Polarity Montages Localization

Polarity
Montages
Localization
Bassel Abou-Khalil, M.D.
I have no financial relationships to disclose that are relative to the content of my presentation
Learning Objectives
to predict the appearance of potentials of negative or positive polarity in different montages
to localize EEG potentials in referential and bipolar recordings
to build montages that are logical; identify the advantages and disadvantages of bipolar and referential montages; select the best montages to characterize particular potentials
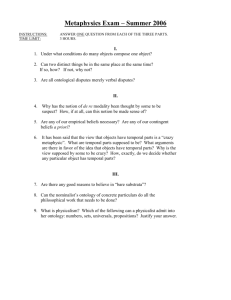
What is the polarity of the transient demonstrated below
Fp1-F3
A.
Positive
B.
Negative
C.
Either positive or negative
D.
Neither
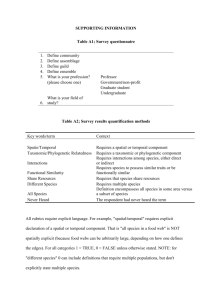
Where is the most likely source of this transient?
Fp1-F3
F3-C3
C3-P3
P3-O1
A.
P3 and O1
B.
O1
C.
Fp1, C3, & P3
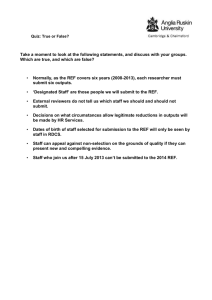
What is the most likely polarity of this transient?
Fp1-F3
F3-C3
C3-P3
P3-O1
A.
Positive
B.
Negative
C.
Either positive or negative
Where is the center of the field?
Fp1-F3
F3-C3
C3-P3
P3-O1
A.
C3 and P3
B.
C3
C.
F3
D.
Fp1
The EEG
The EEG measures potential differences between electrode positions on the scalp.
Factors affecting scalp EEG potentials
Size, depth, orientation of generator/dipole
Conductive properties of intervening tissues
Duration of discharge
Degree of synchronization
– Synchronous discharge over 10 cm 2 cortex surface area needed for spikes to show on scalp
Propagation pattern
Recording technique
Dipole orientation
-
-
EEG at scalp
Amplitude depends on:
– intensity of electrical potential
– distance of potential
– spatial orientation of dipole
– resistance and capacitance of structures between source and electrodes
Amplitude may decrease with:
– increased impedance
– decreased impedance resulting in current shunt
EEG at scalp
Potential changes are favored if they:
– occur near the recording electrodes
– are generated in a large area of tissue
– rise and fall at a slow speed
Potentials generated at a distant site are rarely recorded, but those of high amplitude and low frequency may be transmitted through volume conduction
T1
10-10 system
Combinatorial
Nomenclature
Fp1 Fp2
True anterior temporal
T1
Zg1
Inferolateral temporal
Sp1
F7
Anterior temporal
Inferior frontal
Anterior sylvian
Fronto-temporal
Frontopolar Frontopolar
F3 F4
Fz
Mid-frontal
Midline frontal
Mid-frontal
Cz C4
Inferomesial temporal
T7
Mid-temporal
C3
Central
Vertex
Central
F8
T2
Anterior temporal
Inferior frontal
Anterior sylvian
Fronto-temporal
T8
Mid-temporal
True anterior temporal
Zg2
Sp2
Inferolateral temporal
Inferomesial temporal
P3
P7
Parietal
Posterior temporal
Pz
Midline Parietal
P4
Parietal
P8
Posterior temporal
O1
Occipital
O2
Occipital
POLARITY- LOCALIZATION
Negative
↑
↓
Positive
↓
↑
Lüders Method
B
C
-
+
Lüders Method
A
B
B
C
+
-
+
MONTAGES- BIPOLAR
or midline
Longitudinal Bipolar Montage
Vanderbilt arrangement
10
9
1 5
2 17 6
13
14
11
3 18 7
15
12
4 8
16
Transverse Bipolar Montage
Vanderbilt- Arcs replacing single derivation chains
2
1 3
4 5 6 7
8 9 10 11 12
13
14 15 16 17
18
19
20
END OF CHAIN POTENTIALS
Vanderbilt “Additional” Montage
3
2
4
1
11 14
5
6 12 15
7
13 16
8
9
10
MONTAGES- REFERENTIAL
Referential Montages
Vanderbilt Organization
1
3
11
5
13
7
15
9
17
18
19
2
4
12
6
8
10
16
14
Referential Montages
Alternate Arrangement 1
1
2
11
3
12
4
13
5
17
18
19
6
7
14
8
9
10
16
15
Referential Montages
Alternate Arrangement 2
2
1
3
4
5
6
7
8
9
10
11
12
13
17
14
18
15
16
19
References
Ipsilateral ear
Linked ears
Average
Laplacian
Vertex or other midline reference
Balanced noncephalic reference
Considerations in choosing ear reference
Ideal for generalized abnormalities, which usually predominate in the midline. The ears are the least involved and usually provide the best fidelity.
EKG artifact may be prominent- linking the ears helps cancel out EKG artifact.
Ear reference can be contaminated with temporal lobe abnormal activity (sharp waves or slow activity)
Active ear reference
Fp1
F7
F3 Fz
A1 T7 C3
P7 P3
Cz
Pz
O1
Fp1-A1
F3-A1
C3-A1
P3-A1
O1-A1
F7-A1
T7-A1
P7-A1
Fp1-A2
F3-A2
C3-A2
P3-A2
O1-A2
F7-A2
T7-A2
P7-A2
A1-A2
Considerations in choosing average reference
Average reference is ideal for focal activity, particularly from the temporal lobe
Average reference can be improved by excluding affected electrodes
Average reference tends to get contaminated with generalized abnormal activity
Considerations in choosing vertex reference
Can emphasize/clarify temporal activity
(particularly when average reference is affected by artifact).
