Does access to an Advanced Nurse Practitioner in times of crisis
advertisement

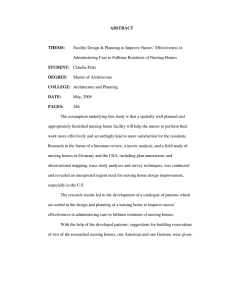
Does access to an Advanced Nurse Practitioner in times of crisis reduce urgent care activity for nursing home residents? Angela Parkes Background Background • Urgent care activity increasing in UK particularly for most vulnerable • Residents of NHs have high level of need which makes them more vulnerable Centre for Policy on Aging (2012): • 51% of residents were over 85 • 10% were 95 and over • 51% were categorised as frail elderly • 41% were categorised as requiring dementia care Evidence • Older residents were more likely to be conveyed to and admitted to hospital (Crilly et al, 2011; Graverholt et al, 2011; Kruger et al, 2011; Quinn, 2011) • People had multiple attendances (Graverholt et al, 2011; Gruneir et al, 2010) • Interventions within home provide reductions in admissions to hospital (Graverholt et al, 2014; Ploeg et al, 2013) • Residents with ACP shown to have lower admission rates than those that did not (Graverholt et al, 2014; Lamb et al, 2011; Ploeg et al, 2013) • Medication reviews resulted in lower rates of admission (Graverholt et al, 2014) • Access to nurse practitioners providing enhanced support. Residents felt supported in decision making, the care was more responsive to their needs and hospital admissions decreased (Ploeg et al, 2013) Evidence A number of conditions were identified as avoidable: • Poor responsiveness (Carter et al, 2009) • Pneumonia (Carter et al, 2009; Gruneir et al, 2010; Lamb et al, 2011) • Urinary Tract Infection (Gruneir et al, 2010; Lamb et al, 2011) • Falls (Gruneir et al, 2010; Lamb et al, 2011) Local data: • 55% of ambulance callouts related to general illness, breathing difficulties or falls and could be avoided or minimised with increased support Project Overview Pilot project overview • ANPs who are senior decision makers supported by Care of the Elderly consultant • Rapid response in times of crisis • Virtual ward rounds • Team to deliver complementary service not replace an existing one • Safety of residents could not be compromised • CCG and provider would need to evidence success Project Evaluation Evaluation - Data • A&E attendances no investigation and no treatment reduced by 13% • Only 8 emergency admissions from the homes during pilot • Average of 0.15 admissions per home per month. Other homes averaged 2.04 per month • Expanding service to all nursing homes could reduce admissions by 68 per month • Six months emergency admission costs show a reduction of £91,902 Case studies • Edith • Has Dementia • Is mobile with walker • Dizzy and pale in morning • Low blood pressure • Home called ambulance • Experienced another episode • Team called instead • Able to remain in home • Continue to monitor • • • • • Team got there first Assessed Edith Diverted ambulance Reviewed medication Developed care plan • • • • Tony Advanced Parkinson’s Lucid intervals Preceding year 6 A&E and 2 emergency admissions • 3 weeks later withdrawn and unresponsive • No infection • End phase • Care plan enforced • Died peacefully 5 days later • Team reviewed • Discussed care with Tony and next of kin • Wish to remain at NH • GP to add to palliative care list • • • • 3 weeks later deteriorated Urine test showed infection Administer antibiotics No admission required Recommendations and Progress • Implement home in reach team across city 1 • Extend hours of home in reach team 2 Projected costs and savings for HIT from business case 600,000 419,741 400,000 200,000 0 -200,000 Costs Gross savings -400,000 -600,000 -800,000 -577,175 Net savings -157,970 3 • Additional service that reviews medication of care home residents Actual costs and savings for medication review project £60,000 £40,896 £40,000 £20,000 £0 -£20,000 Costs Gross savings Net savings -£40,000 -£60,000 -£80,000 -£84,882 -£100,000 -£120,000 -£140,000 -£125,778 4 • Implement a service to ensure all residents have advance care plans in place HIT for nursing homes Evaluate ? GP link to some care homes References Carter, L., Skinner, J. and Robinson, S. (2009) Patients from care homes who attend the emergency department: could they be managed differently Centre for Policy on Ageing (2012) A profile of residents in BUPA care homes: results from the 2012 BUPA census Crilly, J., Chaboyer, W., Wallis, M., Thalib, L. and Polit, D. (2011) An outcomes evaluation of an Australian hospital in the nursing home admission avoidance programme. Graverholt, B., Riise, T., Jamtvedt, G., Ranhoff, A., Kruger, K. and Nortvedt, M. (2011) Acute hospital admissions among nursing home residents: a population based observational study Graverholt, B., Forsetlund, L. and Jamtvedt, G. (2014) Reducing hospital admissions from nursing homes: a systematic review. Gruneir, A., Bell, C., Branstill, S., Schull, M., Anderson, G. and Rochon, P. (2010) Frequency and pattern of emergency department visits by long term care residents: A population study. Kruger, K., Jansen, K., Grimsmo, A., Eide, G. and Geiting, J. (2011) Hospital admissions from nursing homes: Rates and reasons. Lamb, G., Ouslander, J., Tappen, R., Herdan, L., Diaz, S., Roos, B., Grabowski, D. and Banner, A. (2011) Interventions to reduce hospitalisations from nursing homes: Evaluation of INTERACT II collaborative quality improvement project. Ploeg, J., Kaasalainen, S., McAiney, C., Martin-Misener, R., Donald, F., Wickson-Griffiths, A., Carter, N., SangsterGormley, E., Martin, L., Brazil, K. and Taniguchi, A. (2013) Resident and family perceptions of the nurse practitioner role in long term care settings: a qualitative descriptive study. Quinn, T. (2011) Emergency admissions from care homes: Who, why and what happens? A cross-sectional study.