Chronic Granulomatous Disease (CGD) and
advertisement
 and")
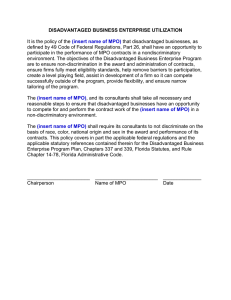
Clinical Chemistry 53:5 890 – 896 (2007) Hematology Chronic Granulomatous Disease (CGD) and Complete Myeloperoxidase Deficiency Both Yield Strongly Reduced Dihydrorhodamine 123 Test Signals but Can Be Easily Discerned in Routine Testing for CGD Lysann Mauch,1 Andreas Lun,2 Maurice R.G. O’Gorman,3 John S. Harris,4 Ilka Schulze,5 Arturo Zychlinsky,6 Tobias Fuchs,6 Uta Oelschlägel,7 Sebastian Brenner,1 Dolphe Kutter,8 Angela Rösen-Wolff,1 and Joachim Roesler1* Background: The flow cytometric dihydrorhodamine 123 (DHR) assay is used as a screening test for chronic granulomatous disease (CGD), but complete myeloperoxidase (MPO) deficiency can also lead to a strongly decreased DHR signal. Our aim was to devise simple laboratory methods to differentiate MPO deficiency (false positive for CGD) and NADPH oxidase abnormalities (true CGD). Methods: We measured NADPH-oxidase and MPO activity in neutrophils from MPO-deficient patients, CGD patients, NADPH-oxidase–transfected K562 cells and cells with inhibited and substituted MPO. Results: Eosinophils from MPO-deficient individuals retain eosinophilic peroxidase and therefore generate a normal DHR signal. The addition of recombinant human MPO enhances the DHR signal when simply added to a suspension of MPO-deficient cells but not when added to NADPH-oxidase– deficient (CGD) cells. Lucigenin-enhanced chemiluminescence (LCL) is increased in neutrophils from MPO-deficient patients, whereas neutrophils from patients with CGD show a decreased response. Conclusions: A false-positive result caused by MPO deficiency can be easily ascertained because, unlike cells from a CGD patient, cells from MPO-deficient patients (a) contain functionally normal eosinophils, (b) show a significant enhancement of the DHR signal following addition of rhMPO, and (c) generate a strong LCL signal. © 2007 American Association for Clinical Chemistry Chronic granulomatous disease (CGD)9 is caused by a genetic defect in 1 of the components of the NADPHoxidase multienzyme complex that produces reactive oxygen intermediates (ROIs). In CGD, the inability to produce ROIs leads to recurrent life-threatening opportunistic infections and uncontrolled inflammation, often accompanied by granuloma formation. In contrast, myeloperoxidase (MPO) deficiency is generally considered to be innocuous and was recently removed as a primary immune deficiency disease as classified by the Primary Immunodeficiency Diseases Classification Committee of the International Union of Immunological Societies (1 ). MPO and the NADPH-oxidase multienzyme complex are 1 University Clinic Carl Gustav Carus, Department of Pediatrics, Dresden, Germany. 2 Institut für Laboratoriumsmedizin und Pathobiochemie, Berlin, Germany. 3 The Children’s Memorial Hospital, Chicago, IL. 4 Valley Medical Center, Lewiston, ID. 5 Department of Pediatrics, Charite, Berlin, Germany. 6 Max Planck Institute for Infection Biology, Berlin, Germany. 7 Department of Haematology, Technische Universität Dresden, Dresden, Germany. 8 Laboratoires Reunis Kutter-Lieners-Hastert, Luxembourg, Luxembourg. * Address correspondence to this author at: University Clinic Carl Gustav Carus, Department of Pediatrics, Fetscherstrasse 74, 01307 Dresden, Germany. Fax: 49-351-458-6333; e-mail: roeslerj@rcs.urz.tu-dresden.de. Received November 23, 2006; accepted February 15, 2007. Previously published online at DOI: 10.1373/clinchem.2006.083444 9 Nonstandard abbreviations: CGD, chronic granulomatous disease; ROI, reactive oxygen intermediate; MPO, myeloperoxidase; DHR, cytometric dihydrorhodamine 123; SHA, salicylhydroxamic acid; ABAH, 4-aminobenzoylhydrazide; PMA, phorbol-myristate-acetate; mAb, monoclonal antibody; LCL, lucigenin-enhanced chemiluminescence. 