Not a good choice during sleep (a lot of high voltage sleep activity is maximal in the midline) or to display activity that is generalized or close to the midline.
What is this?
Focal left temporal sharp waves+ contaminated ear
Focal right temporal sharp waves- Average Ref
Focal right temporal sharp waves- Cz Ref
Focal right temporal sharp waves- Ipsi Ear Ref
Focal right temporal sharp waves- Linked Ear Ref
Focal right temporal sharp waves- Average Ref
Focal right temporal sharp waves- Average Ref
Average reference
Focal right temporal sharp waves- Average ref- cleaned
Average reference- ave cleaned
Focal left posterior activity- Average Ref
Focal left posterior activity- Average Ref- cleaned
Sleep spindles and vertex waves- Ipsi Ear Ref
Sleep spindles and vertex waves- Average Ref
Generalized spike-and-wave activity- Linked Ear Ref
Generalized spike-and-wave activity- Ave Ref
Bifrontal spike-and-wave activity- Ipsi Ear Ref
Bifrontal spike-and-wave activity- Ave Ref
Bifrontal spike-and-wave activity- Fz Ref
Laplacian reference
Each channel in a Laplacian montage is referenced to an average of the electrodes surrounding it
Filters out coherent widespread activity and emphasizes localized waveforms
The Laplacian reference performs well in environments where low-to-moderate artifact can be expected (e.g., any in-lab or inpatient scalp EEG recording)
Balanced Non-Cephalic Reference
Can be considered when it is not possible to find a cephalic reference that is not contaminated by the EEG signal of interest.
Commonly used for evoked potential recordings, where signal averaging effectively removes EKG artifact.
EKG contamination is problematic, but can be diminished by deriving the reference from a combination of two electrodes.
– If the electrodes are placed to present R-waves of opposite polarity they can be summed to cancel each other, removing the EKG artifact from the non-cephalic reference.
Bipolar Recordings
Advantages: sharp distinction
Disadvantages
– Distort wave shape and amplitude
– Widespread potentials may be canceled
– Potentials maximal at the end of a chain or equal in the last 2 electrodes in a chain can result in confusing potentials
Referential recordings
Advantages
– Undistorted display of the shape of potential changes
– Especially useful for potential changes with a wide distribution (not average reference)
Disadvantages
– Reference electrode may be active
– Small focal potentials may be less visible
Localization of potentials
Referential recordings with a neutral reference
– First input in the channel with the highest amplitude (usually greatest negativity, or rarely greatest positivity) is the center of the field
Bipolar recordings
– Electrode(s) common to the channels where reversal of polarity occurs is usually the center of the field
Fp1-F3
F3-C3
C3-P3
P3-O1
Fp2-F4
F4-C4
C4-P4
P4-O2
Fp1-F7
F7-T7
T7-P7
P7-O1
Fp2-F8
F8-T8
T8-P8
P8-O2
Fz-Cz
Cz-Pz
EKG
Fp1-Av
Fp2-Av
F3-Av
F4-Av
C3-Av
C4-Av
P3-Av
P4-Av
O1-Av
O2-Av
F7-Av
F8-Av
T7-Av
T8-Av
P7-Av
P8-Av
Fz-Av
Cz-Av
Pz-Av
ECG
Fp1-Av
Fp2-Av
F3-Av
F4-Av
C3-Av
C4-Av
P3-Av
P4-Av
O1-Av
O2-Av
F7-Av
F8-Av
T7-Av
T8-Av
P7-Av
P8-Av
Fz-Av
Cz-Av
Pz-Av
ECG
Average reference with removal of Fz, Cz, F4, C4, T4 from the average
What is the polarity of the transient demonstrated below
Fp1-F3
A.
Positive
B.
Negative
C.
Either positive or negative
D.
Neither
Where is the most likely source of this transient?
Fp1-F3
F3-C3
C3-P3
P3-O1
A.
P3 and O1
B.
O1
C.
Fp1, C3, & P3
What is the most likely polarity of this transient?
Fp1-F3
F3-C3
C3-P3
P3-O1
A.
Positive
B.
Negative
C.
Either positive or negative
Where is the center of the field?
Fp1-F3
F3-C3
C3-P3
P3-O1
O1- X
40
40
100
40
A.
C3 and P3
B.
C3
C.
F3
D.
Fp1
EEG LOCALIZATION PROBLEMS
Most likely solutions
A-ref
B-ref
C-ref
D-ref
E-ref
1
5
A-B
B-C
C-D
D-E
4
5
A
B
C
D
E
5
2
A-B
B-C
C-D
D-E
3
2
A
B
C
D
E
5
2
A-B
B-C
C-D
D-E
3
2
A
B
C
D
E
5
5
A-B
B-C
C-D
D-E
5
A
B
C
D
E
5
5
A-B
B-C
C-D
D-E
5
Less likely solution
A
B
C
D
E
5
5
5
A-B
B-C
C-D
D-E
5
A
B
C
D
E
5
5
4
2
2
A-B
B-C
C-D
D-E
1
2
A
B
C
D
E
3
3
2
A-B
B-C
C-D
D-E
1
2
A
B
C
D
E
5
5
4
2
2
A-B
B-C
C-D
D-E
1
2
A
B
C
D
E
1
3
3
A-B
B-C
C-D
D-E
1
2