GIRLS IMPACT ALIQUIPPA: A COMMUNITY HEALTH CAPACITY AND
NEEDS ASSESSMENT PROPOSAL
by
Lannea Artrice Adamson
BSW, Slippery Rock University, 2006
MSW, University of Pittsburgh, 2007
Submitted to the Graduate Faculty of
Behavior and Community Health Sciences
Graduate School of Public Health in partial fulfillment
of the requirements for the degree of
Master of Public Health
University of Pittsburgh
g
2013
UNIVERSITY OF PITTSBURGH
GRADUATE SCHOOL OF PUBLIC HEALTH
This essay is submitted
by
Lannea Artrice Adamson
on
July 29, 2013
and approved by
Essay Advisor:
Patricia I. Documét, MD, DrPH
______________________________________
Assistant Professor
Department of Behavioral and Community Health Sciences
Graduate School of Public Health
University of Pittsburgh
Essay Reader:
Valire Carr-Copeland, MSW, MPH, PhD
______________________________________
Associate Professor
School of Social Work and Graduate School of Public Health
Director, School of Social Work Ph.D. Program
University of Pittsburgh
Essay Reader:
Mary Hawk, DrPH, LSW
______________________________________
Visiting Assistant Professor
Department of Behavioral and Community Health Sciences
Associate Director, Institute for Evaluation Science in Community Health
University of Pittsburgh
ii
Copyright © by Lannea Artrice Adamson
2013
iii
Patricia I. Documét, MD, DrPH
GIRLS IMPACT ALIQUIPPA: A COMMUNITY HEALTH CAPACITY AND
NEEDS ASSESSMENT PROPOSAL
Lannea Artrice Adamson, MPH
University of Pittsburgh, 2013
ABSTRACT
Communities with low income families as well as communities of color experience a
disproportionate burden of morbidity and mortality. These health inequities are associated with
lack of access to community services, inadequate housing and low employment opportunities.
The public health significance that these inequities can have on adolescent females is that of
higher rates of dropping out of high school, use of drugs and teenage pregnancy. Aliquippa,
Pennsylvania is a city that may encompass the above disparities. This master’s essay describes a
detailed plan for a community health needs and capacity assessment for the city of Aliquippa to
help determine the health issues girls face and the city’s capacity to address their identified
health needs. I believe this is the first step in developing interventions and enhancing current
programs to address the needs of the adolescent girls in the community. The proposed
community-based participatory assessment includes engaging the community through
developing an advisory board, collecting existing data, conducting surveys and implementing
focus groups.
iv
TABLE OF CONTENTS
1.0 INTRODUCTION................................................................................................................... 1
2.0 BACKGROUND ..................................................................................................................... 4
2.1 HISTORY OF ALIQUIPPA .................................................................................................. 4
2.2 PUBLIC HEALTH SIGNIFICANCE OF TEEN PREGNANCY ...................................... 8
2.2.1
Consequences of Teenage Pregnancy ........................................................ 10
2.2.2
Risks Factors for Teenage Pregnancy ....................................................... 12
2.2.3
Conceptual Approaches.............................................................................. 14
2.2.4
Preventing Teenage Pregnancy ................................................................. 16
3.0 BACKGROUND ON COMMUNITY HEALTH ASSESSMENTS ................................. 21
3.1 NEEDS ASSESSMENTS...................................................................................................... 21
3.2 CAPACITY ASSESSMENTS .............................................................................................. 22
3.3 FORMATION OF ADVISORY BOARD ........................................................................... 23
4.0 COMMUNITY BASED PARTICIPATORY APPROACHES ........................................ 24
5.0 NEEDS AND CAPACITY ASSESSMENT PROPOSAL FOR ALIQUIPPA ................ 26
5.1 OBJECTIVES AND METHODS ........................................................................................ 26
5.2 COMMUNITY ENGAGEMENT ........................................................................................ 29
5.2.1
Relationship Building ................................................................................. 29
5.2.2
Formation of the Advisory Board ............................................................. 30
v
5.2.3
Windshield Tour ......................................................................................... 31
5.3 SECONDARY DATA COLLECTION ............................................................................... 32
5.4 PRIMARY DATA COLLECTION ..................................................................................... 33
5.4.1
Survey Service Providers ........................................................................... 33
5.4.2
Focus Groups ............................................................................................... 34
5.4.3
Community Surveys.................................................................................... 40
5.4.4
Core Group Discussion ............................................................................... 43
6.0
CHALLENGES OF PROPOSED COMMUNITY ASSESSMENT ...................... 44
7.0
CONCLUSION........................................................................................................... 45
BIBLIOGRAPHY ....................................................................................................................... 46
vi
LIST OF TABLES
Table 1. Median Household Income ……………………………………………………………7
Table 2. Comparison Data ……………………………………………………………………...7
Table 3. Methods for a proposed community health assessment for Aliquippa …………...28
Table 4. Focus Group Guide for Adult Women ……………………………………………..36
Table 5. Focus Group Guide for Adolescent Females ……………………………………….37
Table 6: Sample Survey for Girls ……………………………………………………………..42
vii
LIST OF FIGURES
Figure 1. Aliquippa Past and Present .........................................................................................5
viii
1.0 INTRODUCTION
Low-income communities and communities of color disproportionately experience the
burden of morbidity and mortality.[1] These health inequities are associated with numerous sociocultural, structural and physical environmental determinants of health status, such as poverty,
inadequate housing, racism, lack of access to community services, low employment
opportunities, air pollution, and exposure to toxic substances.[2] Aliquippa, Pennsylvania is a city
that encompasses the above disparities for reasons that I will explain below.
Aliquippa is a unique city and as such has unique challenges. However, its citizens have
unparalleled pride in their community. It is their relentless pride that is one of the city’s assets
and I sense that is why the heart of the city still beats. As I grew up in Aliquippa, it never seemed
strange to me that the local playground was called the “dump” or that as I walked home from the
bus stop I had to pass drug dealers that were not much older than I was. Although these
seemingly negative things were commonplace, it was also comforting to know that everyone
knew who I was. If they did not know who I was, they knew my brother, father or grandfather,
which meant people rarely bothered me. I lived down the street from grandparents, aunts, great
uncles and friends and I was at least the fifth descendant to live in this community. Like so many
other residents of Aliquippa, generations of extended families continue to dwell there.
One challenge that I observed growing up and that still has my attention as I work with
adolescent girls in the community has been the health issue of teenage pregnancy. It is also
1
evident that others in the community are starting to focus attention on teen pregnancy prevention
by starting groups for girls in the community such as “A Future Anticipated Cohort” for girls
which focuses on girl’s developmental assets and L.A.D.Y (Learning, Achieving, Developing,
You!) Rites of Passage Program for girls which focuses on life skills and etiquette training.
Because of the emergence of these new programs for girls and my own interest in
adolescent female health, I began wondering if teenage pregnancy is more of an issue in
Aliquippa than in other cities or if teenage pregnancy is even an issue at all. If it is a prevalent
health issue for girls in the city, my next question was, “does the city have the capacity to
address this health issue”? Furthermore, I have wondered what other health issues are prevalent
with adolescent girls such as whether or not smoking marijuana or dropping out of high school
before graduating are more of a problem. As I continued to work with others in the community to
support the needs of girls I realized I did not know the needs of this population.
A community health needs and capacity assessment can answer some of these lingering
questions. The overall objective of this essay is to explain in detail the importance of a
community health needs and capacity assessment and why it would be a valuable tool for the city
of Aliquippa. The proposed assessment will give details of an effective way to confirm the needs
of the adolescent girls in the city and also the city’s capacity to address their identified health
needs.
This essay will begin with the history of Aliquippa, Pennsylvania. The history will be
followed by a literature review of the public health significance of teenage pregnancy. A
background on community health assessments with an emphasis on community based
participatory approaches will follow and to conclude, a detailed plan of a proposed community
health needs and capacity assessment for Aliquippa is presented. The desired result of the
2
proposed assessment is to be able to provide the community of Aliquippa with information on
how to increase awareness of the health concerns of the adolescent girls and shed light on the
capacities that exist so that a plan can be devised to address these needs. The desired outcome is
to provide a plan to obtain a clearer picture of what the girls in the community need. Therefore, a
clear vision of the public health initiatives which should exist in the future is focused on the
evidence based needs of the girls in the community. The ultimate goal is to improve the health of
the adolescent girls in the community of Aliquippa.
