Unit 3 Autoimmunity Part 2 Systemic Lupus Erythematosus Part 3 Rheumatoid Arthritis
advertisement

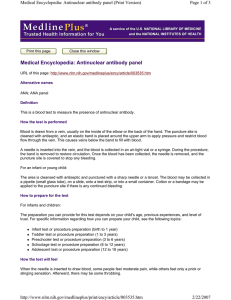
Unit 3 Autoimmunity Part 2 Systemic Lupus Erythematosus Part 3 Rheumatoid Arthritis Terry Kotrla, MS, MT(ASCP)BB Expectation Students are expected to know: Signs and symptoms, especially part of body affected Age and sex if appropriate Tests to diagnose Treatment Systemic Lupus Erythematosus Chronic, systemic inflammatory disease caused by immune complex formation. The word "systemic" means the disease can affect many parts of the body. Pathophysiology associated with clinical features secondary to immune complexes depositing in tissues resulting in inflammation. Parts of the body affected include: the joints, skin, kidneys, heart, lungs, blood vessels, and brain. Systemic Lupus Erythematosus Peak age of onset is 20 to 40 years of age. Found more frequently in women. Has both genetic and environmental factors. Often difficult to diagnose. “Great imitator” as it mimics or is mistaken for other illnesses. Can be fatal but survival rates increasing. SLE Clinical Signs Extremely diverse and nonspecific. Joint involvement most frequent signs are polyarthralgia and arthritis which occur in 90% of patients. Skin manifestations next most common. Erythematosus rash may appear. Most classic is butterfly rash. Symptoms of SLE SLE Butterfly Rash The source of the name "lupus" is unclear. All explanations originate with the characteristic butterfly-shaped malar rash that the disease classically exhibits across the nose and cheeks. Various accounts, some doctors thought the rash resembled a wolf pattern. In other accounts doctors thought that the rash, which was often more severe in earlier centuries, created lesions that resembled wolf bites or scratches. Stranger still, is the account that the term "Lupus" didn't come from latin at all, but from the term for a French style of mask which women reportedly wore to conceal the rash on their faces SLE Clinical Signs Renal involvement very common. Caused by deposition of immune complexes in kidney tissue. Leads to renal failure, most common cause of death. Other systemic effects: Cardiac Central nervous system Liver Hematologic abnormalities Immunologic Findings Lupus Erythematosus (LE) cell, neutrophil which has engulfed the antibody-coated nucleus of another cell. First classic test to aid in diagnosis. Not utilized anymore, may still see in older references. Over activity of B cells main immunologic characteristic. Antinuclear antibodies produced. More than 28 antibodies associated with LE have been identified. Level of antibody production correlates with severity of symptoms. Estrogen enhance B cell activation. LE Cell "LE cell" test which has value only in demonstrating how the concept of autoantibodies work. Pink blobs are denatured nuclei. Two in this slid, one being phagocytosed in the center by a PMN. This test is not nearly as sensitive as the ANA which has supplanted the LE cell test. Therefore, NEVER order an LE cell test. [Image contributed by Elizabeth Hammond, MD, University of Utah] Immunologic Findings Decrease in absolute number of T cells Accumulation of immune complexes with activation of complement lead to kidney damage. Drug induced lupus may occur, discontinue drug, symptoms usually disappear. Laboratory Diagnosis Screening test for anti-nuclear antibodies (ANA) first test done. Antibodies directed against nuclear material of cells. Flourescent anti-nuclear antibody (FANA) most widely used, extremely sensitive, low diagnostic specificity. Animal or human cells fixed to slide. Add patient serum and incubate. Wash to remove unreacted antibody. Add anti-human globulin labeled with fluorescent tag or enzyme. Antinuclear Antibody Test Antinuclear antibodies (ANA) are autoantibodies against various cell nucleus antigens and are found in patients with autoimmune diseases such as SLE. Some of ANA are considered to be useful for diagnosis of autoimmune diseases. This picture illustrates the most common antigens used in the ANA At the MLT level you will not be required to memorize. ANA Patients antinuclear antibody titer of 1:40 and characteristic multiorgan system involvement can be diagnosed with SLE without additional testing Patients with antibody titer of 1:40 who fail to meet full clinical criteria should undergo additional testing including: Tests for antibody to doublestranded DNA antigen Antibody to Sm nuclear antigen. Antinuclear antibody titer of less than 1:40 usually rules out systemic lupus erythematosus but patients with persistent, characteristic multisystem involvement may be evaluated for possible antinuclear antibody–negative disease. ANA Patterns of reactivity: Homogenous-entire nucleus stained Peripheral-rim of nucleus stained Speckled-spots of stain throughout nucleus Nucleolar-nucleolus only stained False positives and negatives occur. If positive, perform profile testing. ANA For the next exam you must be able to: Name the 4 primary reactions Describe the 4 primary reactions seen Identify the type of reaction in a photo Homogeneous Pattern Smooth, even staining of the nucleus with or without apparent