Lett. Drug Design Discov. 1 237-246 (2004).doc
advertisement
.doc")
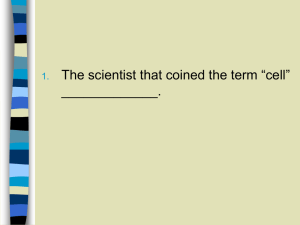
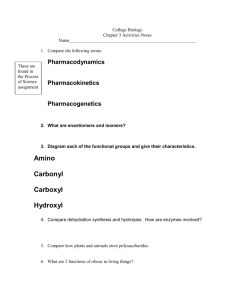
Proteomics to identify novel biomarkers and therapeutic targets in cardiovascular disease Markus Kubicek, Silvia M. Sanz-González, Francisco Verdeguer and Vicente Andrés* Laboratory of Vascular Biology, Department of Molecular and Cellular Pathology and Therapy, Instituto de Biomedicina de Valencia-CSIC, 46010 Valencia, Spain * Correspondence: Vicente Andrés Instituto de Biomedicina de Valencia Consejo Superior de Investigaciones Científicas C/Jaime Roig 11, 46010 Valencia (Spain) Tel: +34-96-3391752 FAX: +34-96-3690800 e-mail: vandres@ibv.csic.es KEY WORDS: Proteomics, Protein modification, Two-dimensional electrophoresis, Mass spectrometry, Cardiovascular disease. 1 Abstract The proteome is described as the entirety of all proteins expressed within a cell at a given moment. In contrast to the stability of the genome, the proteome is highly dynamic and reflects the cell’s current status. Since proteins carry out almost all biological functions, the proteome stands in direct relation to cellular functions. Proteomic analysis (i.e., two-dimensional electrophoresis, mass spectrometry and bioinformatics) aims at identifying changes in the composition of the proteome associated to pathophysiologic events that affect basic cellular functions. Functional proteomics expands to understanding the connection between proteomic changes and the state of a cell, taken into account that the observed modifications can be either cause or consequence of the pathological state. Proteomics will not only improve our basic understanding of the factors and molecular mechanisms underlying cardiovascular disease, but also will help identifying novel diagnostic markers and fuel the rational design and discovery of new drugs for medical intervention. This review will discuss basic proteomic approaches relevant to cardiovascular disease, as well as their applications for the identification of biomarkers and drug design. 2 Outline 1. Potential of proteomic studies in disease research 2. Methodological aspects of proteomic analysis 2.1. Two-dimensional separation of proteins 2.2. Protein visualization and image analysis 2.3. Protein identification by mass spectrometry (MS) 2.4. Recent developments in proteomic technology 3. Applications of proteomics to the pathobiology of the cardiovascular system 3.1. Cardiovascular proteomic databases 3.2. Proteomic studies in cultured cells 3.3. Proteomic studies in animal models of cardiovascular disease 3.3.1. Non transgenic models 3.3.2. Transgenic mouse models 3.4. Proteomic studies relevant to human cardiovascular disease 3.4.1. Proteomic analysis of human arterial tissue 3.4.2. Proteomic analysis of human cardiac tissue 4. Concluding remarks 5. Acknowledgements 6. References 1. Potential of proteomic studies in disease research The genetic information stored in a cell’s nucleus (the genome) is undoubtedly the underlying factor determining cellular phenotype. Nevertheless, despite the impact of genomics in molecular biology and medicine, the genome should not be seen as more than a rough outline of a cell’s body plan. Although a certain percentage of diseases have been linked to genetic changes, the majority of pathological disorders are associated with protein alterations. Since proteins not only carry out almost all bio-enzymatic functions, but they also respond to and integrate extra- and intracellular changes, it comes as no surprise that proteins serve as the main drug targets and biological disease markers. Thus, understanding proteomic changes in pathological situations will help to decipher the molecular basis of disease and to elucidate the relevant protein components, pathways and regulations. In terms of genome size, humans are not so much superior to nematodes. So in order to understand what makes up the complexity we inherit we have to look somewhere else than solely at the genome. DNA is a rather rigid molecule that serves as a template for the expression of mRNA and proteins. Ultimately, it is mainly the entirety of expressed proteins (the proteome) what accounts for the functional flexibility and complexity of the human body. Different mechanisms contribute to phenotypic diversity (Fig. 1). First, transcription of a single gene can give rise to different messenger RNAs (mRNAs) through utilization of alternative transcription initiation sites and alternative splicing [1]. Specific mRNAs display highly different half-lives depending in part on their sequence determinants, but also on the state of the cell. Still, the correlation between mRNA abundance and the abundance of the corresponding protein has been found to be quite low [2]. This discrepancy may arise 3 mainly from protein degradation, which is highly specific and subjected to cellular regulation. Additional complexity arises because protein function depends on the right folding (secondary and tertiary structure), on their interaction with other biomolecules (quaternary structure), and on reversible post-translational modifications [3]. To date, more than 200 different protein modifications have been described [4], amongst them phosphorylation, methylation, glycosilation, prenylation, and sulfatation. In addition, subcellular localization and compartmentalization greatly affects protein function. For example, a number of proteins exert distinct functions in different microcellular compartments. Finally, most proteins operate as parts of large protein complexes or networks. These networks themselves are highly interconnected in complex networks that are capable of sensing and reacting to intra- and