3
2.0 BACKGROUND
2.1
HISTORY OF ALIQUIPPA
Aliquippa, Pennsylvania is the former home of the largest integrated steel mill in the
world, which stretched 7 miles along the Ohio River. Jones & Laughlin (J&L) Steel Company
bought the island in 1900. In 1908, businesses and homes were built to accommodate the influx
of new immigrant steel workers.[3] The borough was laid out in “plans” to separate people of
different racial and ethnic backgrounds. For example, Serbians, Croatians, Slavic, and African
Americans were separated to reduce language and social conflict.[3] Presently, people are no
longer separated by ethnicity; however different neighborhoods in the community are still called
plans. For example, Plan 11 is in the middle of a hill called Monaca Road and Plan 12 is
presently the neighborhood near the Aliquippa Junior and Senior High School.
In 1910, Aliquippa (what was then called Woodlawn) was considered the “jewel of
Pittsburgh-area communities” with its “hundreds of pretty homes, its clean paved streets, its
dozen of modern stores, churches, schools, lodges, clubs and ample transportation facilities”
according to an article in a Pittsburgh newspaper.[3] The article went on to discuss the school
systems as splendidly organized and its opportunities for delightful home and neighborhood life
were not equaled anywhere in this end of Pennsylvania.[3]
4
During the middle of World War II, when the demand for steel was the highest, J & L
Works employed an estimated 9,000 people and Aliquippa’s population was 27,000.[3] This
prosperity continued until 1984, the year I was born. The J&L closed most of the plant and 8,000
workers were laid off. It was the last and greatest big steel plant to fall in Pennsylvania. The once
bustling downtown of Aliquippa became a ghost town. In 1987, Aliquippa was finally
incorporated as a city but continued to plunge into depression and the federal government
declared it a distressed community that same year.[3]
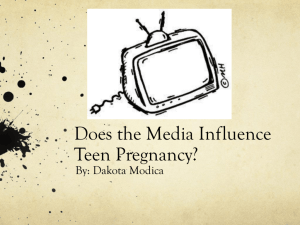
Figure 1. Aliquippa Past and Present
(The above figure shows downtown Aliquippa in the early 1900’s and currently)[3]
In 2011, the population of Aliquippa was estimated to be 9,422.[4] The African American
population was 39.8% compared to the African American populations of 3.9% and 2.7%
respectively in the neighboring townships of Center and Hopewell.[5] As stated previously, since
it is known that there is a disproportionate burden of morbidity and mortality that can exist in
communities with low economic and social resources and in communities of color, this fact may
leave the estimated 500 teens (age 15-19) vulnerable to the negative impacts of a financially
distressed region.[5]
5
Among the negative factors that can impact girls in particular are risky sexual behaviors,
dropping out of high school, engagement in criminal activity and teenage pregnancy. In 2010,
3.5% of girls age 15-19 were pregnant in Beaver County[6] compared to 2.7% in Pennsylvania[7]
and 3.4% nationally.[8] However, I suspect, because I grew up in the community and because of
my present work with girls age 14, that there may be a disparate amount of teenage pregnancy
among African American girls in Aliquippa. This has also been brought up as a past concern in
meetings with the principal and teachers at Aliquippa High School.
Table 1 and Table 2 represent data for Aliquippa and Pennsylvania. Table 1 displays that
the median household income in Aliquippa is almost $20,000 less than the entire state’s median
household income.[4] Table 2 shows the percentage of African American persons in Aliquippa is
far more at 38.6% than in Pennsylvania as a whole at 10.8%.[4] Furthermore, Table 2 also
displays that only 13% of persons from Aliquippa have obtained a Bachelor’s Degree compared
to 27% from Pennsylvania as a whole and 20% of Aliquippa’s people live below the poverty
level compared to 13% of people who live in Pennsylvania.[4]
6
Table 1. Median Household Income
$60,000
$50,000
$40,000
$30,000
Aliquippa
$20,000
Pennsylvania
$10,000
$0
Median Household
Income 2007-2011
Table 2. Comparison Data
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Aliquippa
Pennsylvania
White
Persons
Black
Persons
7
Bachelor’s Persons
Degree or
Below
Higher Poverty Level
2.2
PUBLIC HEALTH SIGNIFICANCE OF TEEN PREGNANCY
Pregnancy among adolescent females is not a new health issue, but it continues to be a
significant public health concern.[9-11] Despite substantial declines in recent years, nearly 800,000
adolescents in the United States become pregnant each year, which is unacceptably high.[12, 13]
The teenage pregnancy rate in the United States is the second highest among 46 industrialized
countries; only Russia has a higher rate.[14] More than 4 in 10 adolescent girls have been pregnant
at least once before 20 years of age and 82-90% of them describe their pregnancies as being
unintended.[15, 16]
After steadily rising in the late 1980s and peaking in 1991, childbearing rates in the
United States among teenagers fell steadily throughout the 1990s and early twenty-first
century”.[9, 17] By the year 2002, the overall teenage pregnancy rate declined from 111 per 1,000
in 1980 to 83.6 per 1,000 women aged 15–19, whereas the birthrate declined from 53.2 per 1,000
in 1980 to a record low of 41.7 per 1000 women aged 15–19 in 2003. [9] From 2007 to 2011, the
birth rate for females aged 15-19 years continued to decline by 25%, from 41.5 to 31.3 births per
1,000, the lowest rate ever recorded for the country.
girls age 15-19 in 2010 was 11,959.
[7]
[18]
In Pennsylvania, the number of births to
Of those births, 3,500 were born to non-Hispanic Black
teens which is a over-representation for this race. The birth rate to non-Hispanic Black girls 1519 was 56.2 per 1,000 compared to 18 per 1,000 for non-Hispanic whites. [7]
Despite declines across all ethnic and racial groups, epidemiological data continues to
document wide disparities in teenage birth rates by race and ethnicity.
[9, 18]
Young women from
all socio-economic and ethnic backgrounds face unintended pregnancies; however, poor youth
and youth of color are more likely to become adolescent parents.[9, 19] Although pregnancy rates
among Black teens decreased by 48% between 1990 and 2008, Black and Hispanic women have
8
the highest teen pregnancy rates (117 and 107 per 1,000 women aged 15–19, respectively).[15]
The majority of all births to non-Hispanic Black teen girls are to unmarried mothers. For
example, in 2010, 98% of births to non- Hispanic Black teen girls age 15-19 were to an
unmarried mother.[20] Finally, Black girls are approximately 1.7 times more likely to experience
an adolescent pregnancy than their White counterparts.[21]
Disparities also exist regarding risky sexual behaviors. In 2011, the rate of high school
students who have had sex are highest among non-Hispanic Black students (60%), followed by
Hispanic and non-Hispanic White students (49% and 44% respectively). [21, 22] Furthermore, the
percentage of non-Hispanic Black students who have ever had sex was significantly higher
among students in higher grades, ranging from 48% of 9th grade students to 74% of 12th grade
students.[22] Approximately two-fifths (41%) of non-Hispanic Black high school students
reported being sexually active —meaning, they had sex in the previous three months.[22] NonHispanic Black male students (21%) are significantly more likely than female students (7%) to
report having had sex by age 13. Finally, non-Hispanic Black students (25%) are more likely
than their Hispanic (15%) and non-Hispanic White peers (13%) to report that they have had four
or more sexual partners.[22]
For the past three decades, the prevalence of engaging in sexual behaviors contributing to
adolescent pregnancy and Sexually Transmitted Infections (STI’s) has been the highest among
Black youth compared with other ethnic groups.
[21]
Given these statistics, Black teens are the
group most vulnerable to the negative consequences of early sexual behavior.[21]
9
2.2.1 Consequences of Teenage Pregnancy
There are various consequences of adolescent pregnancies. Among these consequences
are those related to the health of the teen mother and child.[9] Pregnant teens younger than 17
years have a higher incidence of medical complications such as anemia, preeclampsia, and
premature delivery, although these risks may be greatest for the youngest teenagers.[16, 21] The
incidence of having a low birth weight infant (<2500 g) among adolescents is more than double
the rate for adults, and the death rate of a newborn baby (within 28 days of birth) is almost three
times higher.[16] Young adolescent mothers (14 years and younger) are more likely than other age
groups to give birth to underweight infants, and this is more pronounced in Black adolescents.[16]
Although it is low, the mortality rate for adolescent mothers is twice as high than for adult
pregnant women.[16] Adolescent pregnancy has been associated with other medical problems
including poor maternal weight gain, pregnancy-induced hypertension, and STI’s.[16]
Biological factors that have been associated consistently with negative pregnancy
outcomes are poor nutritional status and low pre-pregnancy weight and height.[16] Adolescents
also have high rates of STDs, substance use, and poor nutritional intake, all of which contribute
to the risk of delivering their baby preterm.[16] Many social factors have also been associated with
poor birth outcomes, including unmarried status, low educational levels, smoking, drug use,
inadequate prenatal care, and poverty.[16]
Poverty is not only a consequence of teenage pregnancy, but it predisposes teenagers to
become pregnant which seems like a never-ending cycle. Women who become mothers in
adolescence, along with their children, are far more likely to live in poverty than women who
postpone childbearing until their twenties. [7, 10, 21] Furthermore, fifty-six percent of teen births
occurred to young women who were poor, which is almost 10 times the rate of higher-income
10
adolescents.[19] This has an affect on their children as well. A child born to an unmarried
adolescent mother without a high school diploma is nine times more likely to live in poverty than
other children.[10]
Since lack of education is linked to poverty, the elevated rate of school dropout among
adolescent mothers remains at the forefront of concerns.[10] Across the nation, more than 60% of
adolescents who give birth before age 18 drop out of high school.[10] Only about 50% of teen
mothers receive a high school diploma by 22 years of age, versus over 90% of women who had
not given birth during adolescence.[15, 23] Fewer than 2% of teens who have a baby before age 18
attain a college degree by age 30 compared to teens who do not have a baby.[15] Not completing
high school or a GED by the age of 20 is a decisive indicator of future poverty.[10]
In addition to lower educational attainment,[9,
24]
adolescent childbearing is associated
with an array of other critical social concerns such as limited future employment opportunities,
welfare dependency, mental and physical health challenges, child health and well-being, child
abuse and neglect, separation from the child’s father, repeated pregnancy and criminal activity.[9,
16, 24]
These effects trickle down to the children of adolescent mothers. “The children of teenage
mothers are more likely to have lower school achievement and drop out of high school, have
more health problems, be incarcerated at some time during adolescence, give birth as a teenager,
and face unemployment as a young adult.”[23] These effects perpetuate a cycle of poverty and
teen pregnancy.
