The Costing of Prescribed Minimum Benefits Centre for
advertisement

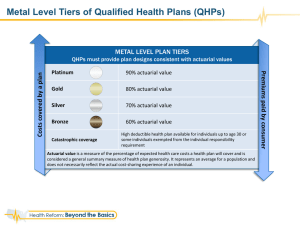
Centre for Actuarial Research The Costing of Prescribed Minimum Benefits January 2003 Söderlund & Peprah (1998) Minimum package defined in terms of diagnosis-treatment pairs. ICD-10 codes for diagnosis element and CPT-4 codes for treatment element. The “core inpatient package” would cost R 502 pbpa in 1998 prices. Data on outpatient services could not be broken down into diagnosis-treatment pairs. Assumption that experience of mine hospital users would apply. Expected outpatient costs of R 183 pbpa. Estimated that total inpatient and outpatient package would cost R 685 pbpa, for those currently without medical scheme cover. Centre for Actuarial Research Definition of the PMB Package Söderlund & Peprah (1998) Minimum package defined in terms of diagnosis-treatment pairs. ICD-10 codes for diagnosis element and CPT-4 codes for treatment element. 1999 Regulations under the Medical Schemes Act No codes in Regulation. Subjective interpretation of PMBs by each scheme. Centre for Actuarial Research Comprehensive Crosswalk Included (IN) as a benefit in the PMB package Excluded (OUT) as a benefit in the PMB package NC (not classifiable) with respect to the PMB package Centre for Actuarial Research PMB Study Data Data from Medscheme Data Warehouse Data covers 2001 calendar year, extracted in July 2002 Data fully run-off, no adjustment for IBNR 90 options 31 schemes 18.071 million beneficiary months of data Average exposure of 1,505,917 beneficiaries Centre for Actuarial Research Data Sets hospital costs related costs Total Costs Average cost per admission hospital costs related costs Total Costs Average cost per admission B Complete data 270,616 R 1,534,270,653 R 614,289,970 R 2,148,560,623 R 7,940 A Total admissions 311,783 R 1,752,659,876 R 684,503,015 R 2,437,162,891 Chapter Analysis Pricing R 7,817 hospital costs related costs Total Costs Average cost per admission C Incomplete data 41,167 R 218,389,223 R 70,213,045 R 288,602,268 R 7,011 Centre for Actuarial Research Cluster Analysis Centre for Actuarial Research Cluster Analysis Different clusters experience different benefit utilisation, costs and disease profiles. Provider behaviour differs by cluster, even within the same hospital facility. Distinct clusters: High contains options with older, 'whiter' members with high utilisation; Medium-older contains options with medium utilisation and older members; Medium-younger contains options with medium utilisation and younger members; and Low contains options with younger, 'blacker' members with low utilisation. Centre for Actuarial Research Beneficiaries in Study 8.8% High 9.6% Medium-older Medium-younger Low 10.1% 71.6% Centre for Actuarial Research Contributions and Benefits 2500 2010 Rands pmpm 2000 1787 1593 1500 1121 1188 Contributions 1074 902 1000 732 Benefits 500 0 High Medium Older Medium Younger Low Cluster Q1 2002 Data Centre for Actuarial Research Proportion of Beneficiaries Over Age 55 30% 26.3% High 18.4% 20% Medium-older 15% Medium-younger 9.7% 10% 8.5% Low Total 5.0% 5% Total Low Mediumyounger Mediumolder 0% High Proportion 25% Cluster Centre for Actuarial Research Proportion of African/Black Beneficiaries 77.1% 80% 70% 61.0% High 50% Medium-older 40% Medium-younger 30% 15.8% 16.3% Mediumolder 20% Low 22.2% High Total 10% Cluster Total Low 0% Mediumyounger Proportion 60% Centre for Actuarial Research Applicability to the Industry Centre for Actuarial Research Simplified Age Profiles of the Study and Industry 100% 90% 80% 70% 55 + 60% 20 - 54 50% 0 - 19 40% 30% 20% 10% SHI+PS Industry High and Medium Study Total Low Mediumyounger Medium-older High 0% Centre for Actuarial Research Detailed Age Profile of the Industry and Study 13% 12% 8% 7% 6% 5% 4% 3% Registrar's