C,n Official Journalofthe cAmerican Heart cAssociation
advertisement

VOL 64
DECEMBER
irculation
C
C,n Official
NO 6
1981
Journalof the cAmerican Heart cAssociation, Inc.
CURRENT TOPICS
The Relationship of Cardiac Output
and Arterial Pressure Control
ARTHUR C. GUYTON, M.D.
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
output and
pressure control
siderably in the past few years. In general, each tissue controls its own local resistance and blood flow regardless of the level of arterial pressure; the sum of the local flows then determines the venous return and cardiac
output. However, the arterial pressure is normally controlled by separate mechanisms that do not significantly
alter the cardiac output. During acute circulatory stresses, such as exercise, the arterial pressure is controlled
almost entirely by nervous reflex mechanisms; but over long periods, these reflex mechanisms fade away
because they adapt. The arterial pressure is then controlled mainly by a renal-volume-endocrine pressure control system, in which the blood volume and total peripheral resistance are manipulated slowly to adjust the
pressure.
RECENT EXPERIMENTS and analyses have led to
several rather startling concepts on the relationships
between cardiac output and arterial pressure control.
For instance, a long-term increase in total peripheral
resistance does not cause any increase in arterial pressure if there is not a concomitant increase in renal
vascular resistance; instead, cardiac output decreases.
Also, a chronic increase in blood volume causes hardly
any increase in cardiac output, but rather, usually
causes a marked increase in arterial pressure.' These
effects are almost exactly opposite to those observed
during the first few minutes after acute increases in
total peripheral resistance or blood volume.
Thus, there seems to be no logic in the way that the
body controls cardiac output and arterial pressure almost as if these controls were a problem of
metaphysics rather than of purpose.
The goal of this report is to show that there are logical systems for control of both cardiac output and
arterial pressure, and especially that cardiac output
and arterial pressure are mainly controlled for
different
The Purposes of Cardiac Output
and Arterial Pressure Control
Cardiac output and arterial pressure control are
much easier to understand if we delineate the purposes
of these controls.
Cardiac Output Control
The purpose of cardiac output control is to deliver
to the body's tissues the necessary blood flow to perform their functions. In most tissues, the need for flow
is to transport nutrients to the tissues and excreta
from the tissues. In the kidneys, the need is for
sufficient flow for proper excretory function; in the
gastrointestinal tract, it is for adequate flow for glandular secretion and for absorption; and in the skin, it
is for body temperature control. Thus, each tissue has
a certain requirement for blood flow, and the cardiac
output must keep in step with these needs.
However, the heart's capability to pump blood is
not unlimited. Even a cardiac output of two times normal, if it continues for days or weeks, seriously taxes
the long-term abilities of the heart. Therefore, the cardiac output must be only great enough to deliver to the
tissues that amount of blood flow that is required; no
more, no less. Figure 1 is an illustration of this principle. In a series of dogs, we purposely increased the cardiac output to more than two times normal by acute
infusion of blood, or we reduced the cardiac output
below normal by hemorrhage. While the cardiac output was either too high or too low, we measured the
total oxygen consumption of the animal. Increasing
the cardiac output to two times normal increased the
oxygen consumption by only a few percent. On the
away
purposes.
From the Department of Physiology and Biophysics, University
of Mississippi Medical Center, Jackson, Mississippi.
This paper was presented as the Goerge C. Griffith Scientific Lecture, Los Angeles, California, September 17, 1980.
Address for correspondence: Arthur C. Guyton, M.D., Department of Physiology and Biophysics, University of Mississippi
Medical Center, 2500 North State Street, Jackson, Mississippi
39211.
Received October 22, 1980; revision accepted April 1, 1981.
Circulation 64, No. 6, 1981.
1079
CIRCULATION
logo
Co
60
;
°.4
E-
3
It
0=
h-
0
0
pumping capacity, blood volume and vascular compliance. The chronic effect of each is often entirely
different from the acute effect.
The Acute Effect of Total Peripheral Resistance
Changes on Cardiac Output and Arterial Pressure
-/
1
VOL 64, No 6, DECEMBER 1981
'
20
40
60
80 100 120 140 160 180 200
CARDIAC OUTPUT (ml/kg/min)
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
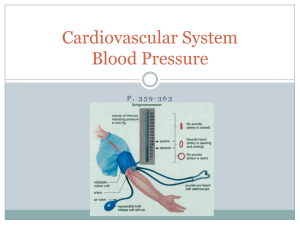
FIGURE 1. Relationship of cardiac output and total oxygen consumption by the body. The normal cardiac output is
at a level barely high enough to provide almost maximum
oxygen consumption by the body, yet using the least pumping energy of the heart to achieve this result. This figure was
drawn from data in five dogs after correcting for excess oxygen consumed by the heart at the high cardiac outputs.
other hand, decreasing the cardiac output below normal very rapidly caused a serious decrease in oxygen
utilization by the tissues. Oxygen is the most important of all the flow-limited nutrients required by the
tissues, and it is clear from this experiment alone that
the normal cardiac output is very precisely optimized
to the level that will supply essentially all the nutrient
needs of the tissues and yet to a level that gives almost
no excess flow, providing for both the needs of the
tissues and yet protecting the heart from overload.
Arterial Pressure Control
One of the obvious purposes of pressure control is
to keep the pressure high enough so that blood can
flow to all of the tissues of the body even when some of
the tissues are far above the level of the heart. For instance, in giraffes, the mean arterial pressure is regulated to a level between 200 and 300 mm Hg; this
much pressure is required to assure blood flow to the
top of the head. At the other extreme, the regulated
level of the arterial pressure in primitive fishes may be
as low as 30 mm Hg; because there are no hydrostatic
pressure gradients in fishes, this is an adequate pressure to assure blood flow to all tissues.