One of the most significant consequences of teen childbearing is financial. Teen
pregnancy accounts for nearly $11 billion per year in costs to U.S. taxpayers for increased health
care and foster care, increased incarceration rates among children of teen parents, and a loss of
tax revenue because of lower educational attainment and income among teen mothers.[23,
11
25]
Specifically, between 1991 and 2008 there have been approximately 268,930 teen births in
Pennsylvania, costing taxpayers a total of $10 billion over that period.[26] Teen childbearing in
Pennsylvania costs taxpayers at least $463 million in 2008. Of the total teen childbearing costs in
Pennsylvania in 2008, 28% were federal costs and 72% were state and local costs.[26] The
Department of Health and Human Services annual budget of approximately $33 million to fund
adolescent pregnancy prevention programs, and the presence of programs in 2,200 communities
provide evidence of ongoing concern.[10]
2.2.2 Risks Factors for Teenage Pregnancy
Given the cost to adolescents and their children, it is crucial to identify life experiences
and pathways for girls at increased risk for early sexual activity and adolescent pregnancy.[24]
Various studies have attributed many predictors that have an effect on early sexual intercourse
and teen pregnancy rates. Among the predictors are early pubertal development, early age at first
menarche, a history of sexual abuse, poverty, lack of attentive and nurturing parents, cultural and
family patterns of early sexual experience, lack of school or career goals, substance abuse, and
poor school performance or dropping out of school.[11, 16] Peer attitudes toward sexual activity
and sexually active friends have been associated with the initiation of sexual intercourse as
well.[11]
There are various other predictors for adolescent pregnancy. Some studies have indicated
early dating and having multiple sexual partners was linked to teen pregnancy.[11] Adolescents’
perceptions of their boyfriends’ level of desire for them to conceive may also be an important
predictor of pregnancy risk.[12] The concurrent use of alcohol, drugs, and risky sexual behaviors
has also been documented.[11,
12]
Finally, many studies have identified the absence of the
12
biological father from the home as a major risk factor for both early sexual activity and teenage
pregnancy.[24]
Family structural effect on teen pregnancy has been the focus of several studies. Families
with pregnant and parenting teenagers versus those with never-pregnant teenagers had lower
monitoring of their daughter’s activities.[27] Other studies have indicated the importance of
communication between parents and children for delaying sexual activity.[27] Being in a singleparent family or family of lower socioeconomic status and having a sister who had a teen
pregnancy has also been said to put teen girls at risk.[11] Milne et al.
[28]
posit that some young
women who are restricted in life choices (due to family circumstances, low income levels, low
educational levels, for example) may see early parenthood as something to aspire. Literature
supports pregnancy and childbirth as strategies used among certain subpopulations to find value
and purpose in an otherwise depressing or chaotic environments.[17]
A somewhat new factor that researchers are exploring as affecting teen pregnancy is
“ambivalence”. Recent research has documented the potential importance of ambivalent attitudes
towards pregnancy as predictors of pregnancy in adolescence.
[13, 29]
Some researchers have
suggested that adolescents may not be motivated to avoid pregnancy because they have
ambivalent feelings about, or feel positively towards becoming pregnant.[13] The majority of
female teens report that they would be very upset (58%) or a little upset (29%) if they got
pregnant, while the rest report that they would be a little or very pleased.[15] Although adolescent
pregnancies are largely unintended or unplanned, several studies have found that a significant
proportion (24%-64%) of adolescents feel some desire or ambivalence about becoming pregnant,
suggesting the importance of these feelings in understanding sexual risk behavior.[17]
13
Adolescents who expressed pregnancy desire or ambivalence were likely to be older, have been
younger at sexual debut, in shorter term relationships, and have greater perceived stress.[17]
2.2.3 Conceptual Approaches
Certain theories and models are consistent with the above research because they support
co-occurring behaviors and the affects life history has on behavior. The Problem Behavior
Theory posits that a syndrome of health-compromising and socially non-normative behaviors cooccur among some adolescents.[12] “Behaviors such as substance abuse, delinquency, and risky
sexual behavior have often characterized application of this theory.”[12] Life Course Adversity
Models of early sexual activity and teenage pregnancy posits that a life history of familial and
ecological stress—poverty, exposure to violence, inadequate parental guidance and supervision,
lack of educational and career opportunities—provokes earlier onset of sexual activity and
reproduction.[24]
The Theory of Reasoned Action, a social cognition model that provides a framework for
understanding an individual's voluntary behavior, supports the idea that an adolescent
engagement in consensual sexual behavior is, therefore, predicted by her intention to engage in
early sexual behavior.[21] An extensive review of programs to reduce teen pregnancy found that a
teen's beliefs about sex, and their values, attitudes, and intentions were the most important
factors related to sexual behavior.[21] Positive or permissive attitudes toward sex have been
directly linked to early sexual behavior with positive attitudes viewed as risk factors.[21]
Intervention efforts should target young women who desire or are ambivalent toward
pregnancy, such as those involved in new romantic relationships, and promote positive coping
skills to help reduce rates of adolescent pregnancy.28 Researchers go so far as to suggest that an
14
intervention designed to delay or prevent early sexual behavior should possibly begin by sixth
grade or age 10–11 years among African American girls.[21] Given the growing salience of
pregnancy desire in predicting risk, having an understanding of its correlates is important to
effectively target intervention efforts.[17]
There has been a previous focus on risk-taking behaviors that have often resulted in a
primary emphasis on measuring and preventing problem behaviors rather than on developing and
strengthening young people's assets.[9] Factors that are related to avoidance of early pregnancy
were older age at menarche, living with both parents in a stable family environment, regular
attendance at places of worship, higher family income, better problem-solving skills, more
educational aspirations, having an older sibling in the home and beginning to date at an older
age.[11, 16] Also, adolescents are less likely to engage in risk-taking behaviors if they have a sense
of physical, emotional, and economic security; are able to make a contribution to the community;
have input into decision making; and have opportunities to participate in engaging and
challenging activities that build skills and competencies.
[9, 10, 19]
Recently, parental supervision,
setting expectations, and parent/child “connectedness” have been recognized as clearly
associated with decreasing risky sexual behavior and other risky behaviors among
adolescents.[16]
Studies point to the significant role played by home, school and after-school
environments on adolescents' health-related decisions.[9] Thus, a key ingredient in reducing
adolescent pregnancy is providing youth with a supportive environment and a positive sense of
the future.[9] Therefore, even though the Theory of Reasoned Action provides support for
individual’s beliefs and attitudes towards sex in playing a significant role in sexual behavior this
15
theory is limited because it does not take into account the role one’s social surroundings have on
such behaviors.
2.2.4 Preventing Teenage Pregnancy
Government has influenced prevention efforts to reduce teenage pregnancy by
implementing policies that affect this population directly and indirectly.[9] Policy decisions have
had far-reaching consequences by simply increasing or reducing the resources available to
support programs and services.[9] Such decisions are laws and appropriations regarding the
availability of birth control and family planning services; policies on sex education in public
schools and government-funded media campaigns; programs to improve parent-child
communication; policies related to the availability of emergency contraception; laws that restrict
access to public funding of contraception; and the availability of abortion.[9] These efforts have
been effective in lowering teen pregnancy rates; however more specific prevention efforts need
to be geared toward minority populations.