Returns 2000 Adjusted OHS99 Unadjusted 75 + 70 - 74 65 - 69 60 - 64 55 - 59 50 - 54 45 - 49 40 - 44 35 - 39 30 - 34 25 - 29 20 - 24 15 - 19 10 - 14 5-9 2% 1% 0% 0-4 Proportion 11% 10% 9% CARE PMB Study Centre for Actuarial Research Ethnicity Summary 100% 90% 80% W h ite 70% O th e r 60% C o lo u re d 50% Afric a n /B la c k 40% In d ia n /As ia n 30% 20% 10% SHI+PS Indus try High and Medium Total Low Medium younger Medium older High 0% Centre for Actuarial Research Weighted Industry Total Study contains more Low cluster beneficiaries than the industry. Re-weighted total to give closer demographic fit to industry data: 100% High cluster 100% Medium-older cluster 100% Medium-younger cluster 50% Low cluster Weighted industry total gives exact matching of beneficiaries over age 55; closer to ethnicity Low cluster is more relevant to the emerging low-cost option environment. Centre for Actuarial Research Cost of PMBs by Cluster Centre for Actuarial Research Admission Count by Status Included Not Classifiable 38.6% Out 47.2% 14.2% Centre for Actuarial Research Claim Value by Status Included 32.1% Not Classifiable Out 55.1% 12.8% Centre for Actuarial Research Average Cost by Status R 10,000 R 9,127 R 7,817 R 8,000 R 7,041 R 6,502 R 6,000 R 4,000 R 2,000 R0 Included Not Classifiable Out Total Claim s Paid Centre for Actuarial Research Proportion of Status by Cluster 100% 90% Proportion 80% 70% Out 60% Not Classifiable 50% Included 40% 30% 20% 10% 0% High Medium - Medium older younger Low Total Centre for Actuarial Research Incidence of PMB Admissions by Cluster 150 141.92 118.84 Incidence per 1000 108.57 97.69 87.90 100 50 0 High Medium older Medium younger Low Total Centre for Actuarial Research Average Cost of PMBs by Cluster R 14,000 R 11,478 R 11,372 R 12,000 R 9,043 Average Cost R 10,000 R 9,127 R 8,270 R 8,000 R 6,000 R 4,000 R 2,000 R0 High Medium older Medium younger Low Total Centre for Actuarial Research Cost of PMBs by Disease Chapter Centre for Actuarial Research 0% Gynaecology Genitourinary Endocrine Skin/Breast MS/Trauma HSP GIT Cardiac Mental Illness Haem-Infect Obstetrics-Neonate OUT INCLUDED Respiratory ENT Eye CNS Proportion of Admissions by Disease Chapter 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% Centre for Actuarial Research 0% Gynaecology Genitourinary Endocrine Skin/Breast MS/Trauma HSP GIT Cardiac Mental Illness Haem-Infect Obstetrics-Neonate OUT INCLUDED Respiratory ENT Eye CNS Proportion of Claim Value by Disease Chapter 100% 80% 60% 40% 20% Centre for Actuarial Research Proportion of Total Cost of PMBs by Disease Chapter Mental Illness Other 2.6% Haem-Infect 3.2% CNS 9.5% 3.9% Eye 3.9% ENT 1.6% Obstetrics Neonate 17.3% Respiratory 10.5% Gynaecology 4.5% Genitourinary 2.7% Endocrine 2.2% Skin/Breast 3.4% MS/Trauma 6.3% Cardiac 12.8% HSP 3.2% GIT 12.2% Centre for Actuarial Research Total Other Mental Illness Haem-Infect Obstetrics - Neonate Gynaecology Genitourinary Endocrine Skin/Breast MS/Trauma HSP GIT Cardiac Respiratory ENT Eye CNS Average Cost Average Cost of PMBs by Disease Chapter R 20,000 R 18,000 R 16,000 R 14,000 R 12,000 R 10,000 R 8,000 R 6,000 R 4,000 R 2,000 R0 Centre for Actuarial Research R0 High Gynaecology Genitourinary Endocrine Skin/breast MS/Trauma HSP GIT Cardiac Respiratory Other Mental illness Haem-Infect Obstetrics-Neonate Low ENT EYE CNS Average Cost Average Cost by Chapter High vs. Low Clusters R 25,000 R 20,000 R 15,000 R 10,000 R 5,000 Centre for Actuarial Research Differences in Cluster Costs Not simply different costs charged by providers for the same diagnoses. Issue is much more complex. Very different age and demographic profiles. Age difference would account for significant differences in diagnoses, e.g. mainly meningitis in Low cluster and stroke in High cluster in CNS chapter. Condition perhaps not diagnosed as