However, pressure control involves more than
simply assuring adequate pressure for flow to all of the
tissues. When the pressure control system is operating normally, even massive changes in blood flow in
one part of the body will hardly affect the arterial
pressure. Therefore, this also will not affect the blood
flow in other parts of the body. That is, proper arterial pressure control allows the blood flows in the
separate parts of the body to be controlled independently.
The Basic Acute Hemodynamic Mechanisms
of Cardiac Output and
Arterial Pressure Control
Four basic factors control both cardiac output and
arterial pressure: total peripheral resistance, heart
Figure 2 illustrates data from a basic experiment
that demonstrate the hemodynamic effects of acute
changes in total peripheral resistance.2 In this
experiment, two groups of dogs were used; in one
group the function of the nervous system was normal
and in the other it was abrogated by removing the animal's head and injecting the spinal cord with alcohol.
In each dog two large arteriovenous (A-V) fistulas
were opened for 6 minutes by opening both femoral
arteries directly into the adjacent femoral veins. In the
dogs with nonfunctioning nervous systems, the acute
hemodynamic effect of opening the A-V fistulas,
which greatly decreased the total peripheral
resistance, was a marked increase in cardiac output
and a decrease in arterial pressure. On a percentage
basis, the increase of cardiac output was almost exactly equal to the decrease in pressure.
Although the initial effects in dogs with intact nervous systems were almost identical to those in dogs
without, within less than 30 seconds the arterial
pressure returned about seven-eighths of the way back
toward normal, while the cardiac output increased still
a little more. Then, when the fistulas were closed, the
arterial pressure rose somewhat above normal at first,
but within another minute or so returned back to the
normal level. This overshoot in pressure was the result
of the compensatory mechanisms that had become activated during the period of the open A-V fistulas.
This A-V fistula experiment illustrates that the major circulatory control function of the nervous system
is to control arterial pressure, not to control cardiac
output. It also demonstrates that if the arterial
pressure is maintained at a normal level by the nervV
OPEN S>
FISTULsA
\s A s
100
TOTAL
PERIPHERAL 75
RESISTANCE
[% of control) I
50 L
CARDIAC
INTACT NERVOUS SYSTEM
I
!
150
OUTPUT 125
{% of control) 100
NO
NERVOUS SYSTEM
INTACT
NERVOUS SYSTEM
""""""""""
NO
NERVOUS SYSTEM
125
ARTERIAL 100
PRESSURE 75
1% of control) 75
50
INTACT NERVOUS SYSTEM
NO NERVOUS SYSTEM
0
_
2
4
.Ai
6
8- 10
12
14
16
18
MINUTES
FIGURE 2. Effect of opening an arteriovenous (A-V)
fistula on arterial pressure, cardiac output, and total
peripheral resistance in dogs with intact nervous systems and
in dogs with the nervous system destroyed. (Drawn from
data in Dobbs et a 1. 2 )
CO AND ARTERIAL PRESSURE CONTROL/Guyton
ous controls when a fistula is opened, the cardiac output will rise to a greater level than it will when the
pressure is not maintained; that is, maintenance of a
normal or nearly normal level of arterial pressure is
important not only for pressure control itself, but also
because it allows adequate blood flow through the
tissues when an abnormal factor tends to drain this
blood flow away from the tissues.
Effect on Cardiac Output and Arterial Pressure
Caused by Changing the Heart Pumping Capacity
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
5\Sllt*o.
90 00 .0
00 *0
00 00
o'..
.
~
~
,/w'
NORMAL
10C
5C
C
40
60
_.75
.75
~ ~ Normal
/
=.50
0
.5
1.0
1.5
2.0
2.5
3.0
HEART PUMPING CAPACITY (times normal)
FIGURE 4. Effect of increased heart pumping capacity on
cardiac output. This figure shows that increasing the heart
pumping capacity to above normal has essentially no effect
to increase the resting cardiac output. (Drawn from data illustrated in figure 11-7 in Guyton A C.84)
put? Figure 4 explains this; it shows an effect that has
been learned from use of extracorporeal circulatory
systems.4 Increasing the pumping capacity of the artificial heart in the extracorporeal system to two times
normal has almost no effect to increase the cardiac
output above normal. Likewise, an increase of heart
pumping capacity to three times normal, five times
normal or even greater will not increase the cardiac
output. The veins entering the chest simply collapse
when the right atrial pressure begins to fall below 0
mm Hg, which is what occurs when the heart tries to
pump more blood than is made available by the normal venous return.
Therefore, there is no reason to believe that in the
normal circulation, increasing the heart pumping
capacity above normal will increase the cardiac output
or the arterial pressure to higher than normal values.
On the other hand, when increased amounts of blood
return from the veins, an increase in pumping capacity
of the heart often then becomes essential to keep up
with the returning blood.
to
200 1
15c
1.00
.25
It is often stated that increasing the heart pumping
capacity, either by increasing the heart strength or by
increasing the heart rate, will increase the cardiac output and the arterial pressure. However, persons with
less-than-normal heart pumping capacities do not
necessarily have a low cardiac output or a low arterial
pressure. Furthermore, some heart valve operations
increase the heart pumping capacity tremendously,
although this does not cause either excess cardiac output or hypertension. Therefore, let us examine the
acute effect on circulatory dynamics of increasing the
heart pumping capacity.
