71 8.6 0.80 50 87 maximum 80 65 9.7 0.80 55 93 Troponin T slope ROC, receiver operator characteristics; CK, creatine kinase. Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 Results paper. Four patients had to be defibrillated within the first hours because of the occurrence of ventricular fibrillation, and one other patient had femoral bleeding consequent to angiography. Since the overall predictive value of the markers examined was not significantly influenced by the data of these five patients, they were included in the analysis. Clinical Data Sixty-three consecutive patients were included in the protocol. There were 54 men and nine women with a mean age of 59±11 years (range, 33-81 years). Twentyeight patients suffered from anterior and 35 from inferior myocardial infarction. Angiography revealed the left anterior descending coronary artery in 26, the right coronary artery in 32, and the circumflex artery in five patients as the corresponding infarct-related artery. The time interval from onset of chest pain to start of thrombolysis averaged 190±112 minutes. In 46 patients (73%), angiography revealed TIMI grade 2 or 3 reperfusion of the infarct-related vessel at 90 minutes. In the remaining 17 patients, the infarct-related artery was found to be occluded (TIMI grade 0 or 1). Late reperfusion of the infarct vessel between 90 minutes and 24 hours occurred in 10 patients, whereas two patients had reocclusion within this time frame. Among the 17 patients with an occluded vessel on the first coronary angiogram, late reperfusion (within 24 hours) did not Analysis of CK The mean peak CK value was 1,041±686 units/L for patients with a patent versus 942±758 units/L for patients with an occluded infarct artery (p=NS). Time to peak concentration averaged 9.0±6.2 hours in patients with versus 17.1±6.4 hours for patients without coronary artery patency (p<0.001). Sensitivity and specificity for prediction of vessel patency at the chosen cutoff were 80% and 82%, respectively, and they were comparable for a range of cutoffs between 10 and 15 hours (Figure 2, Table 1). This resulted in a high area under the ROC curve of 0.83 and a univariate x2 of 18.5 (Figure 3). For the initial CK slope between 0 and 90 minutes after start of therapy, sensitivity and specificity were almost comparable at 87% and 71%, respectively (Figure 1 and Table 1). Accordingly, ROC curve area significantly influence the time elapsed to peak concentrations of the various serum markers. Thus, these patients are referred to as one group throughout the Slopes 0 - 90 min Time to Peak 100 60 0 60 .0 *~~~~~~~~~~.A C KMB(mass) Myogiobin 40 40 20 20 00 0 *Troponin 04 20 40 60 1-Specificity 1%1 80 100 0 20 40 60 80 T 100 1-Specificity l[l FIGURE 3. Receiver operator characteristic (ROC) curves for noninvasive prediction of coronary artery patency by means ofpeak and slope measurements of creatine kinase (CK), CK-MB, myoglobin, and troponin T (n=63). 1547 Zabel et al Serum Markers for Prediction of Reperfusion and x2 were slightly lower, at 0.79 and 17.4 (Table 1). The optimal range of cutoffs was between 40 and 80 units * - hr-t (Figure 2). An inverse correlation was found between CK slope and maximum (r= -0.40, p<O.0Ol). Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 Analysis of CK-MB Mass Peak CK-MB averaged 216±151 ng/mL for patients with a patent versus 167±130 units/L for patients with an occluded infarct artery (p=NS). Time to peak was similar to that of CK and averaged 7.5±4.1 hours in patients with versus 12.0±5.3 hours for patients without coronary artery patency (p=0.004). Sensitivity and specificity for prediction of vessel patency at the chosen cutoff of 10 hours were 78% and 65% for CK-MB maximum, respectively. The best range of cutoffs was 8.5-12 hours. For the slope of CK-MB, the range of acceptable cutoffs