While adolescent pregnancy prevention has emerged as a major health and social policy
issues, the difference in views about the root causes contributing to the high incidence of
adolescent pregnancy, as well as the conflicting social, religious, and ideological positions on
what to do about it, have resulted in an unwillingness to acknowledge that different segments of
the adolescent population most likely require different policy responses, rather than attempting a
one-size-fits-all approach.[9] Therefore, the challenge remains to consider a number of policy
options that respond not only to observable behaviors, such as adolescent childbearing, but also
to their underlying antecedents.[9] So, in order to effectively address teen pregnancy both
16
policymakers and others stakeholders need to recognize that the behavior of youth must be
altered, in concert with changing the attitudes and behaviors of peers and adults with whom they
have relationships.[9] Furthermore, a teen’s social and financial situation must also be taken into
account.
There are specific policies that have been put into place recently that have had a positive
effect on teenage pregnancy. In December 2009, Congress replaced the strict Community-Based
Abstinence Education Program with a new $114.5 million teen pregnancy prevention program to
support evidence-based interventions. Less than a year later, in March 2010, Congress created,
through health care reform, a five-year Personal Responsibility Education Program (PREP).[30]
The purpose of PREP is to educate adolescents on both abstinence and contraception and to
prepare them for adulthood by teaching them such subjects as healthy relationships, financial
literacy, parent-child communication and decision-making.[30] Also, through a provision in the
health care reform legislation, Congress renewed the Title V abstinence-only program for five
years.[30] This funding stream makes available $50 million annually for grants to states to
promote sexual abstinence outside of marriage without any other option for contraception.[30]
While a growing body of research clearly documents that teaching comprehensive
education pertaining to abstinence and contraceptive protection will not hasten the sexual debut
or increase the frequency or number of sexual partners, opponents continue to argue that
teaching abstinence-only is the sole means of reliably restricting young people from sexual
activity.[9] As of 2006, a number of reviews of abstinence programs found no scientific evidence
regarding its efficacy in delaying the initiation of sexual intercourse.[9,
30]
Moreover, research
shows that abstinence-only interventions may in fact deter sexually active teens from using
contraception which increases their risk of unintended pregnancy and STIs.[10, 30]Therefore, it is
17
suggested that successful sexuality education programs use a variety of teaching methods,
personalize the information about the risks of and avoidance of unprotected intercourse, and
provide opportunities to practice communication, negotiation, and refusal skills.[9]
It is not only up to educators and health professionals to have an impact on the
knowledge and views of teens regarding sexual activity and pregnancy. Parents and boyfriends
play an influential role in prevention of teen pregnancy as well. Crosby et al.[[12] state that
adolescent female’s perceptions of their partners’ desire for pregnancy may be an important
point at which to intervene. The authors also suggest that a component of behavioral intervention
programs be to recognize and challenge female adolescent’s perceptions of their boyfriends’
desire for pregnancy and provide females with the skills and resources required to effectively
prevent pregnancy despite potential lack of support or cooperation from their partner.[12]
Furthermore, parent-adolescent communication about sexual risks, maternal disapproval and the
quality of the relationship between the parent and adolescent can have an impact on the attitudes
of adolescents about sexual risk behavior and getting pregnant.[13,
31]
Therefore, pregnancy
prevention programs may need to extend their efforts to the parents and families of teen mothers
to help build their problem-solving and communication skills.[27]
Problem-solving and communication skills are needed in negotiating the use of
contraception. The majority of the decline in teen pregnancy rates in the United States (86%) is
due to teens’ improved contraceptive use; the rest is due to increased proportions of teens
choosing to delay sexual activity.[11, 15, 25, 30] In 2011, 65% of sexually active non-Hispanic black
students reported using a condom the last time they had sex, and 10% of sexually active nonHispanic black students reported using birth control pills.[22] A woman who is sexually active
and not using contraception has an 85% chance of becoming pregnant within a year.[15] Because
18
there is a high percentage of African American teens not using contraception, prevention efforts
need to assist in improving these rates.
Finally, social scientists have begun to examine the relationship between religious
commitment and adolescents’ views and behaviors regarding premarital intercourse or premarital
childbirth.[32] It has been shown that one of the most pervasive influences among AfricanAmericans is religion.[33] African-Americans are one of the most religious population subgroups
in the industrialized world.[33] It has also been suggested that this high level of religious
involvement is beneficial in that it may modify the negative consequences of stress and promote
psychological well-being. Therefore, it might be advantageous to encourage religious
involvement in pregnancy prevention programs regarding this population rather than
discouraging it.[32]
There are many influences and factors that affect pregnancy rates among African
American adolescents. Ongoing efforts to understand and target interventions to decrease
disparities in teen pregnancy are necessary.[34] The Social Ecological Model provides a useful
framework in order to understand the effects of multiple levels of influence such as individual,
dyad, family, peer/community, media, policy and other social systems on the behavior of
adolescents.[9,
35]
Rather than looking to correct deficiencies in adolescents themselves, this
model turns attention to creating healthy and supportive environments.[9] Such strategies to
create these environments could be individual health education, counseling, family education,
initiatives to strengthen educational and occupational opportunities, social marketing to foster
health peer and societal norms and policies and programs to address socioeconomic, racial and
ethnic health disparities.[28,
35]
Programs should also include abstinence promotion and
contraception information, contraceptive availability, sexuality education, school-completion
19
strategies, and job training.[16] Programs are needed that pay particular attention to adolescents
who are at highest risk of becoming pregnant and innovative programs that include males.[16]
Parents, schools, religious institutions, physicians, social and government agencies, and
adolescents all have important roles in successful prevention programs.[16]
20
3.0 BACKGROUND ON COMMUNITY HEALTH ASSESSMENTS
Many health promotion programs fail to reach their goals because they are built upon
invalid assumptions about what people need, want and will do about it.[36] Therefore, in order to
develop, implement, and evaluate health education strategies for health promotional purposes,
needs and capacity assessments have to be a part of the process early on.[36] I will define needs
and capacity assessments in detail and describe a community based participatory approach to
assessments and why it is imperative that such assessments are done in the community of
Aliquippa in order to implement effective health programs for African American girls.
3.1 NEEDS ASSESSMENTS
“A need is the difference between the present situation and a more desirable one.”[36] A
needs assessment is a planned process that identifies the needs of an individual or a group.
Existing data is collected and people are equally important sources of information. Individuals in
the community draw upon their experiences, observations, ideas, opinions, and feelings to guide
them toward conclusions about their needs.
Needs assessments are conducted to provide a starting point before program development
is initiated. Instead of basing the development of a proposed program on the perceptions of
21
outsider’s research of the community, a participatory assessment gets the target population
involved in purposeful activities to be a part of the process.
[37]
The goals of a community
assessment are to: (1) examine data from existing sources; (2) gain clarity on the problem and
study it in greater detail; (3) identify the structural, social, cultural, and other resources that can
be utilized; and (4) identify a direction for action and expand partners and stakeholders who can
help address the problem.[38]
3.2 CAPACITY ASSESSMENTS
Capacity on the other hand, refers to both individual and collective resources that can be
brought to bear on health enhancement. It can provide certain protective influences that affect
whether people engage in certain risk-related behaviors.[36] At the group level, capacity can be
considered as unique histories, cultures, structures, personalities, politics, and systems that come
together to enhance health.[36]
A capacity assessment is a measure of actual or potential individual, group, and
community resources that can be utilized for health maintenance and improvement.[36] Capacity
assessments are conducted to provide an opportunity to engage multiple stakeholders such as
community organizations, churches and others in a review of actual and potential resources that
can influence current and future partnership efforts.[36] It is informs what resources can be used
to address the problems that exist. Together, needs and capacity assessments go hand in hand in
the program planning process.[37]
22
3.3
FORMATION OF ADVISORY BOARD
There are two types of groups involved in community assessments. One group is
comprised of professionals that are directly involved in the planning, coordinating or facilitating
of the assessments. They bring to the process health-related expertise, and often previous
experience in community assessments. The second group consists of the target audience (and
those that support them), which contributes in identifying a range of needs, wants, interests, and
capacities. The latter should be engaged from the outset so that their contributions can be made
during the planning, implementations, and evaluation phases, as appropriate.[36]
The two groups made up of both the practitioners and stakeholders (i.e. those involved in
and affected by the issues being addressed) make up the planning and advisory board. This
committee can help to plan and conduct the assessments.[36] The committee can determine which
kinds of needs and resources to consider, from whom to gather information, and which strategies
to use. They can also assist with data collection and analysis. They will ensure that the program
is based on culturally appropriate needs and the available and potential resources of the intended
participants.[36] Additional insights can be gained from contact with key informants who are able
to express their perceptions of the needs of others. These individuals can include community
leaders, health and human service professionals, leaders of religious organizations, public
officials, educators and the like. Many times these key informants help to frame key areas of
needs which are then followed up by more definitive needs assessment strategies.[36] There
should be consensus among the stakeholder group and the advisory group is committed to this
shared goal.