890 891 Clinical Chemistry 53, No. 5, 2007 involved in ROI metabolism according to the following grossly simplified reaction chain: O2 ⫹ e⫺ ⫹ NADPH-oxidase 3 O2⫺ 3, 3 H2O2 ⫹ Cl⫺ ⫹ MPO 3 HOCl 3, 3 other ROIs H2O2 oxidizes dihydrorhodamine to rhodamine when a peroxidase or an equivalent catalyst is present. Flow cytometric measurement of ROIs by the in vitro stimulation of cells loaded with dihydrorhodamine 123 (DHR) (2 ) was introduced by our group (3, 4 ). The DHR assay is easier to perform, more reliable, and more sensitive than the nitroblue tetrazolium dye reduction assay (5, 6 ), and DHR is also more sensitive than other ROI-indicating fluorescent dyes, such as dichlorofluorescein (7 ). DHR oxidation is not strictly dependent on NADPH-oxidase activity, however, because the oxidation requires (myelo-) peroxidase availability (8 ). In spite of this limitation, the DHR assay has been successfully used to (a) measure transfused non-CGD neutrophils in CGD patients (9 ), (b) measure X-inactivation ratios (lyonization patterns) in X-linked CGD carriers (10 –16 ) even when small percentages of the normal X-linked genes are present (17 ), (c) measure low concentrations of residual NADPH-oxidase activity in CGD patients (10, 18 ), and (d) measure improved granulocyte activity in preclinical (19 ) and clinical gene therapy trials (20, 21 ). In addition, the DHR assay is superior to other methods, such as chemiluminescence, for analyzing shipped blood samples (22, 23 ). CGD is a life-threatening disease, and the diagnosis has significant implications regarding therapy (24 ). It is therefore critical that the limitations of the DHR screening diagnosis assay (and of all other diagnostic tests for CGD) be understood and that confirmatory testing be considered when appropriate. It is in this context that we demonstrate for the 1st time that complete MPO deficiency can lead to a false-positive result for CGD diagnosis using the DHR flow cytometry assay and describe how MPO deficiency can be easily discerned from CGD. Patients, Materials, and Methods patients We evaluated 4 patients with complete MPO deficiency, 2 with partial MPO deficiency, and 3 with CGD (2 without and 1 with residual NADPH-oxidase activity) and compared them in each of the assays described below (Table 1). All patients and/or their parents consented to blood drawing and genetic analysis. materials We purchased salicylhydroxamic acid (SHA) and 4-aminobenzoylhydrazide (ABAH) from Sigma-Aldrich and TCI America, respectively, and DHR, lucigenin, horseradish peroxidase type VI-A, rhMPO, lactoperoxidase, phorbol-myristate-acetate (PMA), and zymosan A from SigmaAldrich. Transfected K562 cells that permanently express gp91-phox, p47-phox, and p67-phox and have endogenous p22-phox were a kind gift from Dr. T. Leto, Laboratory of Host Defenses, National Institute of Allergy and Infectious Diseases, NIH, Bethesda, MD. flow cytometric dhr assay K562 cells were adjusted to 109/L in PBS (137 mmol/L NaCl, 10 mmol/L phosphate, 2.7 mmol/L KCl, pH 7.4), as were neutrophils that had been isolated from lithium-heparin– containing whole peripheral blood by dextran sedimentation followed by hypotonic erythrolysis or from buffy coat cell layers. We incubated all cells in 500-L aliquots with 20 L of 1.6 mol/L PMA for 5 min at 37 °C with or without rhMPO (1 kU/L) or MPO inhibitors as indicated. Thereafter, we added 7.5 L of 30 mol/L DHR followed by another 15-min incubation period at 37 °C, storage on ice, and flow cytometric analysis as described (22 ). Experiments performed in whole blood with the commercially available Phagoburst reagent set (Orpegen Pharma) yielded similar results in all cases (data not shown). Table 1. Genes affected and effects on functions in reactive oxygen metabolism as measured by DHR and LCL. Patient no. 1–3 4 Sex Status Mutation 2 M, 1 F MPO deficiency Ex12–2A3C/Ex12– 2A3C F MPO deficiency Ex12–2A3C/R569W 5 6 7 F F M 8 M 9 M MPO deficiency Ex12–2A3C/A332V MPO deficiency R569W/A332V CGD IVS6–1157A3G X