Figure 3 illustrates the results when the heartpumping capacity of dogs was increased by electrically
pacing the heart to increase the heart rate from 50
beats/min up to 200 beats/min.8 The upper curve
shows the effect of the increasing heart pumping
capacity when a very large fistula existed between the
aorta and the inferior vena cava, so that there was
always an excess preload on the heart (that is, a high
right atrial pressure.) Under these conditions, the increasing heart pumping capacity increased the cardiac output very markedly.
The lower curve of figure 3 shows the effect of the
increasing pumping capacity when the circulation was
normal. Cardiac output changed almost imperceptibly. How does one explain this failure of increased
heart pumping capacity to increase the cardiac out-
250 r
°
1081
I, , ,
s
|
,
t
,
80 100 120 140 160 180 200
HEART RATE (beats/min)
FIGURE 3. Effect of heart pumping capacity (as indicated
by hear t rate) on cardiac output in normal dogs and in dogs
with lawrge arteriovenous (A-V)fistulas. In the normal dog,
changinig the heart pumping capacity had almost no effect
on caraliac output. (Drawn from data in Cowley et al.8)
The Hemodynamic Effects of Increased Blood Volume
or Decreased Vascular Compliance on Cardiac Output
and Arterial Pressure
Though changes in blood volume and vascular
compliance are known to play a very important role in
acute hemodynamic control of the circulation, the
quantitative effects of these factors are difficult to understand, partially because some of the experiments to
clarify the effects have been performed in animals with
normally functioning nervous systems and others have
been in animals either without nervous systems or with
greatly depressed nervous systems as a result of
anesthesia.
in
5 of dogs incomposite
effects recorded
Figure
of blood
which transfusions
three
series illustrates
equal to 30-40% of the dog's original blood volume
were given in only a few minutes.2' 6 In some dogs, the
function of the nervous system had been eliminated
either by total spinal anesthesia or by decapitation and
injection of the spinal cord with alcohol. In other dogs,
CIRCULATION
1082
VOL 64, No 6, DECEMBER 1981
despite the tremendous increase in cardiac output.
Yet, the nervous reflexes have almost no effect on car,1 'diac output, illustrating again that the nervous system
is geared primarily to control arterial pressure, not
ARTERIAL PRESSUREcadcoupt
without nervous system)
z
X
150
: Its§_@_8aLOOD VOLUME
L1-
t
100
ARTERIAL PRESSURE
(with nervous system)
Ch.
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
50
,______________________ _ ,,
20
40
60
MINUTES
FIGURE 5. Effect c n arterial pressure, cardiac outpout and
blood volume causecIby rapid transfusion of blood equal to
about 40% of the nor tmal blood volume. Ths experioment was
performed in dogs with and withoutfunctioning nervous
systems. Note the tremendous difference in the arterial
pressure response Mvith and without the nervous system.
(Drawn from data in Prather et al.5 and Dobbs et al.2)
01L.
-20
0
the nervous systemus were normally functional. In both
states, essentially t he same effect was observed on cardiac output - a rnarked increase in output to about
100% above noirmal. However, cardiac output
returned to normal in less than 1 hour, although the
blood volume still remained about 20% greater than
normal.
Although the presence or lack of a nervous system
had very little effect on the cardiac output response,
this did affect the arterial pressure response tremendously. Note that in the absence of the nervous system
the arterial pressure rose about 130%, while it rose
only about 15% when the nervous system was intact.
Yet, whether the nervous system was intact or not
intact, the pressure still returned essentially to normal
within the first hour.
Several important lessons may be learned from the
experiment illustrated in figure 5. First, the basic
hemodynamic effect of increasing the blood volume is
to increase the cardiac output markedly, and this in
turn increases the arterial pressure markedly.
However, if the nervous reflex pressure control
mechanisms are fully functional, the arterial pressure
will be reflexly prevented from rising very much despite the tremendous increase in the blood volume and
It is also significant that the blood volume had
fallen from its peak of 40% above normal to only 20%
above normal 1 hour after the transfusion; yet despite
this excess 20% of volume, both the cardiac output and
arterial pressure were at that time essentially normal.
Simultaneous measurements of the so-called mean
circulatory filling pressure were also made in these
same experiments." To make these measurements,
heart pumping is stopped completely for a short
period until the pressure becomes the same all through
the circulation. The pressure level at this point is the
mean circulatory filling pressure, which is a measure
of how tightly the circulatory system is filled with
blood. In the first few minutes after the transfusion,
this value had increased to about three times normal
because of all the extra blood in the circulation. However, 1 hour later the mean circulatory filling pressure
had returned entirely to normal even though the blood
volume was still 20% above normal. This illustrates
that the circulatory system itself had enlarged during
this hour, with compliance increasing enough to accommodate the extra 20% blood volume. Thus, an increase in compliance can nullify the hemodynamic
effects of an increase in blood volume. This is one of
the reasons the relationships between blood volume
and circulatory function are so difficult to understand, especially since it is almost impossible to measure circulatory compliance.
The most important principle illustrated by these
experiments is that in the absence of the nervous
reflexes the cardiac output and arterial pressure are
both highly responsive to changes in blood volume.
However, when the circulatory reflexes are fully func-
tional, these reflexes can maintain almost exactly normal arterial pressure despite marked changes in blood
volume.
Cardiac Output and Arterial Pressure During Exercise:
An Example of Complex Short-term Control
The two upper curves in figure 6 illustrate the
approximate changes in cardiac output and arterial
pressure in normal dogs when they begin to exercise at
a moderately heavy rate.6 Note the 2.5-fold increase in
cardiac output and the 50% increase in arterial
pressure. The next two curves illustrate the effect on
cardiac output and arterial pressure in sympathectomized dogs caused by exercise at about the maximum level that these dogs could tolerate.7 The cardiac output increased only 32%, while the arterial
pressure fell about 21%. Thus, the nervous system
obviously plays a major role in the capability of an
exercising animal or person to achieve both greatly increased cardiac output and moderately increased arterial pressure during exercise.