frequently in Low cluster due to differences in access to doctors: Low cluster biased towards GPs , High cluster prefer specialists. Also benefit design, severity of disease and provider and patient demand. Centre for Actuarial Research Top Five Disease Chapters High vs. Low Cluster HIGH Chapter Cardiac GIT CNS Respiratory EYE Chapter Obstetrics-Neonatal Respiratory GIT Cardiac CNS PMB Claims Paid R 38,300,784 R 21,487,290 R 21,895,197 R 16,430,848 R 11,939,964 Count of PMB Admissions 1,665 2,331 1,247 1,571 1,409 LOW PMB Claims Paid Count of PMB Admissions R 150,089,803 R 83,372,298 R 82,341,347 R 63,010,421 R 59,661,085 15,351 11,645 11,225 3,952 5,191 Average PMB Proportion of Cost per Total Admission PMBClaims R 23,003 R 9,218 R 17,558 R 10,459 R 8,474 22.0% 12.3% 12.6% 9.4% 6.9% Average PMB Proportion of Cost per Total Admission PMBClaims R 9,777 R 7,159 R 7,336 R 15,944 R 11,493 21.1% 11.7% 11.6% 8.9% 8.4% Centre for Actuarial Research Diagnoses by Disease Chapter Top 10 diagnoses (ICD-10 codes) in the PMB schedule, ranked by claim value (i.e. total cost), usually account for more than 70% of total cost in each chapter. Surprising since most chapters contain approximately 100 diagnoses (ICD-10 codes). Probably a reflection of the state of coding in SA, rather than a true concentration of diagnoses. Centre for Actuarial Research Pregnancy and Childbirth ICD-10 CODE O82 O80 O82.9 O80.9 P22.9 O82.0 O80.0 P22 P07.3 O82.1 ICD10 CODE LABEL Single delivery by caesarean section Single spontaneous delivery Delivery by caesarean section, unspecified Single spontaneous delivery, unspecified Respiratory distress of newborn, unspecified Delivery by elective caesarean section Spontaneous vertex delivery Respiratory distress of newborn Other preterm infants Delivery by emergency caesarean section Total claim value of top ten conditions Remaining 257 disease classifications Total claim value Total Costs R 43,222,469 R 22,698,932 R 22,437,961 R 19,409,924 R 14,744,032 R 13,678,782 R 10,233,464 R 8,460,302 R 8,323,304 R 7,830,086 R 171,039,257 R 34,522,317 R 205,561,574 Proportion of Count of Total claim Admissions value 21.03% 3,920 11.04% 3,237 10.92% 1,993 9.44% 2,623 7.17% 461 6.65% 1,192 4.98% 1,389 4.12% 289 4.05% 225 3.81% 667 83.21% 15,996 16.79% 4,574 100.00% 20,570 Average Cost per Admission R 11,026 R 7,012 R 11,258 R 7,400 R 31,983 R 11,475 R 7,368 R 29,274 R 36,992 R 11,739 R 10,693 R 7,548 R 9,994 Centre for Actuarial Research Cost of PMBs by Age Centre for Actuarial Research Age Profile of Study 15.00% Total High Medium-older Medium-younger Low 10.00% 5.00% 75+ 70-75 65-70 60-65 55-60 50-55 45-50 40-45 35-40 30-35 25-30 20-25 15-20 10-15 5-10 1-5 0-1 0.00% Centre for Actuarial Research Age Profile Beneficiaries Admitted for PMBs Total High Medium-older Medium-younger Low 20.00% 15.00% 10.00% 5.00% 75+ 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 1-4 0-1 0.00% Centre for Actuarial Research Incidence of PMB Admissions by Age 450 Total High Medium-older Medium-younger Low 400 350 250 200 150 100 50 75+ 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 1-4 0 0-1 Incidence 300 Centre for Actuarial Research Average Cost of PMBs by Age 1 8 ,0 0 0 1 6 ,0 0 0 1 4 ,0 0 0 1 0 ,0 0 0 R9 127 8 ,0 0 0 6 ,0 0 0 4 ,0 0 0 Average Cost for All Ages 2 ,0 0 0 A ll ages 75+ 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 1-4 0 0-1 Ave r age Cos t 1 2 ,0 0 0 Centre for Actuarial Research Average Cost of PMBs by Age Total High Medium-older Medium-younger Low R 18,000 R 16,000 R 12,000 R 10,000 R 8,000 R 6,000 R 4,000 R 2,000 75+ 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 1-4 R0 0-1 Aerage Cost in Rands R 14,000 Centre for Actuarial Research Raw Price of PMBs Centre for Actuarial Research Annual PMB Price by Cluster (pbpa) R 2,000 R 1629.03 R 1,500 R 310.33 R 1351.49 R 