23
4.0 COMMUNITY BASED PARTICIPATORY APPROACHES
An essential part of community-based assessment activity is to work in partnership with
the community, rather than viewing it as a setting in which professionals conduct investigations
known only to them.[36] This awareness by health and human service professionals and
community members has led to the emergence of community-based participatory approaches
where in community members become involved in the essential phases of project planning,
implementation, and evaluation.
Community Based Participatory Research (CBPR) in public health is a partnership
approach to research that equally involves, for example, community members, organizational
representatives, and researchers in all aspects of the research process. All partners contribute
their expertise and share decision making and ownership.[1] The principles of CBPR can also
apply to evaluations or assessments.
Even though there is not one “best” set of principles for CBPR, there are a set of
principles that are suggested as a goal to strive for:
1.) CBPR acknowledges community as a unit of identity (for example, social
networks or geographical neighborhood)
2.) CBPR builds on the strengths and resources that are within the community
3.) CBPR shares decision-making and control regarding collection, interpretation and
dissemination of data while developing relationships based on trust and mutual respect
24
4.) CBPR fosters co-learning and capacity building among all partners by
acknowledging that everyone brings diverse skills, expertise and experiences
5.) CBPR integrates and achieves a balance between both science and knowledge to help
the community
6.) CBPR focuses on the local significance of public health problems and on
ecological perspectives that attend to the multiple determinants of health
7.) It involves developing systems using a cyclical and iterative process
8.) CBPR disseminates results to all partners and involves them in the wider
circulation of results in ways that are understandable, respectful and useful
9.) CBPR involves a long-term process and commitment to sustainability.[1]
Participatory Community Assessments (PCA) are a collective approach to assessing how
a community is defined and organized and assessing who is best to discuss a joint effort with.
Also, PCA assesses what issues and needs exist from a community perspective and what
structural and other factors explain them. Furthermore, it assesses what resources and assets are
available that residents could mobilize to resolve a community problem and what changes might
take place that could address existing disparities in new and transformative ways.[38] A good
PCA involves a partnership between community members (most often a coalition or advisory
board) and academically trained researchers to accomplish a shared practical goal – the
collection of information that leads to community improvement and transformation. [37]
25
5.0 NEEDS AND CAPACITY ASSESSMENT PROPOSAL FOR ALIQUIPPA
5.1
OBJECTIVES AND METHODS
The objective of this proposed assessment is to provide the community of Aliquippa with
a plan to identify the needs of the African American, adolescent girls in Aliquippa and also
develop the community’s capacities and abilities to effectively address these health needs. More
specifically, the proposed assessment will focus on answering the question of whether or not
teenage pregnancy is a health issue and will serve to identify other issues that may be
problematic regarding this population. There are many interventions already in place and
opinions and ideas circulating about the best way to improve the health of young women; but
how many of these ideas will actually work in the city of Aliquippa? It should not be assumed
that just because an intervention has worked in a similar community (even in Pennsylvania or the
surrounding counties) that these same interventions will work for the adolescent girls in
Aliquippa. Aliquippa is a unique city and as such the people have unique skills, challenges and
issues.
Engaging the community and carrying out an assessment will foster an environment
where members of the community can get involved in the process of making things better for
young women in their community. A thorough health needs and capacity assessment can prevent
lack of awareness of the health issues most pressing in the lives of these girls and subsequently
26
will provide a place to start when developing interventions. The individuals who live in
Aliquippa can become truly empowered if they have the knowledge required to assess their
situation.[39] Not only that, but the assessment can foster ownership of the results and lead to
action.
Because I would like to engage a broad spectrum of people in the community for the
assessment, I believe that it is appropriate to use an approach called Locality Development. This
approach is characterized by community participation, increased awareness, community capacity
building, problem-solving and empowerment.[40] As opposed to social action and social planning
approaches, Locality Development involves a broad cross section of people in determining and
solving their own problems and seeks to build the communities capacities to make collaborative
and informed decisions.[40] Leadership is drawn from within and direction and control are in the
hands of local people.[41]
The proposed assessment will be implemented in several phases. Table 3. displays the
proposed methods that can be used in each phase and what specific information/advantage each
method will provide. The below is a plan, but it may be modified with community input. These
methods will be described in detail.
27
Table 3. Methods for a proposed community health assessment for Aliquippa
Phase II
Phase I
Methods
Relationship
Building
To engage the community and elicit their help with
the assessment
Advisory
Board
Formation
To collaborate with members of the community so
that the assessment is a joint effort
Windshield
Tour
To experience the community on the ground level,
cement relationships and draft a list of resources
available
Secondary
Data
Collection
To gather demographical and descriptive data on the
city and its people
Survey
Service
Providers
Phase
III
Objectives
To gauge the city’s current capacity to address the
health issues of girls in the community which helps to
compile the list of resources.
To obtain information on what the service providers
deem as important issues to address with adolescent
girls
Focus
Groups
To elicit opinions and suggestions from women in the
community regarding their main concerns for girls in
Aliquippa
Survey Girls
To collect information on the health behaviors of
girls in the community from their point of view.
28
5.2
COMMUNITY ENGAGEMENT
5.2.1 Relationship Building
Engaging the community will give me a chance to solidify existing and new relationships
with stakeholders in the community who have an interest in the health and well-being of girls.
By building upon these relationships, developing an advisory board and getting to know the
community on the ground level through windshield tours it will allow me to lay the groundwork
to collaborate with the community in this endeavor. This is an important phase because without
community involvement the assessment may not be accurate or successful.
Because I was raised in Aliquippa and still work in the city I will have an advantage over
someone who may have an initial barrier in building relationships if they are an “outsider” to the
community. It will not be difficult for me to build relationships in the community because I can
build off of existing relationships that have already been developed over years of living and
working there. However, this can also be a limitation because even though I can quickly
establish rapport, they might want to please me and report false information.
People that I will reach out to in the community are: the mayor of Aliquippa; directors of
local non-profit organizations such as the Council of Young Men and Fathers and Aliquippa
Impact, Inc.; directors of community centers such as the Tyler Community Youth Center and
Linmar Community Center; church leaders from local churches such as Triedstone Baptist
Church, Sound the Alarm Ministries and Crestmont Alliance Church; the principal, vice
principal and teachers at the Aliquippa Junior and Senior High School; and other family
members and friends. I will also attend community meetings that already occur regularly at the
B. F. Jones Library and Uncommon Grounds Cafe (especially those that are focused on
29
adolescents). Finally, and most importantly I will reach out to African American girls in the
community since they are the focus of the assessment.
5.2.2 Formation of the Advisory Board
These new and existing relationships that will be developed lay the ground work to form
an advisory board. This core group composed of people and girls from the community will help
me in facilitating the assessment process. This core group’s role is to help plan, coordinate and
evaluate responsibilities throughout the whole process of the assessment.[40] This group will help
me keep the needs assessment on task. The goal is to empower community members, leaders and
stakeholders to assist me in developing and implementing the assessment. However, I will be
doing the majority of the work. Along with the above, my role is to introduce the assessment,
train and provide updates to the broader community by sending emails and letters to
organizations, churches and leaders to introduce the advisory board, the reason for our presence,
and explain the assessment purpose in order to prime the community for future participation.
The advisory board will be made up of approximately 7-12 members and leaders from the
community. The goal is for the members of the advisory board to be comprised of the new and
existing relationships that I have already developed in the community. It is desirable to have a
diverse group of people e.g. a pastor, a teacher, a business owner, an organization leader, a
parent and other community members, so that different experiences and capacities of the
individuals can be brought to the table. I will seek members that are adolescent girls or that have
shown interest in adolescent girls either by profession or volunteerism so that hopefully they are
more likely to join the advisory board and stay engaged.
30
The board will meet once a month in a community setting such as the Linmar
Community Center or Uncommon Grounds Cafe so that everyone is on the same page and so
that the assessment stays on track. Everyone will have decision making power and we will use a
majority vote to make decisions. A convenient time and day will be selected to meet to
accommodate everyone’s schedule and the meetings will last approximately one hour and a half.