was 15-20 ng . mL` * hr-1 (Figure 2 and Table 1). ROC curve analysis disclosed values of 0.76 for CK-MB maximum and 0.79 for CK-MB slope. Analysis of Myoglobin Myoglobin peaked after 2.1±2.8 hours in patients with successful (peak value, 2,361±1,824 ng/mL) compared with 4.9±4.2 hours (p<0.02) in patients with failed reperfusion (peak value, 1,037±1,137 ng/mL, p=0.001). Sensitivity was 91% together with a specificity of 77% at the predefined cutoff of 3 hours. For the myoglobin slope, a sensitivity of 94% and specificity of 88% at the preselected cutoff of 150 ng. mL- . hr-1 were obtained (Figure 2). ROC curve area was comparable to the other markers for myoglobin maximum at 0.82; however, the univariate X2 value was highest of all maxima with 25.6. Myoglobin slope revealed the highest ROC curve area and univariate x2 value of all studied markers (ROC, 0.89; X2=36.7) (Figure 3, Table 1). There was an inverse correlation between myoglobin slope and maximum (r=-0.35,p<0.01). Analysis of Troponin T Troponin T peaked after 11.6±9.3 hours in patients with successful reperfusion (peak value, 23.6±18.8 ng/ mL) compared with 20.3±14.4 hours (p=0.03) in patients without reperfusion (peak value, 10.1±6.3 ng/mL; p<0.001). Sensitivity and specificity were 74% and 71%, respectively, at the preselected cutoff of 15 hours, with a narrow range of favorable cutoffs between 14 and 16 hours (Figure 2). This range was also narrow for the analysis of troponin T slopes, for which sensitivity was 80% at a specificity of only 65% for the predefined cutoff of 0.2 ng * mL- * hr-1. ROC curve areas were 0.80 for both maximum and slope analysis of troponin T (Figure 3, Table 1). Univariate X2 values were low, with 8.6 for troponin maximum and 9.7 for troponin slope. Comparison of Serodiagnostic Markers The ROC curves of the four serum markers were plotted to compare the value of each serum marker regarding noninvasive prediction of reperfusion. Analysis of time to peak concentration revealed similar values for all four markers evaluated. Comparison of early slopes demonstrated the highest ROC area for analysis of myoglobin (Figure 3, Table 1). The difference in ROC areas between myoglobin and CK was close to significance (p=O0.07), whereas the difference in 25r E E 20 F x X a .0 0 2 15k r * 0.59 p c 0.001 y * 0.28x - 0.33 0 10F O F 6 0 01 ~~~~~~~~-0 ~~ E- 0 5 0 0 :11 ~ O on 15 10 20 E80 2 E I.E E1 25 30 366 25 30 35 0 T70 B0 r * 0.59 p 0.001 950 y *0.95x +3.3 40 A c CL 0 so~ 30- 111 2 0 -._ 20 11 ~~~~~ 0 -~~~~~~~~~ 10 d 10n 0 5 20 16 10 Time to CK maximum Ih] FIGURE 4. Upper panel: Plot of time to creatine kinase (CK) maximum vs. time to myoglobin maximum. Lower panel: Plot of time to CK maximum versus time to troponin T maximum. CK-MB slope was not significant (p=0.23). As demonstrated in Figure 4, regression analysis disclosed a significant correlation between time to myoglobin and CK maximum and between time to troponin T and CK maximum (r=0.59 for both correlations). With respect to the time-activity curves, analyses of CK, CK-MB, and troponin T were comparable, revealing pathological findings in approximately 60-65% of patients at 60 minutes and in 90% at 120 minutes after the initiation of thrombolysis (Figure 5). The release of myoglobin, however, occurred significantly earlier, resulting in abnormal findings in 77% of patients as early as 30 120 60 Imin after CK -C- GKMB thrombolyasil -* Troponin T Myoglobin FIGURE 5. Graph showing percentage of patients (pts) with abnormal values of various serum markers according to time from initiation of thrombolysis (*p<0.05 between myoglobin and creatine kinase [CK]-MB for 0-60 minutes and between myoglobin and CK for 90 and 120 minutes; **p<0.01 between myoglobin and CKfor 0-60 minutes). 