chromosome CGD 962T3G and 970delG X chromosome CGD delGly533 X chromosome Gene affected MPO MPO MPO MPO CYBB CYBB CYBB MPO activity DHR signal in neutrophils None, e.g., Fig. 1, 2(s), B and E variable None, e.g., Fig. 1, s Fig. 2A B and E Trace, Fig. 1F Normal Trace Normal Normal s, Fig. 2C, 4D Normal Absent, Fig. 4C Normal Absent DHR signal enhanced by rhMPO LCL signal Ref., effect of mutation Yes, n ⫽ 2, Fig. 4A ND a, Fig. 2B (28 ) a, Fig. 2B (28–30 ) ND ND No, Fig. 4D a a s, Fig. 2D (28 ) (28, 29 ) (18 ) No, Fig. 4C Absent No Absent (24, 27 ) Ex (exon) 12–2A3 C (c0.2031–2A⬎C), splice mutation with no in-frame splicing; IVS6 –1157A3 G, complex splice mutation with residual normal splicing; 962T3 G and 970delG, complex null mutation; s, strongly decreased, but present; a, strongly increased; ND, not done. 892 Mauch et al.: CGD and MPO Deficiency modified dhr assay We added 20 L of 1.6 mol/L PMA or 20 L of a 10 g/L nonopsonized vortex-mixed zymosan A suspension and 20 L of a 60 mol/L DHR solution to 200-L cell suspensions (2 ⫻ 106/mL) in a 96-well plate together with different concentrations of MPO inhibitors as indicated. We detected rhodamine fluorescence resulting from oxidized DHR fluorescence by excitation at 485 nm and measured emitted light at 535 nm by use of the Mithras LB 940-luminometer (Berthold Technologies). lucigenin-enhanced chemiluminescence Neutrophils isolated as described above or transfected K562 cells were adjusted to 2 ⫻ 106/mL in PBS, divided into 200-L aliquots, and preincubated with 4 L of a 10 mmol/L solution of lucigenin at 37 °C for 30 min. We added 20 L of 1.6 mol/L PMA or 20 L of a 10 g/L nonopsonized vortex-mixed zymosan A suspension, followed by 30 min of counting at 37 °C by use of the Mithras LB 940-luminometer with or without MPO inhibitors. mpo activity We detected and verified MPO deficiency by (a) the Advia-120 hematology analyzer (25 ), (b) flow cytometry after staining of permeabilized cells with the MPO-7 fluorescein isothiocyanate monoclonal antibody (mAb; DakoCytomation, Kopenhagen, Denmark) according to conventional techniques (Fig. 1), (c) staining of cell smears with o-dianisidine modified from Fujinami et al. (26 ), and (d) photometry. We verified inhibition of MPO activity by SHA and ABAH in assays c and d. Using primers to amplify individual exons including intron boundaries of MPO (myeloperoxidase)10 and CYBB (cytochrome b-245, also called gp91-phox) (18, 27 ), we performed nucleotide sequencing of genomic DNA from MPO-deficient patients and CGD patients. Results The DHR signal yielded by flow cytometry in the routine diagnostic screening assay for CGD depends on intact NADPH-oxidase activity as well as the presence of a peroxidase such as MPO, as shown in Fig. 2. The DHR fluorescence (Fl1) generated by PMA-activated neutrophils of the completely MPO-deficient patient (Table 1, patient 1) was significantly below normal (Fig. 2A) and was comparable to that of an X-CGD patient (Table 1, patient 7) with some residual NADPH-oxidase activity (Fig. 2C). Thus, complete MPO deficiency could be confused with CGD (false positive). In the presence of complete MPO deficiency, a small subpopulation of cells yielded a high DHR signal upon activation with PMA (Fig. 2A, arrow). This subpopulation consisted of eosinophils, which contain the same 10 Human genes: MPO, myeloperoxidase; CYBB; cytochrome b-245. Fig. 1. Staining of MPO-deficient (A, B) and normal (C, D) neutrophils with the MPO-specific mAb MPO-7 and position of completely (E) and partially (F) MPO-deficient neutrophils in the Advia-120 display. (A, C), isotype control; (B, D), addition of mAb MPO-7. Completely MPO-deficient neutrophils localize in the upper part of the upper left field (E), whereas traces of MPO activity are indicated by their localization in the field next to it (F). The line depicting an oval shape marks the position where neutrophils with normal amounts of