masking of the nucleoli Nucleolar 23 or 46 (or some multiple of 46) bright speckles or ovoid granules spread over the nucleus of interphase cells Peripheral Fluorescence is most intense at the periphery of the nucleus with a large ring starting from the internal nuclear membrane and the rest of the nucleus showing weaker yet smooth staining. Speckled Large speckles covering the whole nucleoplasm, interconnected by a fine fluorescent network. Anti-nuclear antibodies detected by FANA Double-stranded DNA (ds-DNA) antibodies are most specific for SLE, correlate well with disease activity. Antihistone antibody second major antibody found in SLE. Deoxyribonucleoprotein (DNP) antibody, responsible for LE cell phenomena and available as a latex agglutination test. Anti-Sm antibody, specific for LE. SS-A/Ro and SS-B/La antibodies, most common in patients with cutaneous manifestations. Anti-nRNP detected in patients with SLE as well as mixed connective tissue disease. Presence of antibodies not diagnostic, may be present due to other diseases. Anti-Nuclear Antibody by Immunodiffusion Used to determine specificity. Ouchterlony double diffusion most frequently used to identify antibodies to: Sm, nRNP, SSA/Ro, SS-B/La and others. Test is not as sensitive but very specific. Systemic Lupus Erythematosus Extractable Nuclear Antigen Antibody to cytoplasmic and nuclear components. Over 100 different antigens described. It is associated with mixed connective disease and SLE with particular features (arthritis, myositis, Raynaud's phenomenon - also association with HLA-DR4 and HLA-DQw8). Extractable Nuclear Antigen ENA Antiphospholipid Antibodies Antiphospholipid antibodies may be present and are of two types. Anticardiolipin. Lupus anticoagulant, if present, may cause spontaneous abortion and increase Risk of clotting, platelet function may be affected. Treatment Aspirin and anti-inflammatories for fever and arthritis. Skin manifestations-anti-malarials or topical steroids. Systemic corticosteroids for acute fulminant lupus, lupus nephritis or central nervous system complications. Five year survival rate is 80 to 90%. Rheumatoid Arthritis Chronic systemic inflammatory disease primarily affecting the joints, but can affect heart, lung and blood vessels. Women three more times as likely as men to have it. Typically strikes at ages between 20 and 40, but can occur at any age. The three major symptoms of arthritis are joint pain, inflammation, and stiffness. Progress of disease varies. Arthritis Group of conditions involving damage to the joints of the body. Over 100 different forms of arthritis. Will discuss the autoimmune type, rheumatoid arthritis. Clinical Signs Diagnosis based on criteria established by American College of Rheumatologists, must have at least 4 of the following: Morning stiffness lasting 1 hour. Swelling of soft tissue around 3 or more joints. Swelling of hand/wrist joints. Symmetric arthritis. Subcutaneous nodules Positive test for rheumatoid factor. Xray evidence of joint erosion. Clinical Signs Symptoms initially non-specific: malaise, fever, weight loss, and transient joint pain. Morning stiffness and joint pain improve during the day. Symmetric joint pain: knees, hips, elbows, shoulders. Joint pain leads to muscle spasm, limits range of motion, results in deformity. Approximately 25% of patients have nodules over bones (necrotic areas), nodules can also be found in organs. Certain bacteria may trigger RA due to certain proteins that possess antigens similar to those antigens found in joint, ie, molecular mimicry Immunologic Findings Rheumatoid Factor (RF) is an IgM antibody directed against the Fc portion of the IgG molecule, it is an anti-antibody. Not specific for RA, found in other diseases. Immune complexes form and activate complement and the inflammatory response. Enzymatic destruction of cartilage is followed by abnormal growth of synovial cells, results in the formation of a pannus layer. Rheumatoid Arthritis Rheumatoid Arthritis Diagnosis Diagnosis is based on: Clinical findings. Radiographic findings Laboratory testing. Laboratory Testing Rheumatoid Factor IgM autoantibody directed against the Fc portion of the antibody molecule. Detected by testing patient serum with red blood cells or latex particles coated with IgG, agglutination is a positive result. Nephelometry and ELISA techniques are available to quantitate the RF. Erythrocyte Sedimentation Rate (ESR) used to monitor inflammation. C-Reactive protein (CRP) is utilized to monitor inflammation Treatment Goal to achieve lowest level of disease, remission if possible, minimization of joint damage. Rest and non-steroidal anti-inflammatory drugs control swelling and pain. Substantial functional loss seen in 50% of patients within 5 years. Slow acting anti-rheumatic drugs are coming into use but have side affects. Joint replacement. The End Write a question about anything you did not understand in this unit. You may choose to ask a question about any of the presentations required for viewing the next class period. WRITE YOUR ANSWERS TO THE 6 QUESTIONS presented in this presentation on a sheet of paper and submit when you walk in the door.