A challenge that may arise while working with the advisory board is to maintain interest
and attendance among the members. Also, since the members will have different opinions and
agendas it may be challenging to make sure that there are no arguments or fights. Since the
advisory board’s role in the assessment is extensive, it is important for me to find ways in which
to empower and show appreciation for all of their work either by compensating them and/or
presenting them with a certificate of recognition.[42]
5.2.3 Windshield Tour
The next phase will be to get to know the community on the ground level. Even though I
was born and raised in Aliquippa, that does not mean I know everything about the city. I will
plan to engage in windshield/walking tours to gain an impression of daily community life and a
feel for Aliquippa. This is something that the advisory board and other community partners can
do with me. They can also be a valuable resource because they live in the city and can give me
insight and information on the composition of different neighborhoods. Furthermore, I can learn
a great amount of valuable information from getting out of my car and walking and noticing how
many dilapidated buildings there are, how many places are available for kids to go, how many
businesses are running, whether there are sidewalks to walk on and whether people drive, ride
31
the bus or catch “jitneys” (informal taxis). Also, this will give me a chance to make a list of the
assets that I see in the community such as the number of churches, community centers, and
businesses that are supporting the community as a whole. While I am walking around I can also
get a chance to talk to local people and get their opinions about their community. I will also
concentrate on getting the opinions of teenagers in the community. I will write a short internal
report for the advisory board about the information obtained to elicit further feedback and to
keep them informed.[42]
5.3
SECONDARY DATA COLLECTION
The following phase will be for me as the primary researcher to collect secondary
quantitative data regarding adolescent girls in Aliquippa. The racial makeup and socioeconomic
status of Aliquippa is quite different from the surrounding communities. Therefore, information
will be collected for the county, but as much as possible information will be collected for solely
Aliquippa. Demographic factors such as race, socioeconomic status, average household size and
income, and the like will help me anticipate the issues the girls in the community may face. The
information collected such as the local health indicators regarding adolescent girls will be
compared to state and national statistics as well as data from local counties to compare and get a
clear picture of the community. Data will be collected from the following sources:
Pennsylvania Department of Health: This source will provide me with data regarding
state and county health statistics such as birth and death records, incidence of teen
pregnancy and burden of specific diseases.
32
Census Bureau: This source will provide rates regarding population, education, income,
etc. on the state of Pennsylvania, Beaver County and specifically, Aliquippa.
Pennsylvania Department of Health – Beaver County Office: This source will add to the
health information specific to Beaver County and the city of Aliquippa such as
immunization records and birth and death certificates.
Aliquippa High School: The school can provide information regarding number of
pregnancies, school attendance, graduation rates, and number of suspensions for fighting
and other bad behavior.
Centers for Disease Control and Prevention (CDC): I can obtain a plethora of facts and
information regarding adolescent health and other relevant public health data for the U.S.
from the CDC website. Also, I can use the information gathered to compare and put into
context the information obtained from Aliquippa.
5.4
PRIMARY DATA COLLECTION
The next phase is to collect primary data. The goal will be to collect data from people in
the community through focus groups, questionnaires and surveys.
5.4.1 Survey Service Providers
I first will survey individuals and organizations that are already providing services to
girls age 13-18 in the community. The services that these organizations provide can be specific
33
to girls and that apply to their age group in general. A list of individuals to contact will be
gathered while engaging the community, from people I already know in the community and
through referrals from the advisory group. The objective in surveying them first will be to
identify services that each individual or organization provides in order to review the
community’s current capacities regarding this population. By gathering this information, I can
then complete the list of existing available resources that these individuals or organizations
provide. Also, I will look on the city’s website and the community boards in the B. F. Jones
Library and local coffee shops such as Uncommon Grounds Café and Mac’s Donuts.
To survey the individuals, I will send electronic surveys through the internet since most
people and organizations have email. The pros in using the internet is that it requires less time
and resources, however, the con is that it may result in a lower response rate and it also can not
reach those who do not use social media.[43] To alleviate this, I will suggest sending weekly
reminders for the duration of a month to remind the individuals to complete the survey.
Examples of questions I will put in the survey are, “What specific services do you provide to
girls age 13 to 18 in Aliquippa?” or “How many girls do you provide services to on average each
week?” Furthermore, I will ask questions in reference to what I have researched in the literature.
5.4.2 Focus Groups
After gaining a grasp on the capacities that the above individuals and organizations bring
to bear I will conduct focus groups with the help of the advisory board. The objectives of the
focus groups are to elicit the opinions and suggestions of the women in the community regarding
adolescent girls and specifically to learn their main health concerns particularly regarding
teenage pregnancy. I want to know if they feel the current services that are in the community are
34
effective, their feelings about the neighborhood as a whole and the health behaviors that put them
at risk. I also want to know if they think teen pregnancy is an issue in their community.
Furthermore, I want to find out if what the community deems as relevant health issues lines up
with what the data obtained from secondary data collection displays. I am solely focusing on
women because I believe that they will have more opinions to bring to bear because they have
experienced it themselves.
The first step before conducting focus groups is to define the population which will help
determine the questions I ask. The Life Course Adversity model will also inform how and what
questions are asked. Second, the advisory board and I will develop an interview guide.[36] The
focus group guides for each group will be very similar; however the wording will be different to
take into account participants for the separate groups. Table 4 and Table 5 display examples of
appropriate focus group guides for adult women and young women respectively. We will recruit
participants through word of mouth, emails to organizations and leaders, and flyers in
community settings and schools. The flyers will state the date and time of the focus groups and
why they are being conducted.
35
Table 4: Focus group guide draft for the adult women focus group
Adult Women Focus Group Guide Draft
Introduction: Introduce moderator, co-facilitator, and anyone present from the advisory board. Then
everyone else can introduce themselves/the aliases they have chosen. Establish rules, location of
bathroom, etc.
Purpose: The purpose is to elicit women’s opinions on the subject of adolescent female health in
Aliquippa. The focus group will be audio recorded. All discussions, names and audio-recordings will be
kept confidential
Questions:
1. Let’s think back to when you were in high school. What do you remember?
PROBE: What were the main issues girls faced?
2. Now come to the present. Tell me what you think the main issues are for teenage girls in Aliquippa
today?
3. What kind of support do girls have regarding these issues?
PROBES: counseling, places to seek refuge, medical facilities…
4. Do you think that teenage pregnancy is an issue?
5. How can teenage pregnancy be prevented?
PROBES: communication, role models, school support, parents
6. What types of supports did you have or would have liked to have had as a teenager?
7. What types of community programs currently exist as a distraction from risky behaviors?
8. Any last comments/remarks?
Closing: Thank you for participating
36
Table 5: Focus group draft of questions for the adolescent girls
Adolescent Girls Focus Group Guide Draft
Introduction: Introduce moderator, co-facilitator, and anyone present from the advisory board. Then
everyone else can introduce themselves/the aliases they have chosen.
Purpose: To learn girl’s opinions on the subject of adolescent female health in Aliquippa
Questions:
1. Tell me about your favorite activity to do during this time of year?
PROBE: ride your bike, take a walk, eat at barbeques
2. What do you like about living in Aliquippa?
PROBE: What don’t you like?
3. What are the positives about your community?
PROBE: What are the challenges?
4. What are some issues that you think girls in Aliquippa deal with?
5. What kind of support do girls have regarding these issues?
PROBE: What places can girls go to get help?
6. What are some things that you would like to see in Aliquippa for girls to do?
PROBE: camps, community center activities
7. What do you think that girls need that will help them?
8. Any last comments or remarks?
Closing: Thank you for your help.
37
The next step is to enlist a well trained, experienced moderator that is similar to the
participants in the groups.[36] They should be experienced in moderating groups and be familiar
with the research and assessment purpose.[36] The moderator will use the focus group guide to
direct the discussion. The guide is important so that all topics are discussed, however new topics
may emerge depending on the conversation that develops amongst the participants and these
topics will be pursued. It is important to let the group take more of a lead in discussing the
questions that are asked by the moderator.[36]
After securing a relaxed and informal setting to have the focus groups in the community,
such as the Linmar Community Center, the next step is to conduct the focus group. The
participants will be given time at the beginning to get to know each other.[36] After this period,
the conversation can start with introductions. The moderator will be the first to introduce herself.
All participants of the focus groups will then be given information regarding why the focus
groups are being conducted, the main discussion topic(s) (e.g. to discuss the health of young
women in Aliquippa) and to get their permission to audio record them. Because real names
should not be used during the group, participants will be called on by an alias that they choose.
They can put the names they choose on name tents to be placed in front of them and that is how
they will be identified. However, this may be limitation since the participants may know each
other. In that case, I would ask them to sign a confidentiality agreement. A clear explanation of
the participation guidelines: such as speak one at a time and be honest with what you think and
feel should also be given.[36]
After the initial introductions are completed, the moderator will begin posing questions
about the topic and guiding the discussion with the help of the focus group guide. The discussion
will be continued on each topic until no further ideas are generated.[36] There may be an issue in
38
getting the true opinions of the participants particularly with the girls because they may simply
follow their social leaders. I along with the moderator will address this by reminding the
participants through out the group that their individual opnions are important. The groups will
last one hour to an hour and a half and near the conclusion of the groups each participant can be
asked to give one final comment. The moderator will then summarize the key issues raised and
end the meeting.