extracellular changes. Although genomic analysis provides important information towards susceptibility to acquire a certain disease, it is equally important to elucidate proteomic changes induced by environmental factors which determine disease severity and prognosis (for example in cardiovascular disease or cancer). Therefore, disease proteomics will allow us to define the pathological state of a cell or a tissue. From this information we will be able to derive the molecular mechanisms of the disorder, putative medical intervention targets and diagnostic markers. Proteomics encompasses a growing set of different techniques aimed at functionally describing the whole proteome of a cell or a tissue in a given moment under specific conditions. Protein components of pathological relevance may be identified by comparing the proteome of patients and unaffected individuals. Consequently, the relevant questions we have to answer in order to ascertain the pathological relevance of a candidate protein include the following: i) when, where and to what level is the protein expressed during disease development, and what are the types of modifications it is subjected to; ii) what is the function of the protein and how is that function modulated during disease progression; iii) is the candidate protein involved in protein-protein interactions, and what can we learn from these interactions about the molecular mechanism of the pathologic process; iv) can functional information be derived from the structure of the protein and how is this linked to the pathology; and v) can the acquired information be used for diagnostic purpose and/or for the design of therapeutic agents. 2. Methodological aspects of proteomic analysis 2.1. Two-dimensional separation of proteins Proteomic technology still is in its infancy days, but methodological advances have made possible to attack the task of analyzing the whole proteome of a clinical sample, an ambitious project given the enormous number of expressed proteins and the diversity in potential post-translational modifications they can undergo. Most proteomic studies aimed at elucidating disease-dependent proteome alterations have so far taken advantage of two-dimensional polyacrylamide gel electrophoresis (2D-PAGE) [5] (Fig. 2). The first dimension (isoelectric focusing) is carried out using gels with a fixed pH gradient to separate proteins according to their isoelectric point (pI). Subsequently, the proteins are resolved according to their relative masses in a second dimension by SDS-PAGE. After completion, protein spots are visualized and subjected to mass spectrometry (MS) in order to determine their identity [6]. Despite certain limitations, proteomics has provided useful information on disease related changes in protein expression as we discuss below. 4 In order to obtain the profile of protein expression in disease, proteins have to be extracted from complex biological samples such as cell populations, tissues, or biological fluids. Sample acquisition and preparation is the first and very often most critical step in 2D-PAGE. Biological fluids such as whole serum or plasma are relatively easily accessible, however protocols for sample collection are not usually ideally suited for proteomics due to possible protein degradation or modifications during handling. The use of serum is complicated by the high abundance of albumin that interferes with 2D-PAGE. This problem can be overcome by prefractionating the sample. For example, Zuo et al. described a system that allowed sample prefractionation into a few welldefined pools using microscale solution isoelectric focusing (nusol-IEF) prior to 2D-PAGE [7]. At least 6- to 30fold higher protein loads were possible for nonalbumin fractions on narrow pH range IPG gels. This method substantially increases the dynamic range of protein detection since higher protein loads can be applied to narrow pH range 2D-PAGE gels. Whole tissue analysis from human patients is often required in proteomics. Tissue heterogeneity may further complicate the analysis of clinical samples obtained by biopsy. Tissue microdissection techniques, especially laser-capture microdissection, allow the isolation of defined cell types from whole tissue. These approaches greatly reduce tissue heterogeneity, however the amount of protein retrieved maybe insuficient for 2D-PAGE analysis [8]. Lymphocytes and mononuclear cells can be easily isolated from whole peripheral blood by differential centrifugation. Tissue recovery of cells can be circumvented by analyzing cultures of primary or immortalized cell lines, an approach that has been widely used in proteomic research because yields high amounts of protein and experimental variables can be tightly controlled. Although treatment of cultured cells with agents that mimic, at least in part, the pathogenic process of interest may shed significant insight into disease-related intracellular changes, it is noteworthy that the results obtained from cultured cells may not accurately reflect the situation in the living tissue/organism. Regardless of their source, proteins need to be extracted using a solubilization protocol that it is suitable for isoelectric focusing. Extraction is accomplished using a chemical cocktail that has to be optimized for every different sample. Still, a single buffer will not solubilize all the proteins contained in the sample due to their chemical and physical heterogeneity (i. e., differences in hydrophobicity, a high range of molecular sizes, etc). This problem can be solved if differentially extracted portions of the sample are analyzed individually. An intrinsic limitation of gel-based proteomic techniques is that highly abundant proteins