Pediatric Shock Recognition, Classification and Initial Management Critical Concepts Course
advertisement

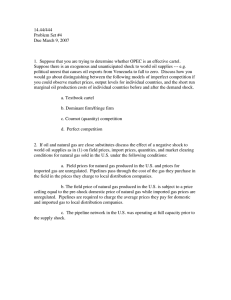
Pediatric Shock Recognition, Classification and Initial Management Critical Concepts Course Introduction Shock is a syndrome that results from inadequate oxygen delivery to meet metabolic demands Oxygen delivery (DO2 ) is less than Oxygen Consumption (< VO2) Untreated this leads to metabolic acidosis, organ dysfunction and death Oxygen Delivery Oxygen delivery = Cardiac Output x Arterial Oxygen Content (DO2 = CO x CaO2) Cardiac Output = Heart Rate x Stroke Volume (CO = HR x SV) – SV determined by preload, afterload and contractility Art Oxygen Content = Oxygen content of the RBC + the oxygen dissolved in plasma (CaO2 = Hb X SaO2 X 1.34 + (.003 X PaO2) Figure 1. FACTORS AFFECTING OXYGEN DELIVERY Hgb CaO2 A-a gradient DPG Acid-Base Balance Blockers Competitors Temperature Influenced By Oxygenation DO2 Influenced By Drugs Conduction System HR CO EDV SV CVP Venous Volume Venous Tone Ventricular Compliance Influenced By ESV Contractility Influenced By Afterload Temperature Drugs Metabolic Milieu Ions Acid Base Temperature Drugs Toxins Blockers Competitors Autonomic Tone Stages of Shock Compensated – Vital organ function maintained, BP remains normal. Uncompensated – Microvascular perfusion becomes marginal. Organ and cellular function deteriorate. Hypotension develops. Irreversible Clinical Presentation Early diagnosis requires a high index of suspicion Diagnosis is made through the physical examination focused on tissue perfusion Abject hypotension is a late and premorbid sign Initial Evaluation: Physical Exam Findings of Shock Neurological: Fluctuating mental status, sunken fontanel Skin and extremities: Cool, pallor, mottling, cyanosis, poor cap refill, weak pulses, poor muscle tone. Cardio-pulmonary: Hyperpnea, tachycardia. Renal: Scant, concentrated urine Initial Evaluation: Directed History Past medical history – heart disease – surgeries – steroid use – medical problems Brief history of present illness – exposures – onset Differential Diagnosis of Shock Hypovolemic Myocardial dysfunction Dysrrhythmia Congenital heart Hemorrhage Fluid loss Drugs Distributive Analphylactic Neurogenic Septic Cardiogenic disease Obstructive Pneumothorax, CardiacTamponade, Aortic Dissection Dissociative Heat, Carbon monoxide, Cyanide Endocrine Differential Diagnosis of Shock Precise etiologic classification may be delayed Immediate treatment is essential Absolute or relative hypovolemia is usually present Neonate in Shock: Include in differential: Congenital adrenal hyperplasia Inborn errors of metabolism Obstructive left sided cardiac lesions: – Aortic stenosis – Hypoplastic left heart syndrome – Coarctation of the aorta – Interrupted aortic arch Management-General Goal: increase oxygen delivery and decrease oxygen demand: For all children: ○ Oxygen ○ Fluid ○ Temperature control ○ Correct metabolic abnormalities Depending on suspected cause: ○ Antibiotics ○ Inotropes ○ Mechanical Ventilation Management-General Airway If not protected or unable to be maintained, intubate. Breathing Always give 100% oxygen to start Sat monitor Circulation Establish IV access rapidly CR monitor and frequent BP Management-General Laboratory studies: – ABG – Blood sugar – Electrolytes – CBC – PT/PTT – Type and cross – Cultures Management-Volume Expansion Optimize preload Normal saline (NS) or lactated ringer’s (RL) Except for myocardial failure use 1020ml/kg every 2-10 minutes. Reasses after every bolus. At 60ml/kg consider: ongoing losses, adrenal insufficiency, intestinal ischemia, obstructive shock. Get CXR. May need inotropes. Fluid in early septic shock Carcillo, et al, JAMA, 1991 Retrospective review of 34 pediatric patients with culture + septic shock, from 1982-1989. Hypovolemia determined by PCWP, u.o and hypotension. Overall, patients received 33 cc/kg at 1 hour and 95 cc/kg at 6 hours. Three groups: – 1: received up to 20 cc/kg in 1st 1 hour – 2: received 20-40 cc/kg in 1st hour – 3: received greater than 40 cc/kg in 1st hour No difference in ARDS between the 3 groups Fluid in early septic shock Carcillo, et al, JAMA, 1991 Group 1 Group 2 Group 3 (n = 14) Hypovolemic at 6 hours -Deaths Not hypovolemic at 6 hours -Deaths Total deaths (n = 11) (n = 9) 6 2 0 6 8 2 9 0 9 2 8 5 7 1 1 Inotropes and Vasopressors Lack of history of fluid losses, history of heart disease, hepatomegaly, rales, cardiomegaly and failure to improve perfusion with adequate oxygenation, ventilation, heart rate, and volume expansion suggests a cardiogenic or distributive component. Consider Appropriate inotropic or vasopressor support. Hypovolemic Shock Most common form of shock world-wide Results in decreased circulating blood volume, decrease in preload, decreased stroke volume and resultant decrease in cardiac output. Etiology: Hemorrhage, renal and/or GI fluid losses, capillary leak syndromes Hypovolemic Shock Clinically, history of vomiting/diarrhea or trauma/blood loss Signs of dehydration: dry mucous membranes, absent tears, decreased skin turgor Hypotension, tachycardia without signs of congestive heart failure Hemorrhagic Shock Most common cause of shock in the United States (due to trauma) Patients present with an obvious history (but in child abuse history may be misleading) Site of blood loss obvious or concealed (liver, spleen, intracranial, GI, long bone fracture) Hypotension, tachycardia and pallor Hypovolemic/Hemorrhagic Shock: Therapy Always begin with ABCs Replace circulating blood volume rapidly: start with crystalloid Blood products as soon as available for hemorrhagic shock (Type and Cross with first blood draw) Replace ongoing fluid/blood losses & treat the underlying cause Septic Shock SIRS/Sepsis/Septic shock Mediator release: exogenous & endogenous Maldistribution Cardiac of blood flow dysfunction Imbalance of oxygen supply and demand Alterations in metabolism Septic Shock: “Warm Shock” Early, compensated, hyperdynamic state Clinical signs Warm extremities with bounding pulses, tachycardia, tachypnea, confusion. Physiologic parameters widened pulse pressure, increased cardiac ouptut and mixed venous saturation, decreased systemic vascular resistance. Biochemical evidence: Hypocarbia, elevated lactate, hyperglycemia Septic Shock: “Cold Shock” Late, uncompensated stage with drop in cardiac output. Clinical signs Cyanosis, cold and clammy skin, rapid thready pulses, shallow respirations. Physiologic parameters Decreased mixed venous sats, cardiac output and CVP, increased SVR, thrombocytopenia, oliguria, myocardial dysfunction, capillary leak Biochemical abnormalities Metabolic acidosis, hypoxia, coagulopathy, hypoglycemia. Septic Shock Cold Shock rapidly progresses to mutiorgan system failure or death if untreated Multi-Organ System Failure: Coma, ARDS, CHF, Renal Failure, Ileus or GI hemorrhage, DIC More organ systems involved, worse the prognosis Therapy: ABCs, fluid Appropriate antibiotics, treatment of underlying cause Cardiogenic Shock Etiology: – Dysrhythmias – Infection (myocarditis) – Metabolic – Obstructive – Drug intoxication – Congenital heart disease – Trauma Cardiogenic Shock Differentiation from other types of shock: – History – Exam: Enlarged liver Gallop rhythm Murmur Rales – CXR: Enlarged heart, pulmonary venous congestion Cardiogenic Shock Management: – Improve cardiac output:: Correct dysrhthymias Optimize preload Improve contractility Reduce afterload – Minimize cardiac work: Maintain normal temperature Sedation Intubation and mechanical ventilation Correct anemia Distributive Shock Due to an abnormality in vascular tone leading to peripheral pooling of blood with a relative hypovolemia. Etiology – – – – Anaphylaxis Drug toxicity Neurologic injury Early sepsis Management – – Fluid Treat underlying cause Obstructive Shock Mechanical obstruction to ventricular outflow Etiology: Congenital heart disease, massive pulmonary embolism, tension pneumothorax, cardiac tamponade Inadequate C.O. in the face of adequate preload and contractility Treat underlying cause. Dissociative Shock Inability of Hemoglobin molecule to give up the oxygen to tissues Etiology: Carbon Monoxide poisoning, methemoglobinemia, dyshemoglobinemias Tissue perfusion is adequate, but oxygen release to tissue is abnormal Early recognition and treatment of the cause is main therapy Hemodynamic Variables in Different Shock States CO SVR MAP Wedge CVP Or Hypovolemic Cardiogenic Or Or Obstructive Or Or Or Distributive Septic: Early Or or Septic: Late Recognition and Classification Initial Management of Shock Final Thoughts Recognize compensated shock quickly- have a high index of suspicion, remember tachycardia is an early sign. Hypotension is late and ominous. Gain access quickly- if necessary use an intraoseous line. Fluid, fluid, fluid - Administer adequate amounts of fluid rapidly. Remember ongoing losses. Correct electrolytes and glucose problems quickly. If the patient is not responding the way you think he should, broaden your differential, think about different types of shock. References, Recommended Reading, and Acknowledgments Uptodate: Initial Management of Shock in Pediatric patients Nelson’s Textbook of Pediatrics Some slides based on works by Dr. Lou DeNicola and Dr. Linda Siegel for PedsCCM American Heart Association PALS guidelines