All sessions will be audio recorded to capture everything that is said. Since it will be
difficult for the moderator to run the group and take notes at the same time, a co-facilitator will
take notes during the focus group to capture body language and other details that may be missed
on the recording.[36, 43] If it is possible, the participants should be given a monetary compensation
for their time, such as gift cards to local businesses.[36]
The goal is to conduct four focus groups: two with adolescent girls, two with women, so
that we can obtain both viewpoints on the same topic. The target will be to have 6-12 members
(ideally 8) in each focus group and participants should be homogeneous.[36] Saturday during the
afternoon is a good time and day to have the focus groups as most people are not working and
are available to participate. For example, there may be better attendance to the group on a
Saturday than there would be on a Wednesday. Finally, we will provide lunch as another
incentive to participate.
While the focus groups are being conducted, I will transcribe the recordings of the groups
for qualitative analysis.[43] I, along with one or two members of the advisory group, will analyze
the transcripts by looking for similar themes. I will train them on how to recognize themes and
together we will look for repeated ideas from several participants that have to do with the health
of young women in Aliquippa. For instance, if several participants state (even in different ways)
39
that girls in Aliquippa usually date older boys, this is a relevant theme that has emerged from the
group discussion. The themes will then be categorized and grouped together (coded) so that
similar topics and suggestions can be highlighted. I expect to find themes related to teen
pregnancy and/or dropping out of high school, however other topics may emerge. Furthermore, I
will analyze and interpret the data with both pen and paper or with the aid of qualitative data
software called Atlas. ti.[37] I will produce an internal report of the information gathered for the
advisory board.
5.4.3 Surveys with Adolescent Girls
After we conduct and analyze the focus groups, the core group and I will develop a
questionnaire to survey girls in the community. The objective in surveying girls in addition to the
focus groups is to collect self-reported information on the health behaviors of girls in the
community. The survey will need to be pilot tested to make sure the wording is clearly
understood by the participants filling out the survey. The questions will be tested out on a group
of five girls so that suggestions and improvements to the questions can be made.[37] After taking
the recommendations into account and implementing suggested revisions we will develop a final
survey. The core group will then need to decide how and where the surveys will be implemented.
Since we want to survey the target population of adolescent girls in Aliquippa it will be
important to have a sampling strategy. I will get a list of girls from Aliquippa Junior and Senior
High School and attempt to survey as many girls as possible of the approximate 150 girls in the
school. I will stratify the list of girls by grade and attempt to survey an equal amount of girls
from each grade. The surveys will be self-administered during a free period during school hours
with the assistance of someone from the advisory board who has been trained to implement the
40
survey. Furthermore, it may also be convenient (especially for the youth) to look into having
participants complete surveys on hand-held devices. This can be costly, however it may yield a
better response rate from the girls since most of them are probably used to using technology.[36]
The confidentiality of the girls would be protected by not asking them to put their name or any
other identifiers on the survey.
Below in Figure 4 is an example of some of the questions that will be used for the survey.
The questions will focus on topics such as sex initiation, fights, dating violence, etc. A majority
of the survey questions have been tested, proven effective and are used by the Centers for
Disease Control and Prevention for their Youth Risk Behavior Survey.[44] In a final version of a
survey I would intersperse more “soft” questions throughout the more threatening questions. An
example of a soft question is, “Do you like your school?’ An example of a more threatening
question is, “During the past 12 months, how many times were you in a physical fight?”
The information that I expect to get from the surveys is information on the health
behaviors of the girls in Aliquippa. The sample questions can adequately elicit that information.
Frequencies of the survey responses will be calculated with the use of a quantitative data tool
such as SPSS. I will describe the data collected in a report that will be shared with members of
the advisory board and the broader community.
41
Table 6: Sample Survey for girls [44]
Sample Survey Questions
This survey is about health behavior. It has been developed so you can tell us what you do that may affect your
health. The information you give will be used to improve health education for girls like yourself.
All information you give will be kept confidential
DO NOT write your name on this survey. The answers you give will be kept private. No one will know what you
write. Answer the questions based on what you really do.
Thank you very much for your help
1. How old are you?
A. 12 years old or younger
D. 15 years old
G. 18 years old or older
2. In what grade are you?
A. 9th grade
D. 12th grade
B. 13 years old
E. 16 years old
C. 14 years old
F. 17 years old
B. 10th grade
C. 11th grade
E. Ungraded or other grade
3. What is your race? (Select one or more responses.)
A. American Indian or Alaska Native
B. Asian
C. Black or African American
D. Native Hawaiian or Other Pacific Islander
E. White
4. Do you like your school?
A. Yes
B. No
5. I am liked by my classmates.
A. Strongly Agree
B. Agree
C. Disagree
D. Strongly Disagree
6. During the past 12 months, how many times were you in a physical fight?
A. 0 times
B. 1 time
C. 2 or 3 times
E. 6 or 7 times
F. 8 or 9 times G. 10 or 11 times
7. Would you consider yourself a happy person?
A. Strongly Agree
B. Agree
C. Disagree
D. 4 or 5 times
H. 12 or more times
D. Strongly Disagree
8. During the past 12 months, did you ever feel so sad or hopeless almost every day for two weeks or more in a row
that you stopped doing some usual activities?
A. Yes
B. No
9. During your life, how many times have you used marijuana?
A. 0 times
B. 1 or 2 times
C. 3 to 9 times
E. 20 to 39 times F. 40 to 99 times
G. 100 or more times
D. 10 to 19 times
10. Have you ever been on a date?
A. Yes
B. No
11. Have you ever had sexual intercourse?
A. Yes
B. No
This is the end of the survey. Thank you very much for your help.
42
5.4.4 Core Group Discussion
After both the completion of surveys and the implementation of focus groups, the core
group will reconvene to analyze and organize the data that has been collected. With the reports
that I have already given the board, we will determine if there is any difference between
secondary data collected about the adolescent females in Aliquippa and the girl’s responses
concerning their health and what they want and need to know. Also, we will organize the themes,
opinions and suggestions that have been collected from the community.
Finally, a community health assessment report will be generated with the support of
volunteers from the core group. We will invite the girls back that participated in the assessment
in order to share the results of the assessment with them and get their opinions on whether they
agree with the findings. It may even be appropriate to present the report to the community in a
public meeting.[36] We will hopefully give the community of Aliquippa a great insight into where
program efforts for girls should be focused and what the true needs of this community are and
how to take action to address them. Organizations and leaders that are already working with the
girls in the community will have a broader knowledge of the health issues that girls face and if
teenage pregnancy is one of them. The entire process of the assessment can last anywhere from 6
months to two years. It all depends on how engaged the community is and how helpful the
volunteers and the advisory board is. It is my guess that teen pregnancy will emerge as an issue,
however we will be open to if teen pregnancy does not emerge as the main issue.
43
6.0 CHALLENGES OF PROPOSED COMMUNITY ASSESSMENT
One challenge in implementing a community assessment may be to get and keep interest
from the community. However, this may not be an issue due to the fact that I already have made
connections and relationships with people in the community and will plan to cultivate those
relationships during the assessment. It is my expectation that there will already be a level of trust
between me and the community and my intentions in doing the community assessment.
Conducting community health assessments can be a strenuous task; however because I
will be eliciting a lot of help from the community it may not be as laborious. Furthermore, the
outcomes of such a task are well worth the effort especially if the community builds ownership
of the project. Having a firm foundation for which programs can be built on is an invaluable gift
to a community.
44
7.0 CONCLUSION
The proposed community health capacity and needs assessment for the city of Aliquippa
stemmed out of my desire to help the community address the needs of the young women who
live there. Not only do I want to support interventions and programs that have been proven to
work, but I want to make sure that energy is placed where it needs to be, which is on the true
health needs of the girls.
A more desirable outcome would be that because of the proposed assessment steps will
be taken to actually implement it. If it was implemented I will consider the assessment successful
even if the community adopts no change, because at the least, through the process of doing the
assessment they will be more educated and aware of the personal and social issues the young
women in their community face. It is my desire that current and future interventions aimed at
adolescent female health will actually address the accurate needs of the community of Aliquippa
and will be based on evidence and not just educated guesses of what girls need.
45
BIBLIOGRAPHY
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Israel, B.A., et al., Introduction to Methods for CBPR for Health, in Methods for
Community-Based Participatory Research for Health, B.A. Israel, et al., Editors. 2013,
Jossey-Bass: San Francisco, CA 94104-4594. p. 6, 8-11, 14.
Braveman, P.A., et al., Socioeconomic Disparities in Health in the United States: What
the Patterns Tell Us. American Journal of Public Health, 2010. 100(S1): p. S186-S196.
Ireton, G. History of Aliquippa. 2013 [cited 2013 February 28, 2013]; Available from:
http://www.aliquippapa.gov/aliquippahistory.php.