The lowerest curve in figure 6 shows the effect of exercise on total peripheral resistance in both the normal
and the sympathectomized dogs. In both instances,
CO AND ARTERIAL PRESSURE CONTROL/Guyton
LM2L\..
CARDIAC OUTPUT (normal)
250 r
-
=
t-X- E R C 1 S. 1E
200
ARTERIAL PRESSURE
150
[normal)
LI&-
CARDIAC OUTPUT
z 100
(sympathectomy)
ARTERIAL PRESSURE (sympathectomy)
TOTAL PERIPHERAL RESISTANCE
(normal & sympathectomyJ
sL 50
0
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
-1
0
1
2
3
4
5
MINUTES
FIGURE 6. Efflect of exercise on cardiac output, arterial
and total peripheral resistance in normal dogs and
in sympathectomized dogs. (Drawn from data in Barger et
al.6 and Ashker and Hamilton.7)
pressure
the change in total peripheral resistance was essentially the same.
At the onset of exercise, two major control events
occur almost simultaneously: The resistance to blood
flow through the contracting muscles decreases
markedly because of local factors in the muscles
directly dilating the blood vessels,8 and the sympathetic nervous system constricts the capicitance vessels
of the circulation, especially the veins, and it also constricts the arterioles in those parts of the body besides
the exercising muscles." This sympathetic drive to the
circulation derives at least partly from signals
generated in the central nervous system during the
course of exercise and probably partly from reflexes
that originate in the active muscles themselves. Dogs
that had been sympathectomized experienced only one
of the above control factors, the very large decrease in
resistance in the muscles, while the normal dogs had
the benefit of the sympathetic drive. The decreased
muscle resistance decreased the total peripheral
resistance by about 40%, which also decreased the
arterial pressure and raised the cardiac output, but
only by 32%. Obviously, if the arterial pressure had
not fallen, far more blood would have flowed through
the greatly dilated muscle blood vessels, and the cardiac output would have been much greater. Furthermore, if the arterial pressure had actually risen, as occurred in the normal dogs with normal sympathetic
signals, then the cardiac output would have risen still
much more. This is the effect that was observed in the
normal dogs: an increase in cardiac output of 130% instead of the almost insignificant increase of 32% seen
in the sympathectomized dogs.
Yet, the total peripheral resistance changes were
almost equal, whether or not the dogs were sympa-
1083
thectomized. The basic difference between the sympathectomized and the normal animal depends in the
ability of the normal animal to increase its arterial
pressure despite the marked decrease in total peripheral resistance. This undoubtedly resulted from increased venous return and cardiac output caused by a
sympathetically stimulated decrease in vascular compliance and an increase in cardiac pumping. But, by
way of circular logic, the increase in arterial pressure
in the normal animal also increased the flow through
the peripheral circulation, allowing the very large increase in venous return in the normal compared with
the slight increase in return in the sympathectomized
dog.
Thus, arterial pressure control is exceedingly important to allow adequate blood flow to those parts of
the body where vasodilatation occurs. The vasodilatation usually results not from direct effects of nervous
signals, but from local changes in the tissues, such as
increased metabolism, that relax the blood vessels.
However, if the arterial pressure is not kept at a normal level, or even raised above normal as occurs during exercise, then the local vasodilatation of the blood
vessels may not be enough in itself to provide the
needed local blood flow.
Long-Term Control of Cardiac Output and
Arterial Pressure: The Importance
of Very Slight Blood Volume Changes
Long-term control of cardiac output and arterial
pressure is quite different from short-term control for
three reasons: (1) The nervous reflexes adapt (that is,
they become inoperative as controllers) within a few
hours to a few days after an acute circulatory
change.lc'l2 (2) Blood flow autoregulation occurs in
almost all tissues of the body, which returns the blood
flows in these tissues essentially to normal regardless
of what happens to the arterial pressure.13~16 (3) The
kidneys respond very markedly to changes in arterial
pressure, increasing their output of salt and water at
higher pressures and decreasing their output at lower
pressures."'-8 These three factors altogether make
blood volume extremely important in long-term circulatory control.
Effect of Adaptation of the Circulatory Reflexes
The baroreceptor reflex is a typical arterial pressure-controlling reflex that every physician knows,
but other reflexes also originate in the heart, the lungs,
and in the basal regions of the brain that also play very
important roles in pressure control. However, a consideration of the baroreceptor reflex will illustrate the
effect of pressure receptor adaptation on long-term
control of the circulation.
When a factor such as an increase in blood volume
increases the arterial pressure, the rising pressure immediately stimulates the baroreceptors. This in turn
causes reflex dilatation of the peripheral circulation
and at the same time decreased strength of heartbeat,
and these factors together prevent much of the rise in
arterial pressure that otherwise would occur.
1084
CIRCULATION
However, during the next 24-72 hours, the baroreceptors themselves gradually stop sending excess signals
to the brain even though the pressure is still high.'0 12
Therefore, the reflex effects that had been preventing
the rise in pressure disappear. As a result, the full
effect of the increased blood volume to increase arterial pressure then becomes manifest.