137.02 R 981.79 R 891.56 R 1,000 R 158.61 R 1,318.70 R 104.76 R 67.65 R 1,214.46 R 500 R 726.92 R 823.17 R 659.27 R 786.80 R0 High SET C PMB SET B PMB Medium older Medium younger Low Total Centre for Actuarial Research Raw PMB Price by Age (pbpa) R 5 ,0 0 0 R 4 ,5 0 0 R 4 ,0 0 0 R 3 ,5 0 0 Average Price for All Ages R 3 ,0 0 0 R 2 ,5 0 0 R 2 ,0 0 0 R 1 ,5 0 0 R 1 ,0 0 0 R 891.56 pbpa R 500 75+ 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 A ll ages S ET C PM B 1-4 0-1 R 0 S ET B PM B Centre for Actuarial Research Raw PMB Price by Age and Cluster (pbpa) R 6,000 Total High Medium-older Medium-younger Low R 5,000 R 4,000 R 3,000 R 2,000 R 1,000 75+ 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 1-4 0-1 R0 Centre for Actuarial Research Raw PMB Price by Wider Age Bands (pbpa) R 3,000 R2710.94 R 2,500 SET C PMB SET B PMB R 2,000 R 1,500 R1264.53 R1 017.71 R 891.56 R 1,000 R 500 R 368.69 R0 < 20 20-54 >55 Total Adults All ages Centre for Actuarial Research Adjustments to the Raw Price of the PMB Package Centre for Actuarial Research Adjustments to Raw Price Uncertainty in Definition of the PMB Package Recoding the OUT Group Recoding the NC Group Costs of hospital management programme Costs of hospital and related claims administration Costs of chemotherapy and dialysis Costs related to HIV/AIDS Estimate of the cost of ambulatory care Costs of ambulatory administration Reduction for cost of delivery in the public sector Centre for Actuarial Research Recoding of Out Group Coding originally done by Söderlund was open to debate among healthcare professionals. No clear definitions in Act so ICD-10 codes placed into IN, OUT or NC on a subjective basis. Reviewed all 1 614 ICD-10 codes classified as OUT. New coding moved 19.8% of admissions of OUT group to IN group. Claim value was 27.0% of the original OUT category. Raw price for PMBs for all clusters increases from R 786.80 pbpa to R 910.14 pbpa, an increase of 13.5%. Recommendation: allow for 27.0% of the OUT category by value to be included in the final price. Centre for Actuarial Research Recoding of NC Group NC group is more complicated to recode, as many conditions need to be linked to CPT-4 codes. Recommendation: stress-test final price using various estimates of proportion of NC that might be included in a better-defined PMB package. Recommended estimate is to include 20% of the NC group by value in the final price. Centre for Actuarial Research Hospital Management Costs Total Hospital Management Cluster High Medium-older Medium-younger High and Medium Low Total Price per benficiary per month R 5.43 R 4.55 R 4.16 R 4.69 R 3.17 R 3.60 Price per benficiary per annum R 65.18 R 54.65 R 49.98 R 56.24 R 38.05 R 43.22 PMB Hospital Management Price per benficiary per month R 2.47 R 2.07 R 1.89 R 2.13 R 1.53 R 1.70 Price per benficiary per annum R 29.63 R 24.81 R 22.66 R 25.53 R 18.35 R 20.39 Centre for Actuarial Research Hospital and Related Claims Administration Total Hospital and Related Claims Administration Cluster High Medium-older Medium-younger High and Medium Low Total Price per benficiary per month R 6.12 R 5.13 R 4.69 R 5.28 R 3.57 R 4.06 Price per benficiary per annum R 73.46 R 61.59 R 56.33 R 63.39 R 42.88 R 48.71 PMB Hospital and Related Claims Administration Price per benficiary per month R 2.78 R 2.33 R 2.13 R 2.40 R 1.72 R 1.92 Price per benficiary per annum R 33.39 R 27.96 R 25.54 R 28.78 R 20.68 R 22.98 Centre for Actuarial Research Chemotherapy and Dialysis Treatable malignancies and chronic renal failure most frequently managed in outpatient setting. Clarity in Regulation November 2002 that these are included in PMBs. Figures described as “very preliminary”. Need further work. Recommendation: use R12 pbpa for chronic renal failure and R36 pbpa for chemotherapy. Centre for Actuarial Research Regulations November 