Ellen Cheang, MS4 Radiology student conference July 1 , 2011
advertisement

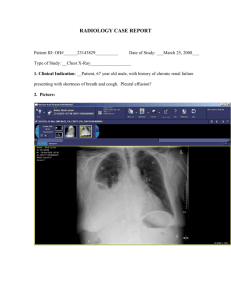
Ellen Cheang, MS4 Radiology student conference July 1st, 2011 Overview Case Presentation - HPI , clinical exams and ddx - Review of our patient’s radiographic findings - Further lab tests Management of empyema - Definition and epidemiology - Discussion of appropriate radiologic test and their indications - Current management guidelines - Literature review and future directions Case presentation HPI: 70 y.o. male presents with 1-week history of dyspnea, dry cough and constant, non-radiating, progressively worsening right-sided chest pain. Denies any fever, chills or weight loss. PMH: 1 mo ago, hospitalized for CAP. Completed 1-wk of abx - Emphysema - Hypertension - Objectives: Vitals: T 99, HR 100, BP 125/80, RR 22, O2 95% RA PE: Crackles , decreased breath sound and dullness to percussion in LLL Labs: WBC 12 (87% PMNs) What’s your differential? Inadequately treated pneumonia - Complicated pneumonia - - Simple/complicated parapneumonic effusion - empyema - necrotizing pneumonia - Primary lung malignancy - Malignant effusion What is your next step of management? What’s the next step? Diagnostic thoracentesis (NEJM 2006;335:e16) Indications: all effusion >1cm in decubitus view Any asymmetry, fever, pleuritic chest pain. Cannot exclude infection clinically If suspect d/t CHF, diurese first and see if effusion resolves in 48-72 hours Diagnostic studies: pH, total protein, LDH, glucose, cell count with diff, gram stain & culture Additional studies should be ordered based on clinical suspicision (e.g. suspected malignancy -> cytology) Transudate vs exudate Light’s criteria (Annals 1972;77:507) - TP eff/ TP serum > 0.5 or LDH eff/LDH serum >0.6 or LDH eff > 2/3 upper normal limit of LDH serum Our patient: pH= 7.01, glucose= 35, LDH = 2100, WBC = 50000 Gram stain positive, culture pending Common causes of transudates Etiology appear WBC diff RBC pH glucose others CHF clear <1000 lymph <5000 normal ~serum bilateral Cirrhosis clear <1000 <5000 normal ~serum R-sided Common causes of exudate Etiology appear WBC diff RBC pH glucos e others Uncomplicated parapneumonic Turbid 5-40,000 polys <5000 >7.2 >40 Abx ok Complicated parapneumonic Turbidpurulent 5-40,000 polys <5000 <7.2 <40 Need drainage Empyema purulent 25-100,000 polys <5000 <7.2 <40 Need drainage Malignancy bloody 1-10,000 ly <100,000 Sl ↓ Sl ↓ +cytology What is your diagnosis? Empyema (Ahmed, et al. Am J Med 2006; Kulman and Singha, Radiographics 1997) Def: The presence of inflammatory debris (pus) in the pleural space due to untreated/undertreated infection (most common cause: bacterial pneumonia) Epi: About 20-60% of pneumonia are associated with parapneumonic effusion, which usually resolve with antibiotic treatment. However, ~1% do not resolve, causing infection and loculated pus in the pleural space. Three phases 1. 2. 3. Exudative: inflammation of the visceral pleura results in weeping of fluid into pleural space Fibinopurulent: inflammatory cells and fibrin accumulate in the pleural space (At this stage, CT may show a “split pleura” sign) Organizing: deposition of collagen and granulation tissue along the visceral & pleural results in pleural fibrosis Empyema: Imaging features Chest radiograph (Study of choice of initial assessment!) - Pleural-based opacity that has an abnormal contour - Does not flow freely on lateral decubitus views - When parapneumonic effusion is suspected, a diagnostic thoracentesis will be the next step - CXR can generally differentiate empyema from lung abscess, CT is not usually indicated! Empyema -Right/obtuse angle with chest wall -Lenticular in shape -Much larger on 1 of 2 right angle projections Lung Abscess -Form an acute angle with chest wall -Spherical in shape -More similar in size on right angle projection What are the indications for Chest CT/ultrasound? Indications for ultrasound - To guide thoracentesis/chest tube placement To assess anatomy in the pediatric population Indications for chest CT To evaluate complex anatomy which cannot be fully assessed by CXR - Differentiate lung abscess and empyema - Suspected pleural masses (e.g. mesothelioma) - Guidance for thoracentesis/chest tube placement when ultrasound is not sufficient - Could CT or ultrasound predict outcomes? Study 1: CT and ultrasound in parapneumonic effusion and empyema (Kearney et al. Clin Radiol. 2000 Jul;55(7):542-7) Aim: To determine if CT and US correlated with the severity of infection and to see if they could predict clinical outcomes Result: There was a trend for mean pleural thickness to increase with an increasing stage of pleural infection but this was not significantly related to the stage of pleural effusion or to the requirement for surgery. No relationship between US appearance, effusion stage or the need of surgical treatment. Conclusion: Neither technique reliably identifies the stage of pleural effusion or predict clinical outcomes Would CT change our management? Study 2: Role of Routune CT in pediatric pleural empyema Jaffe et al. Thorax 2008;63:897-902 Aim: To assess the utility of routine CT scanning and develop a radiologic scoring system for pediatric empyema. Results: - Of the 25 CXRs showing simple opacification of the underlying parenchyma only, CT demonstrated simple consolidation (n = 14), necrotising pneumonia (n = 7), cavitary necrosis (n = 3) and pneumatoceles (n = 1). - No abnormality was detected on CT scanning which directly altered clinical management. - Routine CT was not able to predict length of hospital stay. Conclusion: Chest CT detects more parenchymal abnormalitis than CXR. However, the additional information does not alter management and is unable to predict clinical outcome. Treatment options Systemic antibiotics for at least 4-6 wks Therapeutic thoracentesis Tube thoracostomy Tube thoracostomy + fibrinolytics Video-assisted thoracoscopic surgery (VATS) Surgical decortications Management of parapneumonic effusion AACP guidelines Category Risk of poor outcome Drainage Pleural Space anatomy Pleural Fluid Bacteriology pH 1 very low no Minimal, free flowing effusion (<10mm on LD) unknown unknown 2 low no Small-moderate free flowing effusion (>10mm on LD and <1/2 hemithorax) Negative Gram stain and culture > 7.2 3 moderate yes - Large effusion (>1/2 hemithorax) - Loculated effusion - Thickened parietal pleura Positive gram stain and culture < 7.2 4 high yes Current management guidelines for parapneumonic effusion from ACCP Drainage is recommended for category 3 or 4 Based on the pooled data, therapeutic thoracentesis and chest tube alone appear to be insufficient treatment for category 3 or 4 PPE. However, the panel recognizes individual patient may show complete respond. Careful evaluation is essential in these cases. If resolution occurs, no further intervention is necessary VATS and surgery are acceptable approaches. Data indicates they are associated with lower mortality and need for 2nd interventions. Are large-bore chest tubes better than the small pigtail catheters for drainage? Large vs small chest tubes - Large chest tube have been recommended due to the assumption that smaller tubes would become obstructed with thick fluids - A recent prospective study showed no difference in mortality or the need for 2nd interventions in patients receiving chest tube of different sizes. However, pain scores were higher in patients receiving larger tubes. - Rahman et al. Chest 2010;137;536-543 Large vs small chest tubes - 2 recent studies: 103 and 141 patients with empyema were treated with small-bore catheter inserted under ultrasound or CT guidance. - They showed small tubes served as definitive treatment in 78% and 63% respectively, which were as good as results with using much larger tubes from previous studies . - This suggests correct positioning of the chest tube is more important than its size Shankar et al. Eur Radiol 2000;10:495-499 Chen et al. Ultrasound Med Bio 2009;35:1468-74 In case of complicated PPE/empyema, would fibrinolytics offer better outcomes? Intrapleural fibrinolytics? - Indicated for loculated parapneumonic effusion/empyema Several studies have been done study Size Study groups Results References 1 52 pts Steptokinase vs no tx No difference in the need for 2nd intervention and mortality Chin et.al Chest 1997;111:275-279 3d steptokinase (SK) vs placebo SK group – significant reduction in the size of pleural fluid collection and greater improvement in the CXR Davies et al. Thorax 1997;111:275-279 3d urokinase (UK) vs placebo UK group- 86% showed complete drainage. However, when UK given to pt with incomplete drainage , only 50% showed complete drainage Bouros et al. Am J Resp Crit Care Med 1999;159:37-42 5d urokinase vs placebo UK group- lower need for decortication (29 vs 60%), shorter hospitalization (14d vs 21 d) Tuncozgur et. al. Int J Clin Pract 2001;55: 658-660 Not randomized 2 24 randomized 3 31 randomized 4 49 randomized The results seem promising. What are the problems in the above studies? Small sample size Surrogate endpoint not necessarily correlate with actual clinical endpoint Most recent multicenter, double blind study Maskell N Engl J Med 2005;352: 865-874 - 427 patients were randomized to receive steptokinase vs placebo - No significant differences in between 2 groups in term of mortality, rate of surgery, radiographic outcomes or length of hospital stay - Based on this study, fibrinolytics are not effective in treating loculated (complicated) parapneumonic effusion. The use of fibrinolytics should be reserved for pts in centers without VATS or for pts who are not surgical candidates Drainage alone is unlikely to be the definitive treatment for complicated PPE/empyema. Can VATS potentially be the first line of treatment? Video-assisted thoracic surgery (VATS) A recent review article summarized 14 studies Chambers et al. Int Card and Thor surg 2010;11:171-177 For Stage 2 empyema - VATS vs chest tube+ streptokinase Higher success rate of 91% vs 44%, shorter hospital stay 8.7d vs 12.8 d For stage 3 empyema VATS vs tube thoracostomy Cure rate 88% vs 62%, mortality rate 1.3% vs 11%, hospital stay 14d vs 17d Conclusion: Current guidelines do not recommend VATS as the1st line of tx Studies have consistently shown VATS offers superior outcomes compared to chest tube drainage +/- fibrinolytics Consider VATS as the first step of management in empyema Summary Chest Radiograph remains the most important work-up for the initial dx of pleural effusion Diagnostic thoracentesis gives us the most information about the etiology of the effusion No data suggests Chest CT could predict clinical outcomes or change our management. (expensive + radiation exposure) Large chest tubes are not superior to small chest tubes for drainage Large chest tubes cause more pain to the patients Fibinolytics are not effective in the management of loculated PPE/empyema VATS offers better outcomes compared to tube thoracostomy +/- fibinolytics in complicated PPE/empyema Questions? The proportion of patients dying within each individual cohort (○) and pooled across all studies (♦) is shown for each primary management approach. Colice G L et al. Chest 2000;118:1158-1171 ©2000 by American College of Chest Physicians The proportion of patients requiring a second intervention to manage the PPE within each individual cohort (○) and pooled across all studies (♦) is shown for each primary management approach. Colice G L et al. Chest 2000;118:1158-1171 ©2000 by American College of Chest Physicians