This effect of adaptation of the nervous reflexes to
sensitize the arterial pressure response to changes in
volume is illustrated in figure 5. When the nervous
reflexes were operative, the increase in blood volume
had little effect on arterial pressure. However, in the
absence of the reflexes, which is the state that exists
after the reflexes have adapted, the same change in
volume increased the arterial pressure eight times as
much.2
Control of Local Blood Flow by the Autoregulation
Mechanism
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
The local ability of each tissue to control its own
blood flow is called autoregulation. Autoregulation is
not instantaneous. In some tissues, such as the
kidneys, most of the autoregulation response takes
place within less than 30 seconds. In most other
tissues, the autoregulatory response during the first
minute is relatively weak and becomes progressively
more intense with time.'3 14 The initial autoregulation is caused by contraction of the smooth muscle
walls of the blood vessels when the blood flow is too
great or relaxation when the blood flow is too low.
However, over a period of weeks and months, actual
structural narrowing or enlargement of blood vessels
occurs to return the blood flow back toward normal.'5' 19, 20 Thus, by both these means, the local blood
flows seem to be progressively adjusted to the needs of
the tissues.
Why does this autoregulatory mechanism make
volume control of the circulation more sensitive?
When the blood volume increases and this in turn increases arterial pressure and cardiac output, the initial autoregulation in the entire circulation is very
slight because some blood vessels are dilated as a
result of the rising pressure at the same time that other
vessels begin to constrict as a result of autoregulation. Therefore, the total peripheral resistance hardly
changes at first.'3 Consequently, the high cardiac output can persist at least temporarily. Yet, over time,
the autoregulatory response becomes progressively
enhanced, and the total peripheral resistance increases
steadily in an attempt to decrease the local blood flows
and the cardiac output back toward normal. However,
as first observed by Markwalder and Starling in 1914,
excess volume keeps the heart pumping an excess cardiac output despite progressively increasing total
peripheral resistance.2' The increasing total peripheral
resistance has only a small effect to decrease the cardiac output back toward normal. Instead, it simply
raises the arterial pressure to a higher level. Thus, over
a period of days and weeks only a few percent increase
in volume may increase the cardiac output only a few
percent, but nevertheless increase the arterial pressure
as much as 50%.
VOL 64, No 6, DECEMBER 1981
The Kidney Mechanism for Control of Blood Volume
and Arterial Pressure: "Pressure Diuresis
and Pressure Natriuresis"
The arterial pressure itself is one of the major
factors that affect the rate at which the kidneys excrete
water and salt. Experiments in hundreds of laboratories have demonstrated that a decrease in arterial
pressure to about 60% of normal decreases the urinary
output almost to zero.'"-18 On the other hand, an increase in arterial pressure to about 20% above normal
approximately doubles urinary output, and a doubling
of arterial pressure increases urinary output an
average of about sevenfold, both the water output and
salt output participating in these changes. The very
great effect of pressure on water output is called
pressure diuresis and the effect on salt output is called
pressure natriuresis.
Therefore, when the arterial pressure rises above
normal in the person with normal kidneys, the body
fluid volumes will continue to decrease until the arterial pressure returns exactly back to normal.
Conversely, when the pressure falls below normal the
kidneys retain water and salt, and this retention occurs
until the pressure rises again exactly back to normal.
Thus, the kidneys play a central role in a volume
feedback mechanism for controlling arterial pressure.
Figure 7 shows changes in cardiac output, arterial
pressure, and urinary output after transfusion of blood
4000< Dc
UI-.-
3000-
:X o E
20001000-
a-
ZIFN
E 0m E
JLJ
.:
cr
W E
75]
1
50 INFUSION PERIOD
M
0 10 20 30 40 s0 60
1
120
Ir-1
T I ME (minutes)
FIGURE 7. Function of the kidney-blood volume feedback mechanism to return the arterial pressure back to normal after transfusion of blood into dogs without nervous
reflexes. The transfusion increased the blood volume approximately 30% and was administered in a period of 4
minutes. The dogs were made areflexic by removing their
heads and injecting their spinal cords with alcohol.
(Modified from Dobbs WA Jr.22)
CO AND ARTERIAL PRESSURE CONTROL/Guyton
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
into dogs equal to 30% of their blood volume.22 The
nervous reflexes had been blocked so that the full
effect of the volume could be observed. Note the
marked increases in arterial pressure and cardiac output, similar to those in figure 5, but note also the 12fold increase in urinary output. This excessive urinary
output continued as long as the arterial pressure
remained above normal. However, as the arterial
pressure returned toward normal, so also did the
urinary output. Thus, this mechanism is an extremely
powerful one to return the arterial pressure all the way
back toward its normal level. This phenomenon is an
especially important characteristic of this mechanistn
that is not manifest by any other arterial pressure control system. It is called the principle of "infinite gain"
for control of blood pressure by the kidney-volumepressure control mechanism.l
Thus, even stnall changes in blood volume are extremely important in long-term control of the arterial
pressure; but far greater changes in volume are required in short-term control to achieve the same
results.
Role of Total Peripheral Resistance in the Long-term
Control of Cardiac Output and Arterial Pressure
Although an acute change in total peripheral
resistance affects cardiac output and arterial pressure
about equally (fig.-2), this is not the case when the
total peripheral resistance remains chronically increased or decreased. Figure 8 shows the effects of
long-term total peripheral resistance changes on cardiac output and arterial pressure. This figure was constructed from measurements of arterial pressure and
cardiac output in many different clinical conditions in
which the total peripheral resistance was chronically
decreased or chronically increased.28 For instance,
such factors as beriberi, A-V shunts, anemia and
.-.__
200
_P ~150
c
=
°00
_
=.I
A ..
TOTAL PERIPHERAL RESISTANCE (per cent
of
normal)
FIGURE 8. Relationship of different levels of total peripheral resistance to the long-term levels of arterial pressure and cardiac output in various clinical conditions that
cause primary decreases or increases in total peripheral
resistance. (Reprinted with permission from Guyton A C.34)
1085
thyrotoxicosis cause a chronic decrease in total
peripheral resistance. At the other extreme, hypothyroidism or removal of all four limbs of a person
can caUse a chronic increase in total peripheral resistance. Yet, the measurements show that in none of
these conditions is the arterial pressure abnormal.