1548 Circulation Vol 87, No S May 1993 TABLE 2. Sensitivity, Specificity, Positive and Negative Predictive Values, Univariate x2, and Area Under the ROC Curve for Noninvasive Prediction of Coronary Patency by Means of Clinical Markers Negative Positive Area under predictive predictive Specificity Sensitivity ROC curve value (%) value (%) (%) (%) Marker X2 41 96 ... 94 8.4 50 Reperfusion arrhythmias 0.74 9.7 42 83 71 76 ST segment reduction 0.67 2.7* 47 79 41 83 Reduction in pain score ROC, receiver operator characteristics. See text for details. *p=NS. minutes and 91% at 60 minutes after start of therapy (Figure 5). Comparison With Other Clinical Reperfusion Markers Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 Table 2 demonstrates that resolution of ST segment elevation and the occurrence of reperfusion arrhythmias were also predictors of coronary artery patency. The calculated x2 values indicate that both markers were comparable to those serum markers with the lowest predictive values for coronary artery patency (Tables 1 and 2). ROC curve analysis for ST segment resolution resulted in an area under the ROC curve of 0.74 (versus 0.79 for CK slope, p=NS; versus 0.89 for myoglobin slope, p<0.02). Because of the lack of variable cutoffs with respect to reperfusion arrhythmias, ROC curve analysis cannot be performed for this marker. The chest pain score did not yield statistically significant prediction of the reperfusion status (Table 2). When myoglobin slope was assessed together with other clinical markers by means of logistic regression analysis, only the myoglobin slope was an independent predictor of coronary artery patency (p<0.0001). The probability values for the other markers examined were 0.10 for the occurrence of reperfusion arrhythmias, 0.13 for ST segment resolution, and 0.28 for resolution of chest pain. Discussion The present study indicates that noninvasive prediction of coronary artery patency after thrombolytic therapy in patients with acute myocardial infarction is possible by assessment of time-activity curves of serum markers. Of particular clinical importance is the observation that analysis of the initial slopes of activity curves over the first 90 minutes after initiation of thrombolysis yields the same and for myoglobin even better predictive accuracy than the determination of the time to peak concentration of each marker. Decision making as to further invasive procedures can be improved by use of analysis of these early slopes in a substantial proportion of patients. This allows early mechanical interventions such as salvage angioplasty in selected individuals in whom the infarct-related artery remains occluded after thrombolysis. It has been demonstrated that these patients benefit from invasive interventions,11,12 whereas routine coronary angiography is unnecessary and may even be harmful to some individuals.14-'6 In previous studies from our institution as well as from others, a short time to peak CK or CK-MB concentration has been proposed as an indicator of successful thrombolysis-induced coronary artery reperfusion.19'27-29 Only two studies so far have aimed to examine the usefulness of the initial slopes of timeactivity curves of the two serum markers CK and CK-MB concerning assessment of coronary artery patency.29'39 These investigators found that a rapid increase in CK and CK-MB concentrations closely reflected angiographic documentation of reperfusion. However, ROC characteristics were not reported. Other newly developed serum markers such as CK-MB isoforms31 or the specific cardiac antigen troponin T32 have also been examined with respect to their utility as indicators of coronary reperfusion. Puleo and Perryman31 analyzed peaks of MB2/MB, subform ratios in 33 patients undergoing thrombolysis and found this ratio helpful for assessment of coronary artery patency within 2 hours after start of therapy. However, their