are preferentially displayed. One approach to overcome this challenge is to reduce sample complexity by analyzing protein subsets rather than whole cell extracts. The removal of highly abundant constitutive proteins may help detect lowabundance proteins that may be pathologically relevant. In addition, subcellular fractionation allows the identification of interesting proteins that only exist in certain organelles and may not be visualized in whole cell lysates. Moreover, “organelle proteomics” allows searching for protein changes in compartments that are of special pathological interest. For example, surface membrane proteins currently comprise a large fraction of the therapeutic targets and diagnostic markers due to their key role in disease development (i.e., cancer invasiveness and inflammatory infiltration in atherosclerotic plaques). Of note in this regard, proteins with extracellular domains can be biotinylated and easily extracted by affinity-purification [9]. 2.2. Protein visualization and image analysis In order to compare proteomic profiles between pathological and normal control samples, proteins separated by 2D-PAGE must be visualized by in-gel protein staining protocols. Despite its relatively low 5 sensitivity, Coomassie Brilliant Blue (CBB) R-250 is the most conventional approach for protein staining. However, quantification of protein amount is problematic since proteins may be visualized to a different extent during destaining. Colloidal CBB G-250 has circumvented this problem by allowing background-free detection of proteins at a sub-microgram level [10]. Silver staining protocols are at least hundred times more sensitive than CBB-based techniques [11], but inherent oxidative modification of the stained proteins makes it incompatible with MS [12]. Recently, commercially available MS-compatible silver staining kits have successfully been applied in proteomics [13]. Like silver staining, fluorescent methods allow for the visualization of a larger number of proteins, which is especially crucial for samples available in limited amounts [12]. Fluorescent staining of proteins combines high sensitivity and compatibility with downstream analysis and additionally allows staining of proteins that are hardly stained by alternative methods (like glycoproteins, lipoproteins, low molecular mass proteins and metalloproteases). In addition, alterations between the disease and the control profiles can be easily detected using differential in-gel electrophoresis (DIGE), in which the two samples are labeled with different fluorescent dyes and analyzed in the same two-dimensional gel [13]. Conventionally, pattern comparison between pathological and control samples requires gel scanning and “software-supported” analysis. Nevertheless, improvement in software for automated spot comparisons is desirable. 2.3. Protein identification by mass spectrometry (MS) The identity of spots exhibiting different patterns between control and pathological specimens is usually assessed by MS “fingerprinting” [15]. This technique analyzes the mass-to-charge ratio (m/z) of peptide fragments produced by proteolytic cleavage with specific proteases (i. e., trypsin, chymotrypsin). Every protein digested with a specific enzyme will give rise to a unique mass spectrum that can be compared against a hypothetical genome-derived peptide-mass database. Because MS is a highly sensitive technique, special care must be taken to prevent sample contamination. In order to be subjected to MS, the spot of interest has to be excised from the gel and treated with the desired protease. The resulting peptide mixture is volatilized and ionized by matrix-associated laser desortion (MALDI) or electrospray ionization (ESI) [6]. The real mass analyzer is usually time of flight (TOF) if coupled to MALDI, or ion trap and quadrouple if ESI is used. In either case, peptides are separated according to their specific m/z plotted against peak intensities. Computer comparison to databases will give rise to hit lists, which are the typical informational outputs of proteomic experiments. In some cases, however, protein identity maybe uncertain due to high background levels or impurities (spots separated by two-dimensional electrophoresis often contain several proteins). In either case, the peptides can be further defragmented, producing smaller sized charged fragments that are re-analyzed in a collision induced (CID) mass spectrometer [16]. In principle, CID results in a peak pattern that also contains information about the peptide sequence. In this way proteins are identified accurately and additional information on the localization and identity of post-translational modifications can be gathered. Additional information on the equipment and techniques used to analyze peptide sequence by fragmentation is provided by Aebersold and Mann [6]. 2.4. Recent developments in proteomic technology Despite recent improvements, conventional two-dimensional MS-based analysis still holds some limitations, especially low throughput and the need of a relatively large amount of sample. Both of these problems are quite inconvenient for disease proteomics, where large-scale assays are desired. Several strategies have been developed in order to enhance sample automation. For example, direct scanning of 2D-PAGE or 6 trypsin containing membranes by MALDI–MS have been reported [17]. Moreover, gel-free approaches using liquid chromatography (LC) [18] or capillary electrophoresis [19] to achieve protein separation prior to MS have been developed, thus circumventing the tedious task of 2D-PAGE. Protein samples can be separated by coupling two different HPLC columns in tandem and connecting them directly to a mass