Instead, the cardiac output changes exactly inversely
to the changes in total peripheral resistance because
when the arterial pressure rises above or falls below
the normal level, the normally functioning kidneys
will either eliminate fluid from the body or retain fluid
until the pressure returns back to the original level.
This again is a manifestation of the infinite-gain principle of pressure control by the kidney-volumepressure system.
A Complex Example of Long-term Cardiac Output
and Arterial Pressure Control: Development
of Volume-loading Hypertension
Many experiments have shown that long continuation of excess blood volume in a circulatory system
will almost invariably lead to severe hypertension.24-28
Ordinarily, though, an excess volume is difficult to
maintain in the circulation for more than a few hours
because the kidneys are extremely effective in removing the excess volume. Indeed, the salt and water intake of a person can be increased to as much as 10-15
times normal with no more than a 5-10-mm Hg pressure rise simply because of this vast capacity of the
kidneys to eliminate the excess water and salt.
Nevertheless, under special experimental conditions it
is possible to cause long-term volume loading, and this
seems always to cause hypertension if all other aspects
of the circulation are normal. Though not all investigators agree on the successive events in the
development of this volume-loading hypertension, the
following analysis fits with the available data.
Figure 9 presents a composite set of curves illustrating the hemodynamic changes during the onset of
typical volume-loading hypertension. These curves
were normalized from several dog experiments in
which the kidney mass was first reduced to approximately 30% of normal so that the kidneys could not
excrete sodium and water rapidly.24-28 Then, several
weeks later, at "zero" time, the dogs were placed on a
salt intake approximately five to seven times normal.
Immediately, the extracellular fluid volume, blood
volume, mean circulatory filling pressure, pressure
gradient for venous return, and cardiac output all increased 20-50%. At the same time, the arterial pressure began to rise, but much more slowly than the
other variables. The reason for this slowness was that
the nervous reflexes decreased the total peripheral
resistance below normal, which nullified much of the
pressure rise. Yet, over a period of days the nervous
reflexes adapted and thereby became inoperative. At
the same time, the excess cardiac output caused progressive autoregulatory increase in the vascular
resistance throughout the body. These effects - the
diminution of the reflex effects and the autoregulation
- then increased the total peripheral resistance. This
CIRCULATION
1086
33%
20
EXTRACELLULAR 9 8
FLUID VOLUME 178
(liters)
16
15
60
BLOOD VOLUME 5.55%
Conditions in Which the Long-Term Control
Mechanisms Fail
20%
(liters)
5.0
MEAN
CIRCULATORY
FILLING
PRESSURE
(mmHg)
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
TOTAL
PERIPHERAL
RESISTANCE
(mmHg/liter /
min)
ARTERIAL
PRESSURE
(mmHg)
- -
--
60 %
16
14
12
10
20%
*___________________
28
26
24
22
20
18
-11%
150 SET-POINT ELEVATED
140
130
120
22.5 %
110
100
-----
38%
-----
-----
45%
-
0
VOL 64, No 6, DECEMBER 1981
4
8
12
16
D A YS
FIGURE 9. A composite figure of the results from many
which volume-loading hypertension was
caused by decreasing the renal mass to 30% of normal and
several weeks later increasing the salt and water intake to
five to seven times normal. Note that the final result was
hypertension in which the cardiac output was essentially
normal but the total peripheral resistance was greatly increased. (Reprinted with permission from Guyton A C.34)
experiments in
in turn caused all of the volume factors and cardiac
output factors to return toward normal even though
the arterial pressure remained greatly elevated.
Thus, the initial cause of the volume-loading hypertension is excess volume and excess cardiac output.
However, secondary changes in total peripheral
resistance return the cardiac output and fluid volumes
back to or very near to normal while substituting instead a high total peripheral resistance.
One of the most important features of this analysis
is that, in the long run, cardiac output is controlled
relatively independently of the arterial pressure. That
is, the cardiac output returns so nearly to normal that
one actually can not tell from experiments that it is
abnormal. On the other hand, if the heart is strong
enough to withstand the extra pressure load, the arterial pressure will eventually rise high enough so that
the impaired kidneys can then excrete the greatly increased daily load of water and salt.
So far, this report has presented the long-term control of cardiac output and arterial pressure in a person
who has a normal circulatory system. However, under
abnormal conditions, these mechanisms frequently
fail and may lead to persistent tissue ischemia when
blood vessels have become so contracted that they
cannot possibly vasodilate, heart failure when the
heart cannot sustain an increased pressure or increased cardiac output load, or edema when the capillary system cannot retain fluid in the circulating
blood.
The long-term volume-renal mechanism of pressure control has two functional requirements. First,
the heart be strong enough to increase the cardiac output at least slightly and the arterial pressure considerably when the blood volume increases. This is
well-known from animal experiments but even more
so from clinical practice, for infusion of fluid or blood
into a patient with a failing heart, or even eating large
amounts of salt, all of which tend to increase blood
volume in the normal person, will lead to loss of fluid
from the capillaries into the tissue spaces, causing
edema rather than increased arterial pressure. This is
a well-known characteristic of congestive heart
failure, representing failure of the system to regulate
either cardiac output or arterial pressure normally.