study appears to be limited by the small number of patients undergoing thrombolytic therapy and by the fact that coronary angiography was performed as late as 5 days after thrombolysis. Katus et a132 studied the value of the new cardiac antigen troponin T in 57 patients and showed that troponin T peaks significantly earlier if the infarct-related artery is successfully reperfused. However, cutoff values and initial slopes were not specifically assessed in this study. To the best of our knowledge, the present study is the first to compare the serum markers CK, CK-MB, myoglobin, and troponin T systematically regarding their value for noninvasive prediction of reperfusion. Of all markers examined, myoglobin appears to exhibit several advantages that make this protein particularly suitable for early noninvasive prediction of patency of the infarct-related vessel. First, comparison of the ROC curve characteristics revealed that analysis of the initial myoglobin concentration increase allows the best overall prediction of success or failure of thrombolytic therapy of all studied markers for analysis of both time to peak and early slopes. Although the differences between the ROC areas were small, the difference between myoglobin and CK approached significance (p=0.07), indicating potential clinical importance. Furthermore, the highest univariate X2 values were also obtained for both myoglobin slope and time to peak concentration. This also resulted in high sensitivity and positive predictive value for prediction of coronary artery patency. Additionally, the negative predictive value and specificity, which reflect identification of patients with occluded vessels, were quite high at 82% and 88%, respectively, numbers that are not reached by the other markers examined. Second, as already mentioned, quantitative nephelometric analysis of myoglobin, which has been validated against the radioimmunoassay used by Ellis et al,30 provides laboratory results after a short turnover time of only 15-30 minutes. Furthermore, an even more Zabel et al Serum Markers for Prediction of Reperfusion Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 rapid assay using turbidimetry has recently been introduced into clinical practice.4344 Third, myoglobin concentration exhibited the earliest rise of all serum markers examined after initiation of therapy. Although the purpose of the present investigation was not to examine the accuracy of serum markers with respect to diagnosis of myocardial infarction but rather the efficacy of thrombolysis, this protein may offer an additional diagnostic advantage. The usefulness of myoglobin for noninvasive prediction of infarct-artery patency has recently been confirmed by other investigators.45 However, Clemmensen and coworkers45 reported no comparison with other serodiagnostic markers in their study. In the present investigation, CK maximum and CK-MB maximum yielded relatively good diagnostic information regarding coronary artery patency as well. However, compared with the time elapsed to reach peak myoglobin levels, it took four to five times as long to reach maximal concentrations of these enzymes. This time frame would therefore significantly reduce the chances to salvage jeopardized myocardium by means of invasive procedures. It has been shown previously that combined analysis of noninvasive markers (i.e., peak CK, resolution of ST segment elevation, occurrence of reperfusion arrhythmias) can improve assessment of success or failure of thrombolytic therapy.19 In the present study, other clinical reperfusion markers did not add significantly to the predictive power of myoglobin slope analysis, indicating the particular strength of this marker. According to the results of the present study, troponin T offers no advantages for noninvasive prediction of coronary