Principles of Palliative care Dr Ibrahim Bashaireh

Principles of Palliative care
Dr Ibrahim Bashaireh
Palliative derives from the Latin Pallium which means to cloak.
Palliation means to cloak over, to not address the underlying causes, but to eliminate the effects.
History of Palliative Care
4 th Century Christians
1842 Jeanne Garnier Lyon France
1879 Irish Sisters of Charity Dublin
1905 St Joseph’s London
1967 St Christopher’s London
Independent Sector
Marie Curie
Independent Hospices
Macmillan Cancer Relief
Public Sector
NHS Hospices
Palliative Care Beds
% Funding for Hospices
Palliative care
(WHO, 2003)
“ Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with lifethreatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychological and spiritual.”
Definition of Palliative Care (contd)
The goal of palliative care is achievement of the best possible quality of life for patients and their families
Affirms life and regards dying as a normal process
Provides relief from pain and other distressing symptoms
Integrates the psychological and spiritual aspects of patient care
Offers a support system to help patients live as actively as possible until death
To help the family cope during the patients illness and in their own bereavement
First of all
Family
Patient
You matter
Main aims
Improve the
Quality of Life
Avoid the avoidable suffering
Wellbeing
Promote comfort
Building Capacity : empowerment to adjust, relief and support the unavoidable suffering
Comprehensiv e Care
OMS 2002
Values
Respect their values
Active, alive conception
Patient and relatives
Integrity
Trust Honesty
Principles
•
We are focused on the patient and his/her family
•
We are Accessible
•
We are Collaborative
•
We provide high quality:
•
We are Safe and Effective
•
We are based on Evidence
•
We have resources
Ferris and Gómez- Batiste
10 instruments for palliative care
5.
6.
7.
8.
9.
1.
2.
3.
4.
10.
Needs assessment.
Systematic therapeutic Plan.
Symptom control.
Emotional support.
Information and communication.
Clinical ethics as the method for decisions
Change in the micro organization: the team work
Change in the organization of resources.
Evaluation and monitoring results quality and results.
Education, training, and research
And…..
Advance Care Planning and Case management and continuity of care
Physical
Spiritual
Symptom Bereavement
Control
Emotional
Psychosocial
General Palliative Care
Patients with less complexed needs
Nursing Homes, PC approach,
Specialist
Patients with complexed needs. Multiprofessional team with specialist PC training.
Medical, Nursing, Social Work, Spiritual,
Physio, OT, Pharmacy
Supportive
Provided from pre-diagnosis onwards.
Umbrella term for general & specialist services. Responsibility of all Health & Social care professionals
The Palliative Care Approach
NCPC (1997)
Vital and integral part of all clinical practice.
Informed by a knowledge of and practice of palliative care principals and supported by specialist palliative care
Quality of life
A whole person approach
Care for both the dying person and those that matter to the person
Patient autonomy and choice
Principles underlying palliative care provision
(NCPC 1997)
It is the right of every person with a life threatening illness to receive appropriate palliative care wherever they are.
It is the responsibility of every health care professional to practice the palliative care approach, and to call in specialist palliative care colleagues if the need arises, as an integral part of good clinical practice whatever the illness or stage.
What kind of issues would effect when or why people access palliative care services?
Consider:
Resources available
Regional differences
Education/information
History
When ?
Diagnosis
Active – Treatments
Death
Time
Palliative Care
56% wanted to die at home
25% of Cancer patients did
20% of people with other diseases did
11% wanted to die in hospital
47% of Cancer patients did
56% of people with other diseases did
24% wanted to die in a hospice.
17% of Cancer patients did
4% of people with other diseases did
National Council for Palliative Care 2003
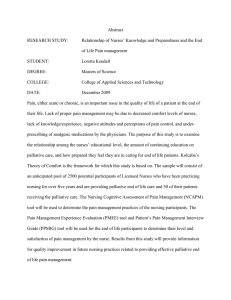
Frequency of common symptoms in advanced illness
(Atkinson & Virdee, 2001)
Symptom
Pain
Breathlessness
Vomiting or nausea
Sleeplessness
Confusion
Depression
Anorexia
Constipation
Pressure sores
Loss of bladder control
Loss of bowel control
Unpleasant smell
Patients with cancer
51
33
38
71
84
47
51
47
28
37
25
19
Patients with progressive nonmalignant disease
36
38
36
38
67
49
27
32
14
33
22
32
Palliative Care Nursing
Palliative care nursing
VALUING connecting empowering
Preserving integrity
Doing for
Finding meaning
Palliative care nursing
Connecting
Making a connection
– establishing a rapport
– building up trust
Maintaining a connection
– being available, spending time, sharing secrets, sharing self, maintaining trust.
Breaking the connection
– usually as a result of the patient’s death
Empowering.....
facilitating –
– recognises patient autonomy
encouraging
defusing
– dealing with negative feelings
mending
– - facilitating healing
giving information
Palliative care nursing
Doing for......
Taking charge
– symptom control
– making arrangements
Team playing
– acting as the patient’s advocate
Finding meaning
Focusing on living helping the patient to live as fully as possible
Acknowledging death
– giving or reiterating bad news
– talking about death and the time left
Preserving Integrity
Confronting own mortality
Burnout
Supporting
Colleagues
Hope
Comfort
Physical distress
Attachment
Physical Ease
Abandonment
& Isolation
Caring relationships
Worth
Feeling devalued Feeling valued
Hope nurturing interventions in palliative care
Comfort
Assessment, psychosocial issues.
Attachment
Be there, caring environment, promote communication
Worth
Explore previous experience, future wishes,enhance independence
The tyrannies of palliative care
(Aranda, 2001)
Niceness
Glowing testimonial
Depressing/Sad
Passive
Ethics
Treatment Options
Feeding/Fluids
Sedation
CPR
Carers
Euthanasia