MPO would normally localize if present. FSC, forward scatter. NADPH-oxidase as neutrophils, but they contain eosinophilic peroxidase instead of MPO. Measurement of lucigenin-enhanced chemiluminescence (LCL) indicated that the signals were significantly increased (consistent with normal NADPH-oxidase) in the MPO-deficient patient (Fig. 2B) but were significantly decreased from normal in patients with a confirmed diagnosis of CGD (Fig. 2D). We confirmed MPO deficiency in patient 1 by use of mAb staining (Fig. 1, A and B), the Advia-120 automated hematology analyzer (25 ) (Fig. 1E), and o-dianisidine staining (data not shown). Three additional patients were confirmed to be completely MPO deficient (Table 1, patients 2, 3, and 4) by 2 or 3 of these methods. We confirmed the mutations in the gene leading to MPO deficiency by genomic sequencing (Table 1). We detected the frequent exon12–2A3 C splice mutation (c.2031–2A⬎C) in 8 alleles, and the A332V and R569W missense mutations in 2 alleles each. None of the patients were related. The c.2031–2A⬎C and the R569W mutation have been published as null mutations, i.e., no residual MPO activity was detected (28 –30 ). The neutrophils iso- 893 Clinical Chemistry 53, No. 5, 2007 Fig. 2. DHR assay (left panel) and LCL (right panel) on granulocytes from a completely MPO-deficient patient (A, B), a CGD patient (C, D), and a healthy blood donor (E). (A, C, E), gray lines, no stimulation; black lines, maximal stimulation with PMA; arrow, PMA-activated eosinophils. (B, D), black symbols, patients; open symbols, normal, healthy blood donor; diamonds, maximal PMA activation; triangles, activation with zymosan A; background on abscissa (crosses), no stimulation. Note the different scale (right ordinate). lated from all of the patients with complete MPO deficiency generated variable but significantly decreased PMA-induced DHR fluorescence signals. Traces of detectable MPO resulted in the generation of normal DHR fluorescence (Table 1). When we added the MPO inhibitors SHA and ABAH to suspensions of normal neutrophils and performed a modified DHR flow assay (Fig. 3), both inhibitors markedly decreased the zymosan A–induced DHR fluorescence signal (Fig. 3A). The inhibition was not attributable to cell damage or cell death, because the same concentrations of the inhibitors actually enhanced the LCL signal (Fig. 3B). Fluorescence in these experiments was measured by luminometry, because zymosan particles interfered with the light scatter detection of cells by flow cytometry. Experiments combining PMA, SHA, and ABAH were inconclusive, presumably owing to their combined toxicity. K562 cells containing no endogenous peroxidase and transfected to express gp91-phox, p47-phox, and p67phox [and having endogenous p22-phox (31 )] provided a model to investigate the peroxidase dependency of PMAinduced DHR oxidation by H2O2. The transfected components of NADPH-oxidase allowed for the production of high amounts of ROIs, as demonstrated by a strong LCL signal (31 ), but yielded no PMA-induced DHR oxidation, as demonstrated by the lack of increase in the fluorescence signal (Fig. 4B). The addition of rhMPO, however, led to a significant increase in the intensity of DHR fluorescence following in vitro activation. A similar result was observed in patients with the false-positive CGD DHR result who had no residual MPO activity (Fig. 4A; Table 1). Addition of rhMPO enhanced the DHR signal in the Fig. 3. Effect of MPO inhibitors on DHR oxidation (A) and LCL (B) in normal neutrophils. (A), fluorescence of rhodamine 123 (oxidized DHR). (B), LCL counts in percentage of uninhibited samples (ordinate). Abscissa, concentration of inhibitors; open columns, ABAH; striped columns, SHA; error bars, SD; 15 independent experiments. MPO-deficient patients’ neutrophils, thus providing a clear discrimination between MPO deficiency and CGD. As shown in Fig. 4, addition of rhMPO did not