Second, the systemic capillaries must be able to
hold fluid in the circulation, preventing excessive
filtration into the interstitial spaces. It is not only in
heart failure that the capillaries cannot retain fluid in
the circulation. The clinical conditions of anaphylaxis
and nephrosis also often make it-difficult or impossible
to maintain even a normal blood volume, much less
excess volume, despite massive fluid therapy; instead,
the fluid rapidly transudes into the tissues - in the
first instance because of increased capillary porosity
and in the second because of decreased plasma colloid
osmotic pressure. In both conditions, excess infusion
or intake of fluid and salt lead only to increased
edema, not to increased arterial pressure.
Another condition that makes it difficult for the
capillary system to maintain an adequate blood
volume is paralysis of the arterioles throughout the
body. For instance, animals whose arteriolar tone has
been acutely paralyzed as a result of total spinal
anesthesia are incapable of maintaining the arterial
pressure above 60 mm Hg despite transfusion of blood
equal to more than 50% of the animal's normal control volume.29 Instead, fluid leaks so rapidly out of the
circulation into the interstitium that within 20 minutes
extreme hemoconcentration occurs while the blood
volume returns essentially to normal and the arterial
pressure equilibrates below 60 mm Hg.
Therefore, the volume-kidney-pressure control
mechanism can fail in many ways. In some of these instances the hemodynamics of the failure are known; in
others, proper explanations are not available. Onesti
et al.30 performed an especially interesting study and
showed that increasing the extracellular fluid volumes
CO AND ARTERIAL PRESSURE CONTROL/Guyton
of totally nephrectomized patients caused hypertension in some patients but not in others.30 Those in
whom hypertension failed to occur developed
peripheral edema instead. Unfortunately, not enough
information was available from these patients to tell
whether' one of the known causes of failure of the
system might have been' operative.-There might have
been something about the humoral or hormonal
makeup of these patients that affected either the
arterioles or the capillaries to prevent retention of
fluid in the circulation. This type of problem
represents one of the foremost areas of research still in
process for defining the long-term mechanisms of circulatory control.
Role of Nervous, Hormonal, and Electrolyte Systems
in Long-term Regulation of the Circulation
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
Although the emphasis of this paper has been that
cardiac output and arterial pressure control, over the
long-term, are mainly controlled by separate hemodynamic mechanisms, there are special conditions under which nervous, hormonal and electrolyte systems
play powerful roles in long-term regulation of both of
these.
Recent experiments have shown that the human being can tolerate changes in sodium intake from
10-1500 mEq per day, a 150-fold change, with only a
10-20-mm Hg arterial pressure change."' Yet, animal
experiments in our laboratory have shown that
blockade of the renin-angiotensin system makes this
wide range of tolerance no longer' possible;23' 32 instead, the pressure then changes about 10 times as
much and almost in direct proportion to the changes
in sodium intake. Therefore, the renin-angiotensin
system, along with its associated aldosterone system,
plays an exceedingly'important long-term role in finetuning the basic hemodynamic pressure control
system.
Although circulatory reflexes were emphasized as
extremely important short-term controllers of arterial pressure, they seem to adapt within a few days and
therefore probably do not play a significant role in
long-term pressure control. Nevertheless, there are
other aspects of nervous control of the circulation
besides the reflexes. For instance, minute-by-minute
or hour-by-hour bursts of sympathetic activity often
result from stress situations. Recent experiments have
illustrated that the hormones released by the sympathetic nervous system, norepinephrine and epinephrine, can have not only short-term effects on the
kidneys, but long-term effects as well,38 and these
could easily lead to a long-term increase in the arterial pressure.
Thus, in addition to the basic circulatory hemodynamic and renal hydraulic mechanisms for longterm control of the circulation, the body has also
developed still other special mechanisms for finetuning the system. When these special mechanisms fail
to function properly, they too can cause clinical abnormalities of cardiac output or arterial pressure control.
1087
Conclusions
The basic theory of long-term circulatory control is
that'the tissues control their own blood flows and also
the cardiac output by changing the resistances
throughout the body. A separate system controls the
arterial pressure independent of cardiac output control. This system is based mainly on long-term control
of blood volume by the kidneys. Though an acute increase in volume increases the cardiac output
markedly, over a period of days to weeks the resultant
excess flow through each tissue leads to autoregulation; this increases the local resistances and returns the
local flows, as well as the cardiac output, back to normal; but this elevation of the peripheral resistance now
maintains a'high arterial pressure. Thus, in a roundabout way, a small change in blood volume may cause
a large change- 'in arterial pressure.
Superimposed onto this intrinsic long-term, hemodynamic control system of the circulation are important hormonal and' nervous mechanisms that normally
fine-tune the system; but they themselves can cause
abnormal cardiac outputs or arterial pressures when
they malfunction.