reperfusion in patients undergoing thrombolysis (Table 1). However, troponin T analysis was helpful in the four patients suffering from ventricular fibrillation. In these patients, CK values were distorted by the enzyme release from skeletal muscles caused by the defibrillation shock, whereas troponin T levels were not affected because of the high specificity of this marker for myocardial tissue.36 Clinical Implications The present study demonstrates that analysis of the early initial rise of several serum markers is as accurate as determination of the time elapsed to reach their peak concentration with respect to noninvasive prediction of success or failure of thrombolysis in patients with acute infarction. This allows early noninvasive prediction of coronary artery patency in the majority of patients within the first 2 hours after initiation of thrombolytic therapy. These time limits allow for measures such as rescue angioplasty that aim to salvage myocardium. Early slope analysis of myoglobin appears to be superior to the other serum markers examined and, in addition, exhibits the most rapid concentration increase of all markers evaluated. References 1. Gruppo Italiano per lo Studio della Streptochinasi nell'Infarto Miocardico (GISSI): Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Lancet 1986;1:397-402 2. Wilcox RG, von der Lippe G, Olson CG, Jensen G, Skeine AM, Hampton JR: Trial of tissue plasminogen activator for mortality reduction in acute myocardial infarction The Anglo-Scandinavian Study of Early Thrombolysis (ASSET). Lancet 1988;2:525-530 1549 3. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17187 cases of suspected acute myocardial infarction. Lancet 1988;2:349-360 4. The Thrombolysis in Myocardial Infarction (TIMI) Study Group: The thrombolysis in myocardial infarction (TIMI) trial. N Engl J Med 1985;312:932-936 5. White HD, Norris RM, Brown MA, Takayama M, Maslowski A, Bass NM, Ormiston JA, Whitlock T: Effect of intravenous streptokinase on left ventricular function and early survival after acute myocardial infarction. N Engi J Med 1987;317:850-855 6. Tiefenbrunn AJ, Sobel BE: Invited review: Thrombolysis and myocardial infarction. Fibrinolysis 1991;5:1-15 7. Kennedy JW, Ritchie JL, Davis KB, Stadius ML, Maynard C, Fritz JK: The Western Washington randomized trial of intracoronary streptokinase in acute myocardial infarction. N Engl J Med 1985; 312:1073-1078 8. Califf RM, Topol EJ, George BS, Kereiakes DJ, Aronson LG, Lee KL, Martin L, Candela R, Abottsmith C, O'Neill WW, Stack RS, and the TAMI study group: One-year outcome after therapy with tissue plasminogen activator: Report from the Thrombolysis and Angioplasty in Myocardial Infarction trial. Am Heart J 1990;119: 777-785 9. Stack RS, O'Connor CM, Mark DB, Hinohara T, Phillips HR, Lee M, Ramirez NM, O'Callaghan WG, Simonton CA, Carlson EB, Morris KG, Behar VS, Kong Y, Peter RH, Califf RM: Coronary perfusion during acute myocardial infarction with a combined therapy of coronary angioplasty and high-dose intravenous streptokinase. Circulation 1988;77:151-161 10. Abbottsmith CW, Topol EJ, George BS, Stack RS, Kereiakes DJ, Candela RJ, Anderson LC, Harrelson-Woodlief SL, Califf RM: Fate of patients with acute myocardial infarction with patency of the infarct-related vessel achieved with successful thrombolysis versus rescue angioplasty. JAm Coll Cardiol 1990;16:770-778 11. Topol EJ: Mechanical interventions for acute myocardial infarction, in Topol EJ (ed): Textbook of Interventional Cardiology. Philadelphia, Pa, WB Saunders Co, 1990, pp 269-299 12. Muller DWM, Topol EJ: Thrombolytic therapy: Adjuvant mechanical intervention for acute myocardial infarction. Am J Cardiol 1992;69:60A-70A 13. White HD, Cross DB, Norris RM, Williams BF: Early infarct artery patency after intravenous streptokinase, intracoronary