change the DHR signal in CGD patients with (Fig. 4D) or without (Fig. 4C) detectable residual NADPH oxidase activity. We detected considerable variability in the DHR fluorescence of the complete MPO-deficient patients (as well as in different samples from 1 individual, compare Figs. 2 and 4). Therefore, the DHR assay may not be reliable in detecting MPO deficiency. In contrast to rhMPO, the addition of horseradish peroxidase (2 different forms) or lactoperoxidase led to an increase in DHR fluorescence even in the absence of a functional NADPH-oxidase (data not shown). Therefore, such peroxidases should not be used to investigate MPO deficiency in the DHR assay. Discussion The incidence of MPO deficiency is estimated to be ⬃1 in 2000 individuals. Although the MPO system is highly conserved in the evolution of mammals, and decreases in the early stages of in vitro killing of certain bacteria, such as Staphylococcus aureus, by MPO-deficient neutrophils have been observed, the vast majority of MPO-deficient individuals in industrialized countries do not exhibit signs of overt immunodeficiency (32 ). One study de- 894 Mauch et al.: CGD and MPO Deficiency Fig. 4. Addition of rhMPO can enhance the DHR signal in MPO-deficient cells (A, B) but not in cells from CGD patients (C, D). Gray lines, DHR and rhMPO alone (position never deviated from cells incubated with DHR alone; omitted for clarity); dashed lines, activation with PMA, no MPO; black lines, activation with PMA in the presence of rhMPO. Abscissa, DHR fluorescence. (A), MPO-deficient patient 1; (B), K562 cells with functional NADPH-oxidase, representative result of 4 experiments; (C), CGD neutrophils without any NADPH-oxidase activity; (D), CGD neutrophils with residual NADPHoxidase activity. signed to avoid disease detection bias reported a significantly enhanced frequency of severe, though heterogeneous, infections in MPO-deficient individuals (33 ), but such events were rare. An association of MPO deficiency with Candida infections in diabetic patients has been described, and associations with decreased or increased frequencies of noninfectious diseases have also been reported (32, 33 ). It remains possible that the MPO system is a very important host defense system when the host is challenged by high doses of infectious agents. In contrast to defects in the MPO gene, mutations in the genes encoding the components of NADPH-oxidase result in CGD, a life-threatening diagnosis that demands appropriate clinical management and therapeutic decisions (24, 34 ). Life-threatening conditions include both severe infections and uncontrolled inflammation associated with granuloma formation even in the absence of overt infection. In comparison with classic CGD, CGD with residual NADPH-oxidase activity is usually less severe and can manifest at an older age, with less severe infection and longer intervals between infections. This does not apply to all such patients, however, and manifestations can be as severe as in classic CGD. Because of the dire consequences of a CGD diagnosis, it is imperative that MPO deficiency not be falsely diagnosed as CGD. As indicated in this study, complete MPO deficiency can lead to a significantly reduced fluorescence signal in the DHR assay that is consistent with the results observed in some CGD patients (Fig. 2). In contrast, cells obtained from partial MPO deficiency containing only minimal residual MPO activity generated fluorescence signals consistent with normal (non-CGD) individuals (8, 22 ). This was confirmed in patients 5 and 6, whose neutrophils contained only trace amounts of MPO but generated PMA-induced DHR fluorescence signals consistent with those of control individuals (Table 1). Our investigation provides direct evidence that the oxidation of DHR by H2O2 depends on a peroxidase in cellular systems (Figs. 2A and 4, A and B). These results are in accordance with those of inhibitor