References
1. Guyton AC, Coleman TG, Cowley AW Jr, Manning RD Jr,
Norman RA Jr, Ferguson JD: A systems analysis approach to
understanding long-range arterial blood pressure control and
hypertension. Circ Res 35: 159, 1974
2. Dobbs WA Jr, Prather JW, Guyton AC: Relative importance
of nervous control of cardiac output and arterial pressure. Am J
Cardiol 27: 507, 1971
3. Cowley AW Jr, Guyton AC: Heart rate as a determinant of cardiac output in dogs with arteriovenous fistula. Am J Cardiol 28:
321, 1971
4. Guyton AC, Lindsey AW, Abernathy JB, Richardson TQ:
Venous return at various right atrial pressures and the normal
venous return curve. Am J Physiol 189: 609, 1957
5. Prather JW, Guyton AC, Taylor AE: Effect of blood volume,
mean circulatory pressure, and stress relaxation on cardiac output. Am J Physiol 216: 467, 1969
6. Barger AC, Richards V, Metcalfe RJ, Gunther B: Regulation
of the circulation during exercise; cardiac output (direct Fick)
and metabolic adjustments in the normal dog. Am J Physiol
184: 613, 1956
7. Ashkar E, Hamilton WF: Cardiovascular response to graded
exercise in the sympathectomized-vagotomized dog. Am J
Physiol 204: 291, 1963
8. Barcroft HA, Dornhorst AC, McClatchey HM, Tanner IM:
On the blood flow through rhythmically contracting muscle
before and during release of sympathetic vasoconstrictor tone. J
Physiol 117: 391, 1952
9. Folkow B: Nervous control of the blood vessels. Physiol Rev
35: 629, 1955
10. McCubbin JW, Green JH, Page IH: Baroreceptor function in
chronic renal hypertension. Circ Res 4: 205, 1956
11. Kezdi P, Wennemark JR: Baroreceptor and sympathetic activity in experimental hypertension in the dog. Circulation 17:
785, 1958
12. Kreiger EM: Time course of baroreceptor resetting in acute
hypertension. Am J Physiol 218: 486, 1970
13. Granger HF, Guyton AC: Autoregulation of the total systemic
circulation following destruction of the central nervous system
in the dog. Circ Res 25: 379, 1969
14. Wakim KG, Slaughter 0, Clagett OT: Studies on the blood
flow in the extremities in cases of coarctation of the aorta:
determination before and after excision of the coarctate region.
May Clin Proc 23: 347, 1948
1088
CIRCULATION
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
15. Dollery CT, Henbind P, Paterson JW, Romalho PS, Hill DW:
Opthalmoscopic and circulatory changes in focal retinal
ischemia. Br J Ophthalmol 50: 285, 1966
16. Selkurt EE, Hall PW, Spencer MP: Influence of graded arterial pressure decrement on renal clearance of creatinine, pamino hippurate and sodium. Am J Physiol 159: 369, 1949
17. Thompson DD, Pitts RF: Effects of alterations of renal arterial
pressure on sodium and water excretion. Am J Physiol 168:
490, 1952
18. Shipley RE, Study RS: Changes in renal blood flow, extraction
of insulin, gomerular filtration rate, tissue pressure, and urine
flow with acute alterations of renal artery blood pressure. Am J
Physiol 167: 676, 1951
19. Folkow B: The hemodynamic consequences of adaptive structural changes of the resistance vessels in hypertension. Clin Sci
41: 1, 1971
20. Folkow B, Hallbick M, Lundgren Y, Sivertsson R, Weiss L:
Importance of adaptive changes in vascular design for establishment of primary hypertension, studied in man and in spontaneously hypertensive rats. Circ Res 32: (suppl I): 1-2, 1973
21. Markwalder J, Starling EH: On the constancy of systolic output under varying conditions. J Physiol 48: 348, 1914
22. Dobbs WA Jr: Relative Importance of Nervous and Intrinsic
Mechanical Factors in Cardiovascular Control Systems. Ph.D.
thesis, University of Mississippi School of Medicine, Jackson,
Mississippi, 1970
23. Guyton AC: Arterial Pressure and Hypertension. Philadelphia, WB Saunders, 1980
24. Langston JB, Guyton AC, Douglas BH, Dorsett PE: Effect of
changes in salt intake on arterial pressure and renal function in
nephrectomized dogs. Circ Res 12: 508, 1963
VOL 64, No 6, DECEMBER 1981
25. Coleman TG, Guyton AC: Hypertension caused by salt loading in the dog. III. Onset transients of cardiac output and other
circulatory variables. Circ Res 25: 152, 1969
26. Cowley AW Jr, Guyton AC: Baroreceptor reflex effects on
transient and steady-state hemodynamics of salt-loading
hypertension in dogs. Circ Res 36: 536, 1975
27. Manning RD Jr, Coleman TG, Guyton AC, Norman RA Jr,
McCaa RE: Essential role of mean circulatory filling pressure
in salt-induced hypertension. Am J Physiol 236: R40, 1979
28. Manning RD Jr, Guyton AC, Coleman TG, McCaa RE:
Hypertension in dogs during antidiuretic hormone and hypotonic saline infusion. Am J Physiol 236: H314, 1979
29. Guyton AC, Batson HM Jr, Smith CM Jr: Adjustments of the
circulatory system following very rapid transfusion or
hemorrhage. Am J Physiol 164: 351, 1951
30. Onesti G, Kim KE, Greco JA, del Guercio ET, Fernandes M,
Schwartz C: Blood pressure regulation in end-stage renal disease and anephric man. Circ Res 36 (suppl I): 1-145, 1975
31. Murray RH, Luft FC, Bloch R, Weyman AE: Blood pressure
responses to extremes of sodium intake in normal man. Proc
Soc Exp Biol Med 159: 432, 1978
32. DeClue JW, Guyton AC, Cowley AC Jr, Coleman TG, Norman RA Jr, McCaa RE: Subpressor angiotensin infusion, renal
sodium handling, and salt-induced hypertension in the dog. Circ
Res 43: 503, 1978
33. Cronin RE, deTorrente A, Miller PD, Bulger RE, Burke JJ,
Schrier RW: Pathogenic mechanisms in early norepinephrineinduced acute renal failure: emotional and histological correlates of protection. Kidney Int 14: 115, 1978
34. Guyton AC: Cardiac Output and Its Regulation, 2nd ed. Philadelphia, WB Saunders, 1973
The relationship of cardiac output and arterial pressure control.
A C Guyton
Downloaded from http://circ.ahajournals.org/ by guest on September 29, 2016
Circulation. 1981;64:1079-1088
doi: 10.1161/01.CIR.64.6.1079
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1981 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/64/6/1079
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/