contrast and intracoronary rt-PA. (abstract) JAm Coll Cardiol 1992; 19(suppl A):275A 14. Topol EJ, Califf RM, George BS, Kereiakes DJ, Abbottsmith CW, Candela RJ, Lee KL, Pitt B, Stack RS, O'Neill WW, and the TAMI study group: A randomized trial of immediate versus delayed elective angioplasty after intravenous tissue plasminogen activator in acute myocardial infarction. N Engl J Med 1987;317: 581-588 15. The TIMI Research Group: Immediate versus delayed catheterization and angioplasty following thrombolytic therapy for acute myocardial infarction. JAMA 1988;260:2849-2858 16. Simoons ML, Arnold AER, Betriu A, de Bono DP, Col J, Dougherty FC, Essen RV, Lambertz H, Lubsen J, Meier B, Michel PL, Raynaud P, Rutsch W, Sanz GA, Schmidt W, Serruys P, Thery C, Uebis R, Vahanian A, van de Werf F, Willems GM, Wood D, Verstraete M: Thrombolysis with tissue plasminogen activator in acute myocardial infarction: No additional benefit from immediate percutaneous coronary angioplasty. Lancet 1988;1:197-202 17. Hogg KJ, Hornung RS, Howie CA, Hockings N, Dunn FG, Hillis WS: Electrocardiographic prediction of coronary artery patency after thrombolytic treatment in acute myocardial infarction: Use of the ST segment as a noninvasive marker. Br Heart J 1988;60: 275-280 18. Krucoff MW, Green CE, Satler LF, Miller FC, Pallas RS, Kent KM, del Negro AA, Pearle DL, Fletcher RD, Rackley CE: Noninvasive detection of coronary artery patency using continuous ST-segment monitoring. Am J Cardiol 1986;57:916-922 19. Hohnloser SH, Zabel M, Kasper W, Meinertz T, Just H: Assessment of coronary artery patency after thrombolytic therapy: Accurate prediction utilizing the combined analysis of three noninvasive markers. JAm Coll Cardiol 1991;18:44-49 20. Saran RK, Been M, Furniss SS, Hawkins T, Reid DS: Reduction in ST-segment elevation after thrombolysis predicts either coronary reperfusion or preservation of left ventricular function. Br Heart J 1990;64:113-117 21. Clemmensen P, Ohman EM, Sevilla D, Peck S, Wagner NB, Quigley PS, Grande P, Lee KL, Wagner GS: Changes in standard electrocardiographic ST-segment elevation predictive of successful 1550 22. 23. 24. 25. 26. 27. Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 28. 29. 30. 31. 32. Circulation Vol 87, No S May 1993 reperfusion in acute myocardial infarction. Am J Cardiol 1990;66: 1407-1411 Gore JM, Ball SP, Corrao JM, Goldberg RJ: Arrhythmias in the assessment of coronary artery reperfusion following thrombolytic therapy. Chest 1988;94:727-730 Gorgels APM, Vos MA, Letsch IS, Verschuuren EA, Bar FWHM, Jannsen JHA, Wellens HJJ: Usefulness of the accelerated idioventricular rhythm as a marker for myocardial necrosis and reperfusion during thrombolytic therapy in acute myocardial infarction. Am J Cardiol 1988;61:231-235 Miller FC, Krucoff MW, Satler LF, Green CE, Fletcher RD, del Negro AA, Pearle DL, Kent KM, Rackley CE: Ventricular arrhythmias during reperfusion. Am Heart J 1986;112:928-932 Califf RM, O'Neill W, Stack RS, Aronson L, Mark DB, Mantell S, George BS, Candela RJ, Kereiakes DJ, Abbottsmith C, Topol EJ, and the TAMI study group: Failure of simple clinical measurements to predict perfusion status after intravenous thrombolysis. Ann Intern Med 1988;108:658-662 Kircher BJ, Topol EJ, O'Neill WW, Pitt B: Prediction of infarct coronary artery recanalization after intravenous thrombolytic therapy. Am J Cardiol 1987;59:513-515 Gore JM, Roberts R, Ball SP, Montero A, Goldberg RJ, Dalen JE: Peak creatine kinase as a measure of effectiveness of thrombolytic therapy in acute myocardial infarction. Am J Cardiol 1987;59: 1234-1238 Katus HA, Diederich KW, Scheffold T, Uellner M, Schwarz F, Kubler W: Noninvasive assessment of infarct reperfusion: The predictive power of the time to peak value of myoglobin, CKMB, and CK in serum. Eur Heart J 1988;9:619-624 Garabedian HD, Gold HK, Yasuda T, Johns JA, Finkelstein DM, Gaivin RJ, Cobbaert C, Leinbach RC, Collen D: Detection of coronary artery reperfusion with creatine kinase-MB determinations during thrombolytic therapy: Correlation with acute angiography. JAm Coll Cardiol 1987;11:729-734 Ellis AK, Little T, Zaki Masud AR, Liberman HA, Morris DC, Klocke FJ: Early noninvasive detection of successful reperfusion in patients with acute myocardial infarction. Circulation 1988;78: 1352-1357 Puleo PR, Perryman MB: Noninvasive detection of reperfusion in acute myocardial infarction based on plasma activity of creatine kinase MB subforms. JAm Coll Cardiol 1991;17:1047-1052 Katus HA, Remppis A, Scheffold T, Diederich KW, Kubler W: Intracellular compartmentation of cardiac troponin T and its release kinetics in patients with reperfused and nonreperfused myocardial infarction. Am J Cardiol 1991;67:1360-1367 33. Rosalki SB: An improved procedure for creatine phosphokinase determination. J Lab Clin Med 1967;69:696-705 34. Giegel JL, Brotherton MM, Cronin P, D'Aquino M, Evans S, Heller ZH, Knight WS, Krishnan K, Sheiman M: Radial partition immunoassay. Clin Chem 1982;28:1994-1998 35. Hangaard J, Rasmussen 0, Norregaard-Hansen K, Jorgensen N, Simonsen EE, Norgaard-Pedersen B: Early diagnosis of acute myocardial infarction with a rapid latex agglutination test for semiquantitative estimation of serum myoglobin. Acta Med Scand 1987; 221:343-348 36. Katus HA, Remppis A, Looser S, Hallermayer K, Scheffold K, Kubler W: Enzyme linked immunoassay of cardiac troponin T for the detection of an acute myocardial infarction in patients. J Mol Cell Cardiol 1989;21:1349-1353 37. Katus HA, Remppis A, Neumann FJ, Scheffold T, Diederich KW, Vinar G, Noe A, Matern G, Kubler W: Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation 1991;83:902-912 38. Meinertz T, Kasper W, Schumacher M, Just H for the APSAC Multicenter Trial Study Group: The German multicenter trial of anisoylated plasminogen streptokinase activator complex versus heparin for acute myocardial infarction. Am J Cardiol 1988;62: 347-351 39. Lewis BS, Ganz W, Laramee P, Cercek B, Hod H, Shah PK, Lew AS: Usefulness of a rapid initial increase in plasma creatine kinase activity as a marker of reperfusion during thrombolytic therapy for acute myocardial infarction. Am J Cardiol 1988;62:20-24 40. Hanley JA, McNeil BJ: The meaning and use of the area under a receiver operator characteristic (ROC) curve. Radiology 1982;143: 29-36 41. Hanley JA, McNeil BJ: A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983;148:839-843 42. Swets JA: Measuring the accuracy of diagnostic systems. Science 1988;249:1285-1293 43. Mair J, Smidt J, Artner-Dworzak E, Lechleitner P, Dienstl F, Puschendorf B: Rapid diagnosis of myocardial infarction by immuno turbidimetric myoglobin measurement. (letter) Lancet 1991;337:1343-1344 44. Ishii J, Nomura M, Ando T, Hasegewa H, Kimura M, Tateishi R, Kurokawa H, Kondo T, Hishida H, Mizuno Y: Early detection of coronary reperfusion based on serum myoglobin concentration. (abstract) Circulation 1991;84(suppl II):II-217 45. Clemmensen P, Jurlander B, Grande P, Ohman EM, Wagner GS: Monitoring peak serum-myoglobin for non-invasive prediction of coronary reperfusion in patients. (abstract) Circulation 1991; 84(suppl II):II-116 Analysis of creatine kinase, CK-MB, myoglobin, and troponin T time-activity curves for early assessment of coronary artery reperfusion after intravenous thrombolysis. M Zabel, S H Hohnloser, W Köster, M Prinz, W Kasper and H Just Downloaded from http://circ.ahajournals.org/ by guest on September 30, 2016 Circulation. 1993;87:1542-1550 doi: 10.1161/01.CIR.87.5.1542 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1993 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/87/5/1542 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/