experiments of MPO (Fig. 3) and the results of van Pelt et al. (8 ). As expected, eosinophilic peroxidase can replace MPO in mediating DHR oxidation (Fig. 2A, arrow). Most patients will have detectable eosinophils, although at low frequency in peripheral blood. Therefore, strong DHR staining of eosinophils after activation with PMA is an extremely facile method to exclude CGD. It is important, however, to discern eosinophils from cell aggregates in the forward/side scatter diagram. It is also important not to confuse a subset of normal ROI-producing granulocytes present in X-linked CGD carriers (that can be small; see Introduction) (35, 36 ). Identification of eosinophils by flow cytometry can be challenging and may not always allow for differentiation between CGD and MPO deficiency. In such cases, alternative methods can be adopted for the rapid identification of false-positive CGD due to complete MPO deficiency. The simple addition of rhMPO to the assay (Fig. 4) enables a very rapid and clear discernment between MPO deficiency and CGD, as cells from patients with true CGD will not be affected by rhMPO. MPO deficiency can be clearly demonstrated using a monoclonal anti-MPO antibody with conventional intracellular staining. MPO is strongly expressed in granulocytes, less so in monocytes, and not at significant levels in lymphocytes, thus providing built-in staining controls. Clinical Chemistry 53, No. 5, 2007 Finally, all measurements of ROIs in neutrophils that use indicators independent of MPO yield considerably enhanced readouts in the presence of MPO deficiency. This is attributed to a regulatory effect of MPO, the products of which are presumed to down-regulate NADPH-oxidase (37 ). In the experiments shown here, LCL was used to measure O2⫺ independent of MPO. As demonstrated in Fig. 2B, the O2⫺ production plateaus at a level more than 3 times higher in MPO-deficient neutrophils than in those cells obtained from non-CGD control blood donors (Fig. 2, B and D). Another possible complementary assay is luminol-enhanced chemiluminescence (38 ) comparing luminol oxidation by PMA-activated neutrophils in the absence and presence of horseradish peroxidase (1.2 kU/L). In the case of MPO deficiency, but not in the case of CGD, the added peroxidase strongly enhances luminol oxidation (unpublished results), a reaction that parallels the effect of rhMPO in the DHR assay (Fig. 4). We do not recommend the DHR assay as a screen for MPO deficiency because of the variable results observed and the lack of sensitivity in detecting partial MPO deficiency. It is possible that there are redundant peroxidases that may substitute for MPO, and it has been reported that DHR may be less dependent on MPO than dichlorofluorescein diacetate (39 ). In summary, it is important to consider complete MPO deficiency when a result consistent with CGD is obtained using the DHR assay, especially if patient history is not consistent with a diagnosis of CGD. It is easy to discriminate between the 2 enzyme deficiencies by (a) consideration of eosinophils, (b) addition of rhMPO and observation of the effect on the DHR-123 assay, (c) intracellular staining with anti-MPO antibody, and/or (d) the use of MPO-independent ROI detection methods such as LCL. In cases in which a diagnosis of CGD is suspected, we highly recommend that confirmatory tests (sequencing or others) be performed. Grant/funding support: None declared. Financial disclosures: None declared. Acknowledgements: We thank Katrin Höhne for excellent assistance; Dr. Thomas Leto, NIH, Bethesda, MD, for the transfected K562 cells; and Andrea Gross for excellent graphic design. References 1. Notarangelo L, Casanova JL, Conley ME, Chapel H, Fischer A, Puck J, et al. Primary immunodeficiency diseases: an update from the International Union of Immunological Societies Primary Immunodeficiency Diseases Classification Committee Meeting in Budapest, 2005. J Allergy Clin Immunol 2006;117:883–96. 