Care Homes' Use of Medicines Study (CHUMS) - Identifying and preventing medication errors in care homes (ppt, 1,582 KB)
advertisement
 - Identifying and preventing medication errors in care homes (ppt, 1,582 KB)")
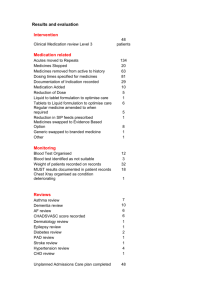
Dr David Alldred Lecturer in Pharmacy Academic Unit of Medicines Management University of Leeds d.p.alldred@leeds.ac.uk Background Patient safety initiatives of early 2000’s supplemented by DH policy research initiative: Patient Safety Research Portfolio at: http://www.pcpoh.bham.ac.uk/publichealth/psrp Commissioned research on medication errors in care homes. Care Homes’ Use of Medicines Study •Prof Nick Barber (University of London) •Prof Theo Raynor (University of Leeds) •Prof Peter Buckle (University of Surrey) www.pharmacy.ac.uk Care homes’ use of medicines study (CHUMS) Aims 1. To identify the frequency and causes of medication errors (prescribing, monitoring, dispensing, administration) 2. To determine the potential harm 3. To suggest solutions (Alldred et al 2009; Barber et al 2009) Methods 256 randomly selected residents from 55 homes in W Yorks, Cambs and London (38 mixed care) Visited homes: observed staff/records observed medicines observed administrations (2 drug rounds/resident) interviewed care home staff. Results Mean age 85, on mean of 8 meds 7 out of 10 residents were exposed to at least one medication error (mean of 1.9 errors/resident) Prevalence of prescribing errors 8.3% of medicines (39% of residents) Monitoring errors 14.7% of medicines (18% of residents) Dispensing errors 9.8% of medicines (37% of residents) Administration errors 8.4% (22% of residents) Administration errors Prevalence of 8.4% (1 in 12) Half were omissions, one-fifth wrong dose Residential > Nursing? (adjusted OR 1.77 95% CI 0.96 to 3.25) Types of administration errors Omission Drug incorrect Allergy error Formulation error Extra dose(s) Route error Wrong dose Deteriorated drug Unprescribed drug Timing error Omission: Fluoxetine 20mg capsules were prescribed “one daily” for depression and not administered for 6 days as drug not in stock. Wrong dose: Casodex® (bicalutamide) 150mg tablets “one daily” were prescribed by the hospital for prostate cancer; the prescription was continued by the GP generically as bicalutamide and administered simultaneously. Wrong dose: Glyceryl trinitrate patch prescribed generically “5mg/24 hours take HALF daily” for ischaemic heart disease. A patch was cut in half and applied to the resident’s chest despite the fact that the contents were leaking out. Formulation and dispensing systems Compared different formulations to see if any difference in error rates Monitored dosage systems versus manufacturers’ packaging (Alldred et al 2011) Formulation and dispensing systems When compared to tablets/capsules in MDS, error rates were: Liquids – 4 times higher Omissions Not shaking bottle Inaccurate measurement (Alldred et al 2011) Formulation and dispensing systems When compared to tablets/capsules in MDS, error rates were: Topical/transdermal/injections – 19 times higher Omissions Wrong doses Expired (Alldred et al 2011) Formulation and dispensing systems When compared to tablets/capsules in MDS, error rates were: Inhalers – 30 times higher Not shaking device Resident not holding breath Spacer not used Wrong number of puffs (Alldred et al 2011) Formulation and dispensing systems When compared to tablets/capsules in MDS, error rates were: Tablet/capsules not in MDS – twice as high (Alldred et al 2011) Drug sensitivities Record review of 121 residents in 31 homes 31 (26%) had ≥1 documented sensitivity 48 sensitivities in total Number of sensitivities recorded by: GP Care home records Medicines administration record 35 (73%) 29 (60%) 3 (6%) Only 2 sensitivities documented on all three records (Alldred et al 2010) Recording of drug sensitivities Causes of errors (CHUMS) Human error theory Systems approach 59 interviews with staff who made errors Multiple causes Accident Causation Model ORGANISATIONAL & CORPORATE CULTURE CONTRIBUTORY FACTORS INFLUENCING PRACTICE Work/ Environment Factors Management Decisions and Organisational Processes DEFENCES/ BARRIERS Unsafe Acts Team Factors Individual (staff) Factors Errors Incident Task Factors Patient Factors LATENT FAILURES CARE MANAGEMENT PROBLEMS ERROR & VIOLATION PRODUCING CONDITIONS Violations ACTIVE FAILURES Causes of errors (CHUMS) Lack of patient awareness of medicines Physical problems e.g. dysphagia, arthritis Dispensing and ordering systems Lack of protocols Lack of knowledge and training Tired, unwell, stressed etc. Verbal rather than written culture Causes of errors (CHUMS) Time pressure Staff turnover Drug round interruptions (up to 12 per hour) Poor communication with pharmacy and GP Lack of support from other healthcare professionals Inaccurate medicines administration records Physical environment –unpleasant smells, poorly lit, noisy, shortage of space Solutions Improve/increase education and training Drug round breaks Redesign the drug trolley Reduce number of medicines/doses Prescribe medicines more evenly over the day Improve communication with, and support from, other healthcare professionals Adequate policies Technology e.g. barcoding, ordering systems Summary Prevalence of administration errors is high and needs reducing Medicine-related and patient-related factors may increase the risk of error Causes are multiple Solutions need to be developed to improve systems Technology has a role References Alldred et al 2011. The influence of formulation and medicine delivery system on medication administration errors in care homes for older people. BMJ Qual Saf DOI: 10.1136/bmjqs.2010.046318 Alldred et al 2010. The recording of drug sensitivities for older people living in care homes. Br J Clin Pharmacol 69:553-557 Alldred DP et al 2009. Care home use of medicines study. Medication errors in nursing and residential care homes – prevalence, consequences, causes and solutions. Report to the Patient Safety Research Portfolio. Available at http://www.haps.bham.ac.uk/publichealth/psrp/PS025_Project_Summary.shtml Barber ND et al 2009. The Care Homes’ Use of Medicines Study: prevalence, causes and potential harm of medication errors in care homes for older people. Qual Saf Health Care 18, pp.341-6. Available at http://qshc.bmj.com/content/18/5/341.abstract Dean B, Barber N. 2001. Validity and reliability of observational methods for studying medication administration errors. Am J Health System Pharm 58:54–9.