Barriers to Health Care Access in the Latino Community: Communication,

Barriers to Health Care Access in the
Latino Community: Communication,
Satisfaction and Adherence
J. Emilio Carrillo, M.D., M.P.H.
Montefiore Medical Center
August 2, 2005
►
Poor health outcomes and disparities are a result of multiple socioeconomic, demographic, environmental and other social and cultural factors
►
Barriers to healthcare access are a significant contributor to poor health outcomes and disparities
Barriers to healthcare access contribute to
Latinos’ poor health outcomes and disparities:
Primary Access Barriers
Health Insurance
Lack of insurance, underinsurance, and inability to pay for care or treatments
Secondary Access Barriers
Organizational and systems of care
All barriers encountered between home and providers’ office: availability of care, transportation, childcare, waiting times, etc.
Tertiary Access Barriers:
Communication between Provider and Patient
When language and culture hinder the provider-patient communication
Primary
Access
Barriers
Race/Eth
Non-
Hisp.Wht.
Blacks
Hispanics
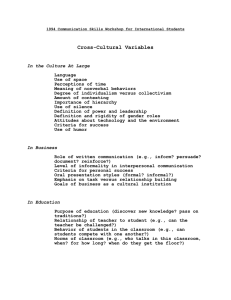
Trends in number of Hispanics without
Coverage
1989 1999 Change in Number uninsured
1989-1999
(thousands)
% Increase in
Unisured
19,190 21,370 2,180
5,840 7,240 1,410
6,930 10,950 4,020
+11%
+24%
+58%
Hispanics who make up 11% of the US population in 1999 accounted for 50% of the increase in the uninsured from 89-99
Source: Carrasquillo O. et al, Am J Pub Health 1999, 2000 CPS data
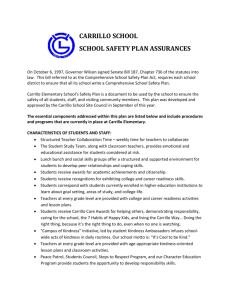
Health insurance among Latino/Caribbean Immigrants
Country
(N=number of immigrants)
Cuba (N=950,000)
% with Private
Health Insurance
% With Gov.
Insurance
% Uninsured
48% 35% 25%
Domin. Republic
(N=700,000)
El Salvador (N=750,000 )
Guatemala (N=350,000)
Haiti (N=400,000)
Mexico (N=7,850,000)
32%
36%
38%
60%
35%
33%
8%
13%
10%
14%
38%
58%
50%
37%
53%
Secondary
Access
Barriers
The Problem
►
Patients at risk who access the health care system face organizational and structural barriers to care
Organizational->leadership/workforce
Structural->systems of care
►
Results: decreased medical screening, later stage of presentation, and insufficient treatment
Organizational Barriers:
Leadership and Workforce
Research supports important role of minority representation in leadership and workforce
Minority providers:
► care for more minority and underserved patients
► are preferred
► score higher on patient-rated quality and satisfaction
Latinos are underrepresented:
► on health professional school faculty
► in city/county public health positions
► in the health professional workforce
Leadership
%Minority
Professional
Representation
Workforce
%Latino
4
3
2
1
0
6
5
Source: BHP
6
Physicians
17
12
10
8
6
4
2
0
18
16
14
3
Med S chool
Faculty
16
Pub Health
Faculty
City/County
Health Officials
5
Dentists
2.9
3.8
Pharmacists Optometrists
3.2
Nurses
Structural Barriers
►
►
►
►
►
►
►
Extramural
Door-->Clinic
Availability of providers
Proximity of Healthcare facilities
(HCF)
Operating hours of HCF
Transportation to HCF
Telephone access to providers
Knowledge of available resources
Lack of child care resources
►
►
►
►
►
►
►
Intramural
Clinic-->Doctor Office
Bureaucratic intake procedures
Long waiting time for appointments
Lack of interpreter services
Difficult referrals to test and specialists
Language-appropriate signage
Language-appropriate health education
Poor continuity of care
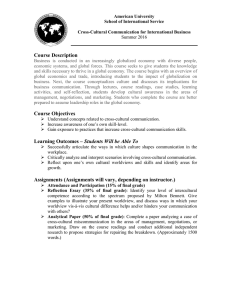
Structural Barriers:
Extramural and Intramural
►
Extramural
Patients at risk disproportionately reside in MUA and
HPSA, have little choice where to go for care, and use ER’s and OPD’s as main source
►
Intramural
Patients at risk face bureaucratic intake processes, long waiting times, limited access to specialists, less continuity of care, and significant language barriers in health care facilities
15
%Reporting
10
25
20
Structural
Barriers
%Reporting
50
45
40
35
30
25
20
15
10
5
0
0
5
22
16
8
Latinos Blacks Whites
Difficulty Accessing Specialists
46
39
26
Latinos Blacks Whites
Don’t have a regular doctor
Source: Commonwealth Fund
Tertiary
Access
Barriers
What are tertiary barriers?
►
Rooted in the provider-patient interaction
►
Sociocultural differences barriers to effective care due to:
poor communication
different beliefs about illness and treatment
poor adherence to therapeutic plan
limited health education
provider bias and stereotypes
Major Considerations
►
Heterogeneity of Patients at risk population
►
Acculturation, SES
►
Risk of stereotyping
►
Tertiary barriers less concrete
►
Address provider/patient perspectives
Primary, Secondary and Tertiary access barriers impact on Latinos’ health through various intermediary factors:
A. Less screening and preventive care
B. Late presentation to healthcare
C. Less treatment or no treatment
Intermediary Factors
Associated with Disparities
1 o
, 2 o
, 3
Access
Barriers o
* Evidence Based
*
A.
Screening
B. Late
Presentation
To Care
C. No Rx or Rx
*
POOR
HEALTH
OUTCOMES
A
R
I
T
D
I
S
P
I
E
S
What is Patient Based
Cross-Cultural Care?
Patient Based Cross-Cultural Care is a dynamic process of care which focuses on the unique social and cultural characteristics of the patient and provides skills to facilitate communication across social and cultural boundaries.
(Carrillo, ‘04)
EVERY INDIVIDUAL IS UNIQUE
Cultural
Unique
Individual
Social
Constitutional
(Carrillo, Green, Betancourt ‘99)
D
Disease vs. Illness
I
(Carrillo, Green, Betancourt ‘99)
How do we provide Patient Based
Cross-Cultural Care ?
1.
Language interpretation and translation
2.
Avoid cultural categorization
3.
Identify and address areas of cross-cultural sensitivity
4.Serve the individual
–
–
–
–
Be aware of you own personal perspective
Explore the patient’s perspective
Explore the patient’s expectations
Engage the patient, Earn the trust
(Carrillo, ‘04)
How do we provide Patient Based
Cross-Cultural Care ?
1.
Language interpretation and translation
2.
Avoid cultural categorization
3.
Identify and address areas of cross-cultural sensitivity
4.Serve the individual
–
–
–
–
Be aware of you own personal perspective
Explore the patient’s perspective
Explore the patient’s expectations
Engage the patient, Earn the trust
(Carrillo, ‘04)
What is Culture?
Shared system of values, beliefs, and learned patterns of behavior
Not equivalent to ethnicity or race
Dynamic, not static
(Carrillo, Green,
Betancourt ‘99)
Carlos Gutiérrez,
United States Secretary of Commerce
Cameron Diaz, Actress
How do we provide Patient Based
Cross-Cultural Care ?
1.
Language interpretation and translation
2.
Avoid cultural categorization
3.
Identify and address areas of cross-cultural sensitivity
4.Serve the individual
–
–
–
–
Be aware of you own personal perspective
Explore the patient’s perspective
Explore the patient’s expectations
Engage the patient, Earn the trust
(Carrillo, ‘04)
Identify and address areas of cross-cultural sensitivity
•
Every culture has areas of sensitivity
•
Sometimes sensitivities clash in the crosscultural encounter
–
–
Patients
Staff
•
Be alert to these sensitive areas
(Carrillo, Green,
Betancourt ‘99)
What are some of these sensitive areas?
•
•
•
•
•
Styles of communication
–
Informality may be seen as disrespect
–
–
Eye contact
Touch
Who’s in charge?
Gender of professional
Mistrust and Prejudice
Food preferences
(Carrillo, Green,
Betancourt ‘99
Curiosity
How do you know?
SIMPLY ASK!
Respect
Empathy
(Carrillo, Green,
Betancourt ‘99)
How do we provide Patient Based
Cross-Cultural Care ?
1.
Language interpretation and translation
2.
Avoid cultural categorization
3.
Identify and address areas of cross-cultural sensitivity
4.Serve the individual
–
–
–
–
Be aware of you own personal perspective
Explore the patient’s perspective
Explore the patient’s expectations
Engage the patient, Earn the trust
(Carrillo, ‘04)
Explore the patient’s perspective
•
What does the illness or the symptoms mean to the patient?
(Carrillo, ‘04)
Picture….
Why is it important to explore the meaning of the illness?
To facilitate diagnosis
To enhance patient satisfaction
address patients’ expectations, fears
earn patient’s trust
strengthen doctor-patient relationship
To promote adherence to therapeutic plan
Explore the patient’s expectations
•
What does the patient expect?
•
Patient’s social context
(Carrillo, ‘04)
Explore the patient’s expectations
•
What is at stake for the patient?
(Carrillo, ‘04)
►
45 year old Puerto Rican woman lives in East Harlem, “El Barrio,” depressed, adhering poorly to DM and BP medications. Major concern is obtaining Public Housing.
Engage the patient, Earn the trust
•
Acknowledge
•
Explain
•
Negotiate
(Carrillo, ‘04)
How do we provide Patient Based
Cross-Cultural Care?
Language
Patient’s
Sensitivities
• Identify Sensitive
Areas
• Simply Ask
Recognize Our
Personal
Perspective
Patient’s
Perspectives
• What does it mean?
• What is expected?
• What is at stake?
Engage the patient,
Earn the trust
• Acknowledge
• Explain
• Negotiate
(Carrillo, ‘04)
PATIENT BASED CROSS-CULTURAL
COMMUNICATION CAN SERVE AS AN
ADJUNCT TO TREATMENT ADHERENCE
EFFORTS
Screening for Adherence Risk
Didactic Acronym
M eaning Concordance
A pprehension and concern about treatment
P layback of negotiated treatment plan
S ocial barriers to treatment adherence
(Carrillo, ‘04)
• What’s wrong?
• What will happen?
• What can I do?
Patient
Negotiate
Mutual Accord
M. A. P. S.
Provider
• What do you think is going on?
• What do you expect?
• What’s at stake?
Acknowledge
Present Bio-Med Model
(Syntonic)
Satisfaction
Adherence
(Carrillo, ‘04)