2. Rothe G, Oser A, Valet G. Dihydrorhodamine 123: a new flow cytometric indicator for respiratory burst activity in neutrophil granulocytes. Naturwissenschaften 1988;75:354 –5. 895 3. Roesler J, Hecht M, Freihorst J, Lohmann-Matthes ML, Emmendorffer A. Diagnosis of chronic granulomatous disease and of its mode of inheritance by dihydrorhodamine 123 and flow microcytofluorometry. Eur J Pediatr 1991;150:161–5. 4. Emmendorffer A, Hecht M, Lohmann-Matthes ML, Roesler J. A fast and easy method to determine the production of reactive oxygen intermediates by human and murine phagocytes using dihydrorhodamine 123. J Immunol Methods 1990;131:269 –75. 5. Vowells SJ, Fleisher TA, Malech HL. Testing for chronic granulomatous disease. Lancet 1996;347:1048 –9. 6. Roesler J, Emmendorffer A. Diagnosis of chronic granulomatous disease. Blood 1991;78:1387–9. 7. Vowells SJ, Sekhsaria S, Malech HL, Shalit M, Fleisher TA. Flow cytometric analysis of the granulocyte respiratory burst: a comparison study of fluorescent probes. J Immunol Methods 1995;178: 89 –97. 8. van Pelt LJ, van Zwieten R, Weening RS, Roos D, Verhoeven AJ, Bolscher BG. Limitations on the use of dihydrorhodamine 123 for flow cytometric analysis of the neutrophil respiratory burst. J Immunol Methods 1996;191:187–96. 9. Emmendorffer A, Lohmann-Matthes ML, Roesler J. Kinetics of transfused neutrophils in peripheral blood and BAL fluid of a patient with variant X-linked chronic granulomatous disease. Eur J Haematol 1991;47:246 –52. 10. Jirapongsananuruk O, Malech HL, Kuhns DB, Niemela JE, Brown MR, Anderson-Cohen M, et al. Diagnostic paradigm for evaluation of male patients with chronic granulomatous disease, based on the dihydrorhodamine 123 assay. J Allergy Clin Immunol 2003; 111:374 –9. 11. Rupec RA, Petropoulou T, Belohradsky BH, Walchner M, Liese JG, Plewing G, et al. Lupus erythematosus tumidus and chronic discoid lupus erythematosus in carriers of X-linked chronic granulomatous disease. Eur J Dermatol 2000;10:184 –9. 12. Crockard AD, Thompson JM, Boyd NA, Haughton DJ, McCluskey DR, Turner CP. Diagnosis and carrier detection of chronic granulomatous disease in five families by flow cytometry. Int Arch Allergy Immunol 1997;114:144 –52. 13. Atkinson TP, Bonitatibus GM, Berkow RL. Chronic granulomatous disease in two children with recurrent infections: family studies using dihydrorhodamine-based flow cytometry. J Pediatr 1997; 130:488 –91. 14. Koker MY, Sanal O, de Boer M, Tezcan I, Metin A, Tan C, et al. Skewing of X-chromosome inactivation in three generations of carriers with X-linked chronic granulomatous disease within one family. Eur J Clin Invest 2006;36:257– 64. 15. Lun A, Roesler J, Renz H. Unusual late onset of X-linked chronic granulomatous disease in an adult woman after unsuspicious childhood. Clin Chem 2002;48:780 –1. 16. Rosen-Wolff A, Soldan W, Heyne K, Bickhardt J, Gahr M, Roesler J. Increased susceptibility of a carrier of X-linked chronic granulomatous disease (CGD) to Aspergillus fumigatus infection associated with age-related skewing of lyonization. Ann Hematol 2001; 80:113–5. 17. Anderson-Cohen M, Holland SM, Kuhns DB, Fleisher TA, Ding L, Brenner S, et al. Severe phenotype of chronic granulomatous disease presenting in a female with a de novo mutation in gp91-phox and a non familial, extremely skewed X chromosome inactivation. Clin Immunol 2003;109:308 –17. 18. Rump A, Rosen-Wolff A, Gahr M, Seidenberg J, Roos C, Walter L, et al. A splice-supporting intronic mutation in the last bp position of a cryptic exon within intron 6 of the CYBB gene induces its incorporation into the mRNA causing chronic granulomatous disease (CGD). Gene 2006;371:174 – 81. 19. Mardiney M III, Jackson SH, Spratt SK, Li F, Holland SM, Malech HL. Enhanced host defense after gene transfer in the murine 896 20. 21. 22. 23. 24. 25. 26. 27. 