Bureau, U.C. State & County QuickFacts: Aliquippa (city), Pennsylvania. 2013 January
10, 2013 [cited 2013 January 6]; Available from:
http://quickfacts.census.gov/qfd/states/42/4200820.html.
Bureau, U.S.D.o.C.U.S.C. ACS Demographic and Housing Estimates 2007-2011
American Community Survey 5-Year Estimates. 2013 2011 [cited 2013 February 6];
Available from:
http://factfinder2.census.gov/faces/tableservices/jsf/pages/productiveview.xhtml?=ACS_
11.
Health, P.D.o. EpiQMS: Teen Pregnancy: County. 2013 [cited 2013 January 6];
Available from:
https://apps.health.pa.gov/EpiQMS/asp/SelectParams_Table_TeenPregnancy_County.asp
.
Pregnancy, T.N.C.t.P.T.a.U. State Profiles: Pennsylvania. 2012 2012 [cited 2012
November]; Available from: http://www.thenationalcampaign.org/state-data/stateprofile.aspx?State=pennsylvania.
Joyce A. Martin, M.P.H., et al. Births: Final Data for 2010. National Vital Statistics
Reports, 2012. 61, 72.
Brindis, C.D., A public health success: understanding policy changes related to teen
sexual activity and pregnancy. Annu Rev Public Health, 2006. 27: p. 277-95.
Harris, M.B. and J.G. Allgood, Adolescent pregnancy prevention: Choosing an effective
program that fits. Children and Youth Services Review, 2009. 31(12): p. 1314-1320.
Talashek, M.L., M.L. Alba, and A. Patel, Untangling the health disparities of teen
pregnancy. J Spec Pediatr Nurs, 2006. 11(1): p. 14-27.
Crosby, R.A., et al., Psychosocial predictors of pregnancy among low-income AfricanAmerican adolescent females: a prospective analysis. J Pediatr Adolesc Gynecol, 2002.
15(5): p. 293-9.
Jaccard, J., T. Dodge, and P. Dittus, Do adolescents want to avoid pregnancy? Attitudes
toward pregnancy as predictors of pregnancy. J Adolesc Health, 2003. 33(2): p. 79-83.
46
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
Bennett, S.E. and N.P. Assefi, School-based teenage pregnancy prevention programs: a
systematic review of randomized controlled trials. J Adolesc Health, 2005. 36(1): p. 7281.
Institute, G. Facts on American Teens’ Sexual and Reproductive Health. 2012 2012
[cited 2012 November 7]; Available from: http://www.guttmacher.org/pubs/FBATSRH.pdf.
Klein, J.D., Adolescent pregnancy: current trends and issues. Pediatrics, 2005. 116(1): p.
281-6.
Sipsma, H.L., et al., Adolescent pregnancy desire and pregnancy incidence. Womens
Health Issues, 2011. 21(2): p. 110-6.
Hamilton, B.E. and S.J. Ventura. QuickStats: birth rates for females aged 15-19 years, by
race/ethnicity – national vital statistics system, united states, 2007 and 2011. 2012
October 26, 2012 [cited 2012 November 7]; Available from:
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6142a8.htm?s_cid=mm6142a8_w.
Santelli, J.S., et al., The association of sexual behaviors with socioeconomic status,
family structure, and race/ethnicity among US adolescents. Am J Public Health, 2000.
90(10): p. 1582-8.
Pregnancy, T.N.C.t.P.T.a.U. Teen pregnancy and childbearing among non-hispanic black
teens. Fast Facts 2012 [cited 2012 November]; Available from:
http://www.thenationalcampaign.org/resources/pdf/FastFactsTPChildbearingBlacks.pdf.
Doswell, W.M., et al., Testing the theory of reasoned action in explaining sexual
behavior among African American young teen girls. J Pediatr Nurs, 2011. 26(6): p. e4554.
Pregnancy, T.N.C.t.P.T.a.U. Non-Hispanic Black Teens’ Sexual Behavior and
Contraceptive Use: Data from the Youth Risk Behavior Survey, 2011. Fast Facts 2012
[cited 2012 November 7]; Available from:
http://www.thenationalcampaign.org/resources/pdf/FastFacts_SexualBehavior_Contracep
tiveUse_NHBlacks.pdf.
Prevention, C.f.D.C.a. About Teen Pregnancy. 2012 November 21 2012 [cited 2012
November 7]; Available from: http://www.cdc.gov/TeenPregnancy/AboutTeenPreg.htm.
Ellis, B.J., et al., Does father absence place daughters at special risk for early sexual
activity and teenage pregnancy? Child Dev, 2003. 74(3): p. 801-21.
Hamilton, B.E. and S.J. Ventura. Birth Rates for U.S. Teenagers Reach Historic Lows for
All Age and Ethnic Groups. NCHS Data Brief 2012 April 10, 2012 [cited 2012
November 7]; Available from: http://www.cdc.gov/nchs/data/databriefs/db89.htm.
Pregnancy, T.N.C.t.P.T.a.U. Counting it Up: The Public Costs of Teen Childbearing in
Pennsylvania in 2008. 2011 [cited 2012 November 7]; Available from:
http://www.thenationalcampaign.org/costs/pdf/counting-it-up/fact-sheetpennsylvania.pdf.
Corcoran, J., Multi-Systemic Influences on the Family Functioning of Teens Attending
Pregnancy Prevention Programs. Child and Adolescent Social Work Journal 2001.
18(1): p. 37-49.
Milne, D. and A. Glasier, Preventing repeat pregnancy in adolescents. Curr Opin Obstet
Gynecol, 2008. 20(5): p. 442-6.
Jaccard, J., T. Dodge, and P. Dittus, Maternal discussions about pregnancy and
adolescents, attitudes toward pregnancy. J Adolesc Health, 2003. 33(2): p. 84-7.
47
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
Institute, G. Facts on American Teens' Sources of Information About Sex. In Brief 2012
2012 [cited 2012 November 7]; Available from: http://www.guttmacher.org/pubs/FBTeen-Sex-Ed.html.
Crosby, R.A., et al., Correlates of using dual methods for sexually transmitted diseases
and pregnancy prevention among high-risk African-American female teens. J Adolesc
Health, 2001. 28(5): p. 410-4.
Jeynes, W.H., The effects of religious commitment on the attitudes and behavior of teens
regarding premarital childbirth. J Health Soc Policy, 2003. 17(1): p. 1-17.
McCree, D.H., et al., Religiosity and risky sexual behavior in African-American
adolescent females. J Adolesc Health, 2003. 33(1): p. 2-8.
Upadhya, K.K. and J.M. Ellen, Social disadvantage as a risk for first pregnancy among
adolescent females in the United States. J Adolesc Health, 2011. 49(5): p. 538-41.
Raneri, L.G. and C.M. Wiemann, Social ecological predictors of repeat adolescent
pregnancy. Perspect Sex Reprod Health, 2007. 39(1): p. 39-47.
Gilmore, G.D. and D.M. Campbell, Needs and Capacity Assessment Strategies for Health
Education and Health Promotion2005, Sudbury, Massachusetts: Jones and Bartlett
Publishers. 267.
Gilmore, G.D. and M.D. Campbell, Needs and Capacity Assessment Strategies for Health
Education and Health Promotion2005, Sudbury, Massachusetts: Jones and Bartlett
Publishers. 267.
Schensul, J.J., M.J. Berg, and S. Nair, Using Ethnography in Participatory Community
Assessment, in Methods for Community-Based Participatory Research for Health, B.A.
Israel, et al., Editors. 2013, Jossey-Bass: San Francisco, CA 94104-4594. p. 163, 166.
Hancock, T., Information for Health at the Local Level: Community Stories and Healthy
City Indicators., 1989.
Marti-Costa, S. and S.-G. I., Needs Assessment and Community Development: An
Ideologic Perspective. Prev Hum Serv, 1983. 2(4): p. 75-88.
Rothman, J., Approaches to Community Intervention, in Strategies of Community
Intervention, J. Rothman, J.L. Erlich, and J.E. Tropman, Editors. 2001, F.E. Peacock:
Itasca, IL.
Lasker, R.D. and E.S. Weiss, Broadening Participation in Community Problem Solving:
a Multidisciplinary Model to Support Collaborative Practice and Research Journal of
Urban Health: Bulletin of the New York Academy of Medicine, 2003. 80(1): p. 14-60.
Singleton Jr., R.A. and B.C. Straits, Approaches to Social Research. 5th ed2010, Oxford:
Oxford University Press, Inc. 654.
Prevention, C.f.D.C.a. 2013 State and Local Youth Risk Behavior Survey. Youth Risk
Behavior Surveillance 2013 2013 [cited 2013; Available from:
http://www.cdc.gov/healthyyouth/yrbs/pdf/questionnaire/2013_hs_questionnaire.pdf.
48