TB Clearance Process Requirements for Students/Staff who are
advertisement

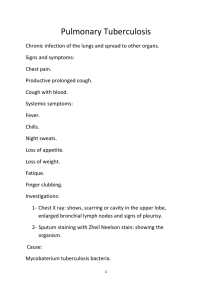
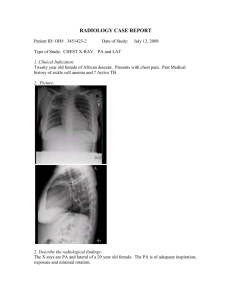
TB Clearance Process Requirements for Students/Staff who are New PPD Skin Test Convertors Definition: New Convertor is a term applied to those persons who had prior history of negative Tuberculosis (TB) skin tests but their most recent one is now positive. Steps Required for TB Clearance Once it has been determined that a student is a new convertor, the following steps are required in order to document and provide TB clearance before the student can be cleared to return to class/work/clinical: 1. Immediate referral to a licensed healthcare provider for health evaluation. 2. AP/Lat Chest x-ray to aid in the exclusion of pulmonary TB (submit copy of the chest x-ray radiology report). 3. Completion of a TB Symptoms Health Screening Checklist (attached) 4. TB Skin Test New Convertor Clearance Form (attached) completed and signed by student and healthcare provider. Upon completion, the TB skin test new convertor clearance form, chest x-ray radiology report and completed TB symptoms health screening checklist must be given to the Student-Employee Health Coordinator (SEHC). The SEHC will then notify the Dean that the student is cleared to return to usual duties. Notification of Removal From Class /Clinical A student with a newly positive Tuberculosis Skin Test (TST) shall be removed from their assignment(s) until they have been seen, evaluated and cleared by a licensed healthcare provider. The student will be advised on what they must do in order to be allowed to return to their assignment. Removal: The College Dean, and/or Clinical Dean shall be notified by the Student-Employee Health Coordinator of this requirement for removal by telephone or in person only. Discussion may be required on determining when the student has to be removed, e.g., student has exam in the next day or two. In order to protect the health of our patients and clinical staff, the student should be relieved of all clinical assignments immediately. Every effort will be made to expedite the health clearance process so that the student can return to their assignment as quickly and safely as possible. Return: Once the student is cleared to return to their assignment, the Student-Employee Health Coordinator will notify, by phone or in person only, the College Dean or Clinical Dean of the clearance to return. Once you are considered to have a positive TST, it is recommended that you do not receive them again. A TB Symptoms Health Screening Checklist form and chest x-ray are recommended for all future TB clearance. TB Skin Test New Convertor Clearance Form STUDENT I, _______________________ have been told that I have been diagnosed with latent tuberculosis infection. My tuberculin skin test was positive at ____mm and/or I had a positive quantiferon test on ___/___/___ showing that I have been infected with the tuberculosis bacteria. ____ I understand I must be seen and evaluated by a healthcare provider in order to obtain TB clearance. ____ I will provide the Student-Employee Health Office with documentation from my healthcare provider regarding my TB clearance on ___/___/___ (needs to be completed within 5 days). ____________________ __________________ __________ __/__/__ Student Name Student Signature ID# Date HEALTHCARE PROVIDER ____ I have reviewed the Tuberculosis Health Screening Checklist completed by the student. ____ I have reviewed the student’s chest x-rays. ____ I have discussed treatment options with the student. ____ I have seen, evaluated, and determined that this student does not have active pulmonary tuberculosis disease. Comments: _____________________________________________ ___________________ ___________________ ___/___/___ Healthcare Provider Name Healthcare Provider Signature Date TB Symptoms Health Screening Checklist Date: ________________________ Student/Employee ID # @____________________ College: COMP Dental MSMS Nursing Campus: Pomona Optometry Name______________________________________________ PT PA Lebanon, OR Pharmacy Grad. Year: _______ Podiatry Vet Med Birth Date___________________________ Address _________________________________________City _______________________ Zip Code_________ Telephone Number ______________________________ Date of last PPD _____________________________________ Date of Quantiferon gold serum test: _____________________ Date of Last Chest X-Ray:_____________ PPD Results ______________ MM Results: __________________ Results: ______ Positive for TB _______ Negative for TB 1. Have you ever been told you have active tuberculosis? ( ) Yes ( ) No 2. Have you ever taken INH or any other anti-TB drug? ( ) Yes ( ) No If yes, list names: 3. Date and duration of medication regime (months) 4. Have you ever had BCG Vaccination? ( ) Yes ( ) No If yes, when? ________________________________ 5. During the past year have you noticed: Unexplained weight loss? ................... ( ) Yes ( ) No Decrease in your appetite? ..................... ( ) Yes ( ) No Cough not associated with cold or flu? ...... ( ) Yes ( ) No Increase in AMOUNT of Sputum? .......... ( ) Yes ( ) No Change in COLOR of Sputum? .......... ( ) Yes ( ) No Change in CONSISTENCY of Sputum? ....... ( ) Yes ( ) No Blood Streaked Sputum?...... ( ) Yes ( ) No Night sweats? ........ ( ) Yes ( ) No Unexplained low grade fever? ..... ( ) Yes ( ) No Unusual tiredness or fatigue? ...... ( ) Yes ( ) No Swelling of lymph nodes? ........... ( ) Yes ( ) No Have you had contact with a family member or partner who has been diagnosed with tuberculosis? ( ) Yes ( ) No Have you or a member of your family been exposed to someone who is immune compromised? ( ) Yes ( ) No Explain any “Yes” answers above: _________________________________________________________________ _____________________________________________________________________________________________ List any on-going medical problem(s): Evaluation : Signature of Reviewer:_____________________________________________________ ________ No further action needed _______Chest X-Ray Requested Date ______ Further Evaluation Needed Must be reviewed by licensed healthcare provider if any “yes” answers TB Symptoms Questionnaire 7-22-10; Rev 4-7-11; 8-12-11; 9-7-11; 6-18-15