28. Mauch et al.: CGD and MPO Deficiency p47phox-deficient model of chronic granulomatous disease. Blood 1997;89:2268 –75. Ott MG, Schmidt M, Schwarzwaelder K, Stein S, Siler U, Koehl U, et al. Correction of X-linked chronic granulomatous disease by gene therapy, augmented by insertional activation of MDS1-EVI1, PRDM16 or SETBP1. Nat Med 2006;12:401–9. Malech HL, Maples PB, Whiting-Theobald N, Linton GF, Sekhsaria S, Vowells SJ, et al. Prolonged production of NADPH oxidasecorrected granulocytes after gene therapy of chronic granulomatous disease. Proc Natl Acad Sci U S A 1997;94:12133– 8. Emmendorffer A, Nakamura M, Rothe G, Spiekermann K, Lohmann-Matthes ML, Roesler J. Evaluation of flow cytometric methods for diagnosis of chronic granulomatous disease variants under routine laboratory conditions. Cytometry 1994;18:147–55. O’Gorman MR, Corrochano V. Rapid whole-blood flow cytometry assay for diagnosis of chronic granulomatous disease. Clin Diagn Lab Immunol 1995;2:227–32. Roesler J, Koch A, Porksen G, von Bernuth H, Brenner S, Hahn G, et al. Benefit assessment of preventive medical check-ups in patients suffering from chronic granulomatous disease (CGD). J Eval Clin Pract 2005;11:513–21. Van den Bossche J, Devreese K, Malfait R, Van de Vyvere M, Wauters A, Neeis H, et al. Reference intervals for a complete blood count determined on different automated haematology analysers: Abx Pentra 120 Retic, Coulter Gen-S, Sysmex SE 9500, Abbott Cell Dyn 4000 and Bayer Advia 120. Clin Chem Lab Med 2002;40:69 –73. Fujinami N, Sugimoto Y, Hagiwara A. Induction of erythroid maturation by dimethyl sulfoxide in friend leukemic cells. Dev Growth Differ 1973;15:141–51. Roesler J, Heyden S, Burdelski M, Schafer H, Kreth HW, Lehmann R, et al. Uncommon missense and splice mutations and resulting biochemical phenotypes in German patients with X-linked chronic granulomatous disease. Exp Hematol 1999;27:505–11. Marchetti C, Patriarca P, Solero GP, Baralle FE, Romano M. Genetic characterization of myeloperoxidase deficiency in Italy. Hum Mutat 2004;23:496 –505. 29. Nauseef WM, Cogley M, McCormick S. Effect of the R569W missense mutation on the biosynthesis of myeloperoxidase. J Biol Chem 1996;271:9546 –9. 30. Nauseef WM, Brigham S, Cogley M. Hereditary myeloperoxidase deficiency due to a missense mutation of arginine 569 to tryptophan. J Biol Chem 1994;269:1212– 6. 31. de M, I, Leto TL. Functional reconstitution of the phagocyte NADPH oxidase by transfection of its multiple components in a heterologous system. Blood 1995;85:1104 –10. 32. Suzuki K, Muso E, Nauseef WM. Contribution of peroxidases in host-defense, diseases and cellular functions. Jpn J Infect Dis 2004;57:S1–2. 33. Kutter D. Inborn metabolic errors of white blood cells: myeloperoxidase deficiency of neutrophils and monocytes physiopathological consequences. Klinicka Biochemie Metabolismus 2003;11: 141–7. 34. Cale CM, Jones AM, Goldblatt D. Follow up of patients with chronic granulomatous disease diagnosed since 1990. Clin Exp Immunol 2000;120:351–5. 35. Weening RS, de Boer M, Kuijpers TW, Neefjes VM, Hack WW, Roos D. Point mutations in the promoter region of the CYBB gene leading to mild chronic granulomatous disease. Clin Exp Immunol 2000;122:410 –7. 36. Woodman RC, Newburger PE, Anklesaria P, Erickson RW, Rae J, Cohen MS, et al. A new X-linked variant of chronic granulomatous disease characterized by the existence of a normal clone of respiratory burst-competent phagocytic cells. Blood 1995;85: 231– 41. 37. Klebanoff SJ. Myeloperoxidase. Proc Assoc Am Physicians 1999; 111:383–9. 38. Aniansson H, Stendahl O, Dahlgren C. Comparison between luminol- and lucigenin-dependent chemiluminescence of polymorphonuclear leukocytes. Acta Pathol Microbiol Immunol Scand [C] 1984;92:357– 61. 39. Crow JP. Dichlorodihydrofluorescein and dihydrorhodamine 123 are sensitive indicators of peroxynitrite in vitro: implications for intracellular measurement of reactive nitrogen and oxygen species. Nitric Oxide 1997;1:145–57.