2002 Note: (2A) In respect of treatments denoted as “medical management”, note (2) above describes the standard of treatment required, namely “prevailing hospital-based medical or surgical diagnostic and treatment practice for the specified condition”. Note (2) does not restrict the setting in which the relevant care should be provided, and should not be construed as preventing the delivery of any prescribed minimum benefit on an outpatient basis or in a setting other than a hospital, where this is clinically most appropriate. Centre for Actuarial Research Costs related to HIV/AIDS Only 9 admissions coded 168S (Diagnosis: # HIVAssociated Disease). Confidential data from Aid-for-AIDS programme will not be obvious. Costs of related conditions and complications are identified in categories such as pneumonia, encephalitis, TB etc. Available for further analysis. Study almost certainly incorporates the cost and pricing of hospitalisation of symptomatic AIDS, as at 2001. Recommendation: Allow for impact of increased hospitalisation for HIV/AIDS in later stages of epidemic. Obtain advice from Actuarial Society of South Africa’s AIDS Subcommittee. Centre for Actuarial Research Estimate of Additional Cost of Ambulatory Care Condition Non-hospital, Non-drug Requirements Estimate of Additional Costs Pregnancy Antenatal visits and care including office- and laboratory-based investigations such as VDRL and ultrasound R 2,500 per patient per episode Asthma Costs of GP, Specialist, Casualty Dept visits, nebulisers, asthma pumps, lung function tests R 1,900 per patient per year Diabetes Costs of GP, Specialist, Dietician and other provider visits, glucometers, test strips, laboratory investigations such as HbA1c R 2,100 per patient per year Hyperlipidaemia Costs of GP and Specialist visits plus blood tests and related clinical tests such as ECGs R 1,200 per patient per year Epilepsy Costs of GP and Specialist visits, EEGs and drug R 1,100 per patient levels per year Centre for Actuarial Research Ratio of Ambulatory to Inpatient Expenditure Söderlund (1998) used 36.5% 70.00% 60.00% 50.00% 40.00% 30.00% 20.00% 10.00% Source: Van den Heever using OECD database United States Turkey Switzerland Spain Norway New Zealand Netherlands Luxembourg Korea Japan Italy Iceland Germany France Finland Denmark Czech Republic Canada Belgium Austria Australia 0.00% Centre for Actuarial Research Estimate of Ambulatory Care Amount paid to hospital groups, less admissions, was R314 million. Includes out-patient visits, on-going tests performed in a hospital setting, dispensing from the hospital pharmacy, emergency room visits for conditions such as asthma and diabetes, and costs for certain dialysis centres. Chemotherapy and dialysis separately estimated. Caution overlap with CDL package. Recommendation: use 15% as estimate for ratio of other ambulatory expenditure to in-patient expenditure for the PMB package, excluding the CDL package. Centre for Actuarial Research Ambulatory Administration Scanty information. Level of pre-authorisation and management will be much lower and will apply only to certain tests. Administration of claims will require much less intensive activity. Recommendation: If the other ambulatory expenditure estimate is held at the recommended level of 15%, then use 10% of the non-health care costs of the in-patient PMB package, as the estimate for the costs of ambulatory administration. Centre for Actuarial Research Delivery of PMBs in the Public Sector Centre for Actuarial Research Public Sector vs. Private Sector Costs: PAWC Study of Selected Conditions PAWC Procedure / Diagnosis UPFS Total (2002 tariffs) Comparisons PMB Study Low - LOS BHF Total comparative with (2002 tariffs) BHF UPFS (2002) Relative to BHF (2002) PMB Study (2001) Relative to BHF (2002) Appendectomy R 3,115 R 5,421 R 3,836 57.5% 70.8% Unstable angina; coronary angiogram; PTCA R 9,284 R 76,866 R 24,735 12.1% 32.2% Cataract and IOL R 1,605 R 32,609 4.9% R 31,439 R 111,296 28.2% Confinement - C/section R 6,494 R 10,015 Confinement - NVD R 5,571 R 6,211 Congestive Cardiac Failure R 2,720 R 4,657 Gastroscopy - epigastric pain R 1,178 R 798 Pneumonia R 2,583 R 3,366 Colonoscopy - Lower GI bleed R 1,178 R 571 Tonsillectomy R 2,584 R 1,962 R 3,301 131.7% 168.3% Myocardial Infarction R 7,962 R 47,137 R 6,986 16.9% 14.8% Hysterectomy -mennorhagia R 7,950 R 17,067 46.6% R 12,723 R 16,938 75.1% CABG x3, harvesting saphenous veins Laparotomy - large bowel obstruction (partial colectomy) R 11,436 64.8% 114.2% 89.7% R 8,036 58.4% 172.6% 147.6% R 3,854 76.7% 114.5% 206.3% Centre for Actuarial Research Public vs. Private sector Costs for Appendicectomy Setting and Population Claims Paid Count of Admissions Public sector District Hospital (estimate) Public sector Academic Hospital (estimate) Average Cost per Admission R 3,820 R 4,752 Private sector High Cluster (Actual cost all admissions) R 2,363,000 292 R 8,092 Private sector Low Cluster (Actual cost all admissions) R 12,498,159 1,639 R 7,625 Private sector High Cluster (Actual cost for 4 days or less) R 1,790,051 258 R 6,938 Private sector Low Cluster (Actual cost for 4 days or less) R 9,187,697 1,413 R 6,502 34.08% higher than public sector Centre for Actuarial Research Length of Stay for Appendicectomy for Low Cluster 900 800 763 650 Count of Admissions 700 600 500 Complications 400 300 161 200 47 100 8 9 1 6 8 10 Length of Stay in Days 12 0 2 4 86.2% hospitalised for 4 days or less. Maximum stay was 43.5 days. 12+ Centre for Actuarial Research PMB Cost in the Public Sector Studies available use theoretical cases. Attempts to compare actual costs of public and private sector admissions uncovered unexpected finding that not all provinces were billing using UPFS system in 2001. Need to definitively determine the relationship between UPFS costs in the public sector and costs in the private sector. DoH study now underway. Recommendation: use 70% of PMB price for delivery of PMB Inpatient package and PMB Outpatient package in public sector. Adjust in negotiations with provincial authorities. Centre for Actuarial Research Full Price of Existing PMB Package Centre for Actuarial Research Full Price of PMB Package Four components : In-patient PMB package price based on full data in study (high degree of certainty) Portion of price for which uncertainty exists in PMB definition (proportion to include of NC and OUT) Margin added for ambulatory costs Non-healthcare costs. Note: Prices should not be used blindly in pricing work. Contact a professional for assistance. Centre for Actuarial Research Full Price of PMBs (excl CDL) R 2,500.00 Non-healthcare costs Ambulatory package Uncertainty in PMB definition In-patient PMB package R2 432.41 R2 010.90 R1 956.01 Per Beneficiary Per Annum R 2,000.00 R1 479.04 R1 489.49 R 1,500.00 R1 343.43 R1 100.08 R 1,000.00 R 500.00 R 0.00 High Medium- Medium- High and older Younger Medium Low Total Study Weighted Total Centre for Actuarial Research Full Price PMB Package (excluding CDL) Price per beneficiary per annum (in 2001 Rand terms) Total Inpatient package Total Outpatient package High Mediumolder MediumYounger High and Medium R 2,076.97 R 1,709.86 R 1,256.20 R 1,662.21 R 355.44 R 301.04 R 233.29 R 293.79 Low Total Study Weighted Total R 917.01 R 1,128.88 R 1,246.95 R 183.07 R 214.55 R 232.10 PMB package (excl. CDL) Private Sector R 2,432.41 R 2,010.90 R 1,489.49 R 1,956.01 R 1,100.08 R 1,343.43 R 1,479.04 PMB package (excl. CDL) Public Sector R 1,716.72 R 1,419.39 R 1,053.40 R 1,381.31 R 778.53 R 949.91 R 1,045.41 Centre for Actuarial Research Non-healthcare Expenditure Non-healthcare Expenditure as a Proportion of … High Mediumolder MediumYounger High and Medium Low Total Study Weighted Total Total Inpatient package 3.9% 4.0% 5.0% 4.3% 5.4% 4.9% 4.7% Total Outpatient package 2.3% 2.3% 2.7% 2.4% 2.7% 2.6% 2.5% Total PMB package (excluding CDL) 3.7% 3.8% 4.6% 4.0% 5.0% 4.6% 4.4% Well below Registrar’s benchmark of 10% of total expenditure Centre for Actuarial Research PMB Package Relative to Industry Hospital Expenditure Per Beneficiary per Annum R 2,500 PMB package (excluding CDL) Schemes in PMB Study Open non-study schemes Restricted non-study schemes 2,034 R 2,000 1,762 1,449 R 1,500 1,741 1,414 1,296 1,181 R 1,000 854 R 500 R0 Hospital only Hospital plus related Centre for Actuarial Research PMB Package Relative to Benefits and Contributions R 6,000 Per Beneficiary per Annum R 5,000 5,760 PMB package (excluding CDL) Schemes in PMB Study Open non-study schemes Restricted non-study schemes 4,668 4,772 4,285 5,613 5,013 R 4,000 R 3,000 R 2,000 1,479 1,414 R 1,000 R0 Total Benefits Contributions Centre for Actuarial Research Conclusions Centre for Actuarial Research Preliminary Conclusions on Affordability The PMB package (excluding CDL) appears to be affordable compared to hospital benefits and the proxy for hospital and related benefits. The package also appears to be well covered when compared to the level of total benefits and contributions at an industry level. Centre for Actuarial Research Improvements to PMB Definition All stakeholders need an unambiguous definition of the PMB package. The Council for Medical Schemes is requested to reconsider the definition of PMBs in the Regulations and to include clear diagnosis and procedure codes in an amendment as soon as possible. Tighter definition of PMBs would ensure more focussed attention on accurate coding from providers and administrators. Attention should be given to the nature of the chapters and to bringing them in line with clinical practice or a particular coding standard. Centre for Actuarial Research Public Sector vs. Private Sector Approaches to Treatment As yet, no coherent approach to defining the basic essential minimum services between the public and private sectors. Far more agreement and convergence are required in terms of public vs. private sector approaches to common conditions. Admission to hospital is the norm in the private sector but not in the public sector where some events are regarded as being non-acute in terms of PMBs. Agreement is needed on the roles of new generation prostheses, devices, immune modulators, gene therapy, procedures and drugs. Centre for Actuarial Research Comprehensive Crosswalk Provides a powerful tool for rapid application of PMB status to hospital admissions based on ICD-10 coding Strongly recommend that this should be made freely available to other medical schemes and administrators, in order to improve their understanding and management of PMBs. Recommend utilising this tool, or one developed from this work, to define and manage the PMB package in future. Centre for Actuarial Research Further Research It is now possible (within a few minutes), to extract data for a specific ICD-coded diagnosis with its accompanying costs, related length of stay, age data and cluster data. These can also be expanded to include ethnicity, scheme options and provider information. This information can be grouped into clusters, age bands, and disease patterns depending on the requirements of the user. This opens the possibility of doing much valuable and detailed analysis of specific problem areas in the PMB definitions in order to refine the PMB package. Several projects planned for 2003 at UCT using this data. Centre for Actuarial Research Centre for Actuarial Research (CARE) A Research Unit of the University of Cape Town A Research Report Prepared Under Contract for the Council for Medical Schemes Centre for Actuarial Research