spectrometer. Usually, proteins in the first chromatography are retained according to their charge using an ion exchange column. Then, in a coupled reverse phase column, proteins are further separated according to their hydrophobicity [20]. Although protein mixtures can be analyzed this way, enzymatic digestion of the sample prior to chromatography is more convenient. In this approach a thousand of different peptides are separated by the HPLC that can readily be analyzed by MS. Because subpicomolar amounts of sample are sufficient, peptides derived from low abundant proteins that usually are not detectable by gel-based methods can be identified using this approach. Moreover, the serial setup of tandem HPLC connected directly to the MS analyzer allows for high throughput automation. Isotope code affinity tagging (ICAT) of proteins further increases detection sensitivity for low abundance proteins analyzed by gel-free proteomics [14]. By using different tags, one of natural abundance and the other isotopically labeled, quantitative differences in protein abundance between two different samples can be readily detected. The proteome is first digested and the resulting peptides are purified and subjected to LC-ESI. Imaging MS has been recently developed to perform in situ proteomic analysis of whole tissues without the need of previous protein separation [21]. In this technique, frozen tissue sections are directly applied to MALDI-MS analysis in a regular spatial manner to directly obtain mass profiles across the tissue section. Following the success of DNA microarray chips, protein microarrays are being developed for protein profiling and medical diagnostics [22-24]. Protein chips contain defined sets of proteins arrayed at high density onto glass slides. Some approaches use peptides [25] or whole proteins encoded by libraries which are coated onto the chip in order to screen for interacting molecules, or to carry out functional screens. Recently, reverse phase protein arrays have been described that immobilize the whole protein content of a tissue on an array [26] to screen for protein modifications or in search for autoimmune disorders [27]. Ziauddin et al. have reported the generation of protein microarrays whose features are clusters of live cells that express a defined cDNA at each location [28]. Protein array techniques are especially appropriate for understanding drug intervention and for finetuning of drug design. For instance, screening a protein array against low molecular weight drug inhibitors may yield significant insight into both drug targets as well as the drug’s mode-of-action. Protein arrays are also suitable to test the affinity of new drug derivatives. One example of such use is a recent study on FKBP12 binding to different small molecules in yeast [24]. Another useful application of protein chips is the screening for specific enzymatic activities. Protein kinases are of high interest in drug intervention due to their key regulatory role in biological signaling pathways. Zhu et al. have shown that many kinases remained active when immobilized on polydimethylsiloxan (PDMS) chips and showed genuine substrate specificity [22]. As an alternative to protein arrays, antibodies that will specifically recognize their respective antigen according to their abundance can be immobilized onto the microchip surface [23]. Such antibody arrays are suited for protein quantification (by using a second antibody against the bound protein), and for the detection of specific posttranslational modifications like phosphorylation. The main advantage of protein arrays is their capacity to simultaneously analyze a high number of proteins even among different cell and tissue types. Chips can be 7 combined with direct MALDI analysis for read-out, thereby generating a highly sensitive and high-throughput automated system. Major limitations in current protein chips are the generation of expressing clones for a whole proteome, the lack of post-translational modifications in bacterially expressed proteins, the short-term stability of some proteins on synthetic slides, and the difficulties in printing homogeneous spots. Moreover, the shortness of highly specific antibodies limits the use of antibody arrays. Nevertheless, protein chip automation is a rapidly evolving technique with a huge potential in molecular medicine. Better and more efficient methods of quantification need to be developed before protein microarrays will become a standard method for clinical applications. 3. Applications of proteomics to the pathobiology of the cardiovascular system 3.1. Cardiovascular proteomic databases Databases of cardiac proteins have been generated from human [29-35], dog [35,36], rat [35,37], and bovine [38] tissue. The uniform resource location (URL) of some of these databases is given in Table 1. Proteomic analysis of pathological samples can be directly compared to these databases instead of, or in addition to, their comparison to experimental control samples. In fact, a large number of proteins extracted from dog, rat and mouse cardiac tissue has been successfully identified by direct comparison against a human heart protein database [39]. This provides a useful shortcut in the rough analysis of proteins of specific tissues from different species, although confirmation of these data will be required. 3.2. Proteomic studies in cultured cells Several studies have been carried out in primary cultures of cells that are relevant to cardiovascular disease, including smooth muscle cells (SMCs), endothelial cells (ECs), foam cells (Table 2), and cardiomyocytes (Table 3). Cultured cells can be analyzed under multiple conditions and pathophysiological stimuli. For instance, significant differences in the expression of certain proteins have been reported in proliferating versus nonproliferating primary rabbit SMCs [40]. Likewise, LC-MS/MS analysis of quiescent human umbilical vein ECs (HUVECs) has allowed the identification of 53 proteins involved in several processes, including cytoskeletal organization, cellular motility and plasticity, control of apoptosis and senescence, coagulation, and antigen presentation [41]. Since both hyperplastic and hypertrophic growth play a key role in cardiovascular disease, Patton et al. investigated alterations in the proteome of rat aortic SMCs stimulated with different growth factors (FCS, PDGF and angiotensin II) [42]. Compared to unstimulated cells, several proteins could be identified that underwent growth factor-dependent upregulation (i. e., heat shock proteins hsp60 and hsp70, protein disulfide isomerase, vimentin, actin, EF-1, and calreticulin) and downregulation (i. e., myosin heavy chain). The authors concluded that hyperplastic and hypertrophic growth processes are accompanied by similar changes in protein expression. Nichols et al. studied the effect of glucocorticoids on the proteome of cultured bovine aortic ECs, rat SMCs (synthetic- and contractile-state), and rat cardiac muscle and non-muscle cells [43,44]. They observed direct effects of glucocorticoids on ECs that may be clinically relevant in the setting of cardiovascular disease. 8 They also identified an overlapping, but not identical, set of proteins of the so-called glucocorticoid domain that are induced by glucocorticoids in the various cell lines analyzed. Changes in the proteome during foam cell formation have been investigated using an in vitro model consisting of exposure of U937 cells to oxidized LDL (oxLDL) [45]. oxLDL-regulated factors included 28 upregulated and 9 downregulated proteins. Moreover, 11 proteins were exclusively detected in foam cell cultures, whereas 8 proteins detected in control U937 cultures were absent in foam cells. Treatment of rabbit ventricular myocytes with adenosine at a concentration sufficient to mimic pharmacological preconditioning has revealed two novel phosphorylation sites in myosin light chain 1 (MLC1), both of which are highly conserved in rats and humans [46]. Likewise, treatment of cardiac myocytes with the hypertrophic agent phenylephrine resulted in changes in MLC, as well as in mitochondrial proteins, hsp27 and several chaperone cofactors [47]. The effect of blood flow in plaque development has been investigated in a 2D-PAGE study using bovine aortic ECs subjected in vitro to different flows [48]. The gelsolin family member CapG was undetectable under pro-atherogenic (oscillating) flow conditions, whereas its level of expression was upregulated under nonatherogenic (unidirectional) flow, in agreement with the protective function of CapG against atheroma development. In addition to environmental influences, age is a relevant factor in the pathogenesis of cardiovascular disorders. Proteome comparison of cultured aortic SMCs that had been obtained from either newborn or aged rats detected 14 differentially expressed proteins, 4 in newborn and 10 in older animals [49]. One of the protein specific for old aortic SMCs has been identified as cellular retinol-binding protein. 3.3. Proteomic studies in animal models of cardiovascular disease 3.3.1. Non transgenic models Using a bovine model of hereditary dilated cardiomyopathy (DCM), Weekes et al. separated over 1125 proteins from ventricular tissue. Amongst these, 24 were found decreased and 11 increased in pathological versus control tissue, but only 12 have been successfully identified [38]. The authors concluded that inappropriate protein ubiquitination plays a major role in DCM. Rapid ventricular pacing in dogs results in a heart failure condition that closely resembles human and canine DCM. Proteomic analysis of control versus paced myocardial samples indicated that the development of heart failure in this model involves alterations in proteins involved in mitochondrial energy production, cytoskeletal architecture, and calcium-regulated processes [50,51]. Particularly, diminished expression of mitochondrial hydroxylmethyl glutaryl CoA synthase was observed, consistent with the hypothesis of reduced mitochondrial energy supply during DCM. Furthermore, glycolytic enzymes were detected in increased amounts, probably as a mechanism to counteract insufficient mitochondrial energy production. Several animal studies have investigated changes in the protein profile in the myocardium following ischemia-reperfusion injury. Sakai et al identified rat myocardial proteins altered upon ischemia by using fluorescence-based 2D-PAGE [52]. Likewise, Schwertz et al. have also found marked differences in protein expression following myocardial ischemia-reperfusion in rabbits [53]. Additionally, the authors surveyed the effect of FUT-175, a complement inhibitor that can reduce the amount of necrosis in ischemic tissue, on ischemia-induced myocardial protein alterations. Specially, superoxide dismutase precursor and B-crystalline 9 were preserved by drug treatment. Importantly, this assay provides an interesting application for proteomics in order to discover therapeutic targets and to detect specific effects of pharmacological drugs. In order to gain insight into the regulation of heart function by different blood flow rates, myocardial tissue from distinct regions of the heart of beagle dogs has been subjected to 2D-PAGE [54]. As compared with high flow areas, tissue from low flow regions displayed reduced nitric oxide synthase inhibition, suggesting enhanced nitric oxide formation, a higher glycolytic and a lower fatty acid oxidation capacities. Chronic alcohol consumption accentuates the severity of acquired immunodeficiency syndrome (AIDS) and contributes to the development of cardiomyopathy. As concluded from proteomic alterations detected in an AIDS mouse model, Weekes et al. have suggested that alcohol consumption exacerbates the effects of retroviral infection on the heart by lowering the stress response, thus leading to de-protection and further cytotoxic effects [55]. Patel et al. reported proteome alterations in cardiac tissue from rats that had been chronically exposed to alcohol, including reduced expression of hsp60, hsp70 and desmin, whereas actin, vimentin, albumin, MLC1 and MLC2 did not change [56]. 3.3.2. Transgenic mouse models Transgenic mice have become an invaluable tool to further our understanding of cardiovascular disease. By analyzing serum from apolipoprotein E*3-Leiden transgenic mice, Skehel et al. have identified haptoglobin as a putative marker of early atherosclerosis [57]. The epsilon isoform of protein kinase C (PKC-) plays a critical role in protection against injury in multiple organs, including the heart. Using 2D-PAGE and affinity pull-down assays, Ping et al. have identified PKC--dependent signaling complexes in PKC- transgenic mice [58]. Furthermore, complementary separation techniques coupled to LC-MS/MS showed that these regulatory complexes include metabolism- and transcription/translation-related proteins [59]. 3.4. Proteomic studies relevant to human cardiovascular disease One important goal of proteomic analysis is to identify novel disease biomarkers, which can be used for diagnostic purposes and to monitor disease progression and the response to therapy. Because severe clinical manifestations of cardiovascular disease maybe prevented or limited by early medical intervention, identification of biomarkers associated to early pathological stages is especially crucial. Major cardiovascular risk factors (i. e., hyperlipidemia, hypertension, smoking, diabetes) are not markers of an existing pathological manifestation (like plaque formation), nor can disease progression be followed using these indirect blood markers. Moreover, early diagnostic of atherosclerosis is particularly difficult since disease manifestations like angina pectoris or thrombosis occur at late phases of the disease. Therefore, the identification of biomarkers of different stages of the disease will be of great significance. In the next section, we discuss proteomic studies of relevance for human cardiovascular disease. It is noteworthy that only four of these studies performed mRNA expression studies, two of them reporting a good correlation between protein and mRNA levels [48,54] and two reporting lack of correlation between these parameters [60,67]. Enhanced transcription may contribute to increased expression of a given protein if the corresponding mRNA is induced in a temporally appropriate manner under the same conditions. In contrast, post-transcriptional and/or post-translational mechanisms may operate when increased expression of a given protein is not paralleled by augmented mRNA steady-state level. Thus, it is desirable that mRNA expression studies are performed to shed light on the results of proteomic analysis. 10 3.4.1. Proteomic analysis of human arterial tissue Proteomic studies using human arterial tissue are summarized in Table 2. By examining human coronary artery tissue by proteomic analysis, You et al. found increased expression of ferritin light chain in coronary artery disease (CAD) patients when compared to unaffected individuals [60]. Augmented ferritin light chain expression is postulated to contribute to the pathogenesis of CAD by modulating the oxidation of lipids within the vessel wall through the generation of reactive oxygen species. In another study, Duran et al. examined the proteins secreted by cultures of arterial tissue obtained from atherosclerotic and non-atherosclerotic vessels [61]. Pathological arteries showed a much higher number of in vitro excreted proteins as revealed by 2D-PAGE. Obviously, additional studies are required to determine which of these proteins may be genuine biomarkers of atherosclerosis. Changes in the distribution of several cytoskeletal proteins, like vimentin, desmin and actin, have been described within the tunica media of atherosclerotic human arteries [62]. Because some of these alterations appear to depend on the stage of the lesion, they are candidate markers for early and advanced phases of atheroma formation. Similarly, protein alterations associated with the initial stages of human atherogenesis have been detected by comparing plaque-free aortic tissue, fatty streaks and fibro-fatty containing lesions [63,64]. Age is a major cardiovascular risk factor. Using a 2D-PAGE approach, Song et al have suggested that alterations in the proteome of atheroma-free aortic intima correlate with histological changes such as the intimal thickening often found with aging [65]. For instance, certain proteins detected in arteries from old individuals were rarely found in young individuals, such as 1-antichymotrypsin, haptoglobin -chain and immunoglobin G chains. Other proteins, such as albumin and -antitrypsin, were present in both groups, although their expression was augmented with age. 3.4.2. Proteomic analysis of human cardiac tissue The application of proteomics to heart disease is probably the most developed area of cardiovascular proteomics (Table 3). Pleissner et al. found a characteristic distribution of MLC by comparing human myocardium from left ventricular (LV) and right atrial (RA) samples obtained from end-stage, failing explanted versus healthy donor hearts [66]. In fact, expression of atrial MLC, but not -myosin heavy chain, is correlated in vivo with increased ventricular function in patients with hypertrophic obstructive cardiomyopathy [67]. Thiede et al. [68] have identified several DCM-associated post-translational modifications as well as differentially expressed proteins by using HPLC-separation coupled to MALDI-MS. Some alterations in cytoskeletal proteins associated with DCM have been found in humans, such as MLC1 [69]. In another study, 88 proteins displayed downregulation in cardiac tissue from DCM versus ischemic heart disease (IHD) patients, while 5 proteins were increased in the DCM group, with the most prominent changes occurring in the contractile protein MLC2 and in desmins [70]. Recently, Weekes et. al found in the heart of DCM patients a 2-fold and 5fold increase in protein ubiquitination relative to IHD and control hearts, respectively [71], in agreement with their previous studies in a bovine model [38]. Scheler et al. have investigated by 2D-PAGE the pattern of hsp27 in human myocardial tissue [72,73]. Their studies have demonstrated significant alterations in hsp27 pattern of expression when comparing normal and cardiomyopathic hearts (DCM and IHD), and suggest that some form of hsp27 degradation occurs during heart failure. 11 4. Concluding remarks Identification of proteome changes will fuel the establishment of novel diagnostic tests to assess an individual’s cardiovascular risk, such as the development of atherothrombosis or heart failure. It may as well become possible to monitor disease progression and the prognosis of cardiovascular patients by identifying stage-specific disease markers, and to direct therapeutic strategies to the overabundance, deficiency or altered function of a specific disease-related protein. Proteomics is also likely to facilitate both the development of new drugs as well as the design of drug derivates of superior effectiveness and reduced toxicity. In particular, proteomic chip technology may be employed in the fast and accurate screening of therapeutic agents by assessing both their specificity and potency towards the target protein. Undoubtedly, proteomics is a rapidly evolving methodology that holds great promise in cardiovascular research through the assessment of disease related alterations that are not predictable from genomic analysis. However, proteomics still awaits further advancements in order to satisfy the needs of effective disease diagnostics and drug therapy. Once improvements in sensitivity, throughput and sample requirement are accomplished, proteomic techniques will substantially expand and probably become a standard approach both in the research laboratory and in the clinic. 5. Acknowledgements We apologize to the many colleagues whose work has not been cited due to space constrains. Proteomic studies in the laboratory of V.A. are supported by Laboratorios INDAS (Spain) and Instituto de Salud Carlos III (Red de Centros C03/01). M.K. is a fellow of the European Union Marie Curie Programme. S.M.S.-G. and F. V. are fellows of the Instituto de Salud Carlos III. 6. References [1]. Liebler, D.C. Environ Health Perspect, 2002, 110 Suppl 1, 3. [2]. Anderson, L.; Seilhamer, J. Electrophoresis, 1997, 18, 533. [3]. Abbott, A. Nature, 1999, 402, 715. [4]. Krishna, R.G.; Wold, F. Adv Enzymol Relat Areas Mol Biol, 1993, 67, 265. [5]. Gorg, A.; Obermaier, C.; Boguth, G.; Harder, A.; Scheibe, B.; Wildgruber, R.; Weiss, W. Electrophoresis, 2000, 21, 1037. [6]. Aebersold, R.; Mann, M. Nature, 2003, 422, 198. [7]. Zuo, X.; Speicher, D.W. Proteomics, 2002, 2, 58. [8]. Petricoin, E.F.; Zoon, K.C.; Kohn, E.C.; Barrett, J.C.; Liotta, L.A. Nat Rev Drug Discov, 2002, 1, 683. [9]. Shin, B.K.; Wang, H.; Yim, A.M.; Le Naour, F.; Brichory, F.; Jang, J.H.; Zhao, R.; Puravs, E.; Tra, J.; Michael, C.W.; Misek, D.E.; Hanash, S.M. J Biol Chem, 2003, 278, 7607. [10]. Neuhoff, V.; Stamm, R.; Pardowitz, I.; Arold, N.; Ehrhardt, W.; Taube, D. Electrophoresis, 1990, 11, 101. [11]. Switzer, R.C., 3rd; Merril, C.R.; Shifrin, S. Anal Biochem, 1979, 98, 231. [12]. Patton, W.F. Electrophoresis, 2000, 21, 1123. [13]. Patton, W.F. J Chromatogr B Analyt Technol Biomed Life Sci, 2002, 771, 3. [14]. Flory, M.R.; Griffin, T.J.; Martin, D.; Aebersold, R. Trends Biotechnol, 2002, 20, S23. [15]. Larsen, M.R.; Roepstorff, P. Fresenius J Anal Chem, 2000, 366, 677. [16]. Mann, M.; Hendrickson, R.C.; Pandey, A. Annu Rev Biochem, 2001, 70, 437. 12 [17]. Pandey, A.; Mann, M. Nature, 2000, 405, 837. [18]. Hunt, D.F.; Henderson, R.A.; Shabanowitz, J.; Sakaguchi, K.; Michel, H.; Sevilir, N.; Cox, A.L.; Appella, E.; Engelhard, V.H. Science, 1992, 255, 1261. [19]. Brivio, M.; Fokkens, R.H.; Verboom, W.; Reinhoudt, D.N.; Tas, N.R.; Goedbloed, M.; van den Berg, A. Anal Chem, 2002, 74, 3972. [20]. Link, A.J.; Eng, J.; Schieltz, D.M.; Carmack, E.; Mize, G.J.; Morris, D.R.; Garvik, B.M.; Yates, J.R., 3rd. Nat Biotechnol, 1999, 17, 676. [21]. Stoeckli, M.; Chaurand, P.; Hallahan, D.E.; Caprioli, R.M. Nat Med, 2001, 7, 493. [22]. Zhu, H.; Klemic, J.F.; Chang, S.; Bertone, P.; Casamayor, A.; Klemic, K.G.; Smith, D.; Gerstein, M.; Reed, M.A.; Snyder, M. Nat Genet, 2000, 26, 283. [23]. Zhu, H.; Bilgin, M.; Bangham, R.; Hall, D.; Casamayor, A.; Bertone, P.; Lan, N.; Jansen, R.; Bidlingmaier, S.; Houfek, T.; Mitchell, T.; Miller, P.; Dean, R.A.; Gerstein, M.; Snyder, M. Science, 2001, 293, 2101. [24]. MacBeath, G.; Schreiber, S.L. Science, 2000, 289, 1760. [25]. Pellois, J.P.; Zhou, X.; Srivannavit, O.; Zhou, T.; Gulari, E.; Gao, X. Nat Biotechnol, 2002, 20, 922. [26]. Paweletz, C.P.; Charboneau, L.; Bichsel, V.E.; Simone, N.L.; Chen, T.; Gillespie, J.W.; Emmert-Buck, M.R.; Roth, M.J.; Petricoin, I.E.; Liotta, L.A. Oncogene, 2001, 20, 1981. [27]. Robinson, W.H.; DiGennaro, C.; Hueber, W.; Haab, B.B.; Kamachi, M.; Dean, E.J.; Fournel, S.; Fong, D.; Genovese, M.C.; de Vegvar, H.E.; Skriner, K.; Hirschberg, D.L.; Morris, R.I.; Muller, S.; Pruijn, G.J.; van Venrooij, W.J.; Smolen, J.S.; Brown, P.O.; Steinman, L.; Utz, P.J. Nat Med, 2002, 8, 295. [28]. Ziauddin, J.; Sabatini, D.M. Nature, 2001, 411, 107. [29]. Jungblut, P.; Otto, A.; Regitz, V.; Fleck, E.; Wittmann-Liebold, B. Electrophoresis, 1992, 13, 739. [30]. Corbett, J.M.; Wheeler, C.H.; Baker, C.S.; Yacoub, M.H.; Dunn, M.J. Electrophoresis, 1994, 15, 1459. [31]. Jungblut, P.; Otto, A.; Zeindl-Eberhart, E.; Plessner, K.P.; Knecht, M.; Regitz-Zagrosek, V.; Fleck, E.; Wittmann-Liebold, B. Electrophoresis, 1994, 15, 685. [32]. Baker, C.S.; Corbett, J.M.; May, A.J.; Yacoub, M.H.; Dunn, M.J. Electrophoresis, 1992, 13, 723. [33]. Kovalyov, L.I.; Shishkin, S.S.; Efimochkin, A.S.; Kovalyova, M.A.; Ershova, E.S.; Egorov, T.A.; Musalyamov, A.K. Electrophoresis, 1995, 16, 1160. [34]. Muller, E.C.; Thiede, B.; Zimny-Arndt, U.; Scheler, C.; Prehm, J.; Muller-Werdan, U.; Wittmann-Liebold, B.; Otto, A.; Jungblut, P. Electrophoresis, 1996, 17, 1700. [35]. Evans, G.; Wheeler, C.H.; Corbett, J.M.; Dunn, M.J. Electrophoresis, 1997, 18, 471. [36]. Dunn, M.J.; Corbett, J.M.; Wheeler, C.H. Electrophoresis, 1997, 18, 2795. [37]. Li, X.P.; Pleissner, K.P.; Scheler, C.; Regitz-Zagrosek, V.; Salnikow, J.; Jungblut, P.R. Electrophoresis, 1999, 20, 891. [38]. Weekes, J.; Wheeler, C.H.; Yan, J.X.; Weil, J.; Eschenhagen, T.; Scholtysik, G.; Dunn, M.J. Electrophoresis, 1999, 20, 898. [39]. Corbett, J.M.; Wheeler, C.H.; Dunn, M.J. Electrophoresis, 1995, 16, 1524. [40]. Weiss, H.D.; Betz, E.; Karsch, K.R. Electrophoresis, 1992, 13, 757. [41]. Bruneel, A.; Labas, V.; Mailloux, A.; Sharma, S.; Vinh, J.; Vaubourdolle, M.; Baudin, B. Proteomics, 2003, 3, 714. [42]. Patton, W.F.; Erdjument-Bromage, H.; Marks, A.R.; Tempst, P.; Taubman, M.B. J Biol Chem, 1995, 270, 21404. [43]. Nichols, N.R.; Lloyd, C.J.; Mendelsohn, F.A.; Funder, J.W. Mol Cell Endocrinol, 1983, 32, 245. [44]. Nichols, N.R.; McNally, M.; Campbell, J.H.; Funder, J.W. J Hypertens, 1984, 2, 663. [45]. Yu, Y.L.; Yang, P.Y.; Fan, H.Z.; Huang, Z.Y.; Rui, Y.C. Acta Pharmacol Sin, 2003, 24, 873. [46]. Arrell, D.K.; Neverova, I.; Fraser, H.; Marban, E.; Van Eyk, J.E. Circ Res, 2001, 89, 480. 13 [47]. Arnott, D.; O'Connell, K.L.; King, K.L.; Stults, J.T. Anal Biochem, 1998, 258, 1. [48]. Pellieux, C.; Desgeorges, A.; Pigeon, C.H.; Chambaz, C.; Yin, H.; Hayoz, D.; Silacci, P. J Biol Chem, 2003, 278, 29136. [49]. Cremona, O.; Muda, M.; Appel, R.D.; Frutiger, S.; Hughes, G.J.; Hochstrasser, D.F.; Geinoz, A.; Gabbiani, G. Exp Cell Res, 1995, 217, 280. [50]. Heinke, M.Y.; Wheeler, C.H.; Chang, D.; Einstein, R.; Drake-Holland, A.; Dunn, M.J.; dos Remedios, C.G. Electrophoresis, 1998, 19, 2021. [51]. Heinke, M.Y.; Wheeler, C.H.; Yan, J.X.; Amin, V.; Chang, D.; Einstein, R.; Dunn, M.J.; dos Remedios, C.G. Electrophoresis, 1999, 20, 2086. [52]. Sakai, J.; Ishikawa, H.; Kojima, S.; Satoh, H.; Yamamoto, S.; Kanaoka, M. Proteomics, 2003, 3, 1318. [53]. Schwertz, H.; Langin, T.; Platsch, H.; Richert, J.; Bomm, S.; Schmidt, M.; Hillen, H.; Blaschke, G.; Meyer, J.; Darius, H.; Buerke, M. Proteomics, 2002, 2, 988. [54]. Laussmann, T.; Janosi, R.A.; Fingas, C.D.; Schlieper, G.R.; Schlack, W.; Schrader, J.; Decking, U.K. Faseb J, 2002, 16, 628. [55]. Weekes, J.; Watson, R.R.; Dunn, M.J. Alcohol Alcohol, 2003, 38, 103. [56]. Patel, V.B.; Corbett, J.M.; Dunn, M.J.; Winrow, V.R.; Portmann, B.; Richardson, P.J.; Preedy, V.R. Electrophoresis, 1997, 18, 2788. [57]. Skehel, J.M.; Schneider, K.; Murphy, N.; Graham, A.; Benson, G.M.; Cutler, P.; Camilleri, P. Electrophoresis, 2000, 21, 2540. [58]. Ping, P.; Zhang, J.; Pierce, W.M., Jr.; Bolli, R. Circ Res, 2001, 88, 59. [59]. Edmondson, R.D.; Vondriska, T.M.; Biederman, K.J.; Zhang, J.; Jones, R.C.; Zheng, Y.; Allen, D.L.; Xiu, J.X.; Cardwell, E.M.; Pisano, M.R.; Ping, P. Mol Cell Proteomics, 2002, 1, 421. [60]. You, S.A.; Archacki, S.R.; Angheloiu, G.; Moravec, C.S.; Rao, S.; Kinter, M.; Topol, E.J.; Wang, Q. Physiol Genomics, 2003, 13, 25. [61]. Duran, M.C.; Mas, S.; Martin-Ventura, J.L.; Meilhac, O.; Michel, J.B.; Gallego-Delgado, J.; Lazaro, A.; Tunon, J.; Egido, J.; Vivanco, F. Proteomics, 2003, 3, 973. [62]. Kocher, O.; Gabbiani, G. Hum Pathol, 1986, 17, 875. [63]. Stastny, J.; Robertson, A.L., Jr.; Fosslien, E. Exp Mol Pathol, 1986, 45, 279. [64]. Stastny, J.; Fosslien, E.; Robertson, A.L., Jr. Atherosclerosis, 1986, 60, 131. [65]. Song, J.; Stastny, J.; Fosslien, E.; Robertson, A.L., Jr. Exp Mol Pathol, 1985, 43, 297. [66]. Pleissner, K.P.; Regitz-Zagrosek, V.; Weise, C.; Neuss, M.; Krudewagen, B.; Soding, P.; Buchner, K.; Hucho, F.; Hildebrandt, A.; Fleck, E. Electrophoresis, 1995, 16, 841. [67]. Ritter, O.; Luther, H.P.; Haase, H.; Baltas, L.G.; Baumann, G.; Schulte, H.D.; Morano, I. J Mol Med, 1999, 77, 677. [68]. Thiede, B.; Otto, A.; Zimny-Arndt, U.; Muller, E.C.; Jungblut, P. Electrophoresis, 1996, 17, 588. [69]. Kovalyov, L.I.; Naumov, V.G.; Pulyayeva, H.V.; Samko, A.M.; Tsvetkova, M.N.; Shishkin, S.S.; Mukharlyamov, N.M. Electrophoresis, 1990, 11, 333. [70]. Corbett, J.M.; Why, H.J.; Wheeler, C.H.; Richardson, P.J.; Archard, L.C.; Yacoub, M.H.; Dunn, M.J. Electrophoresis, 1998, 19, 2031. [71]. Weekes, J.; Morrison, K.; Mullen, A.; Wait, R.; Barton, P.; Dunn, M.J. Proteomics, 2003, 3, 208. [72]. Scheler, C.; Muller, E.C.; Stahl, J.; Muller-Werdan, U.; Salnikow, J.; Jungblut, P. Electrophoresis, 1997, 18, 2823. [73]. Scheler, C.; Li, X.P.; Salnikow, J.; Dunn, M.J.; Jungblut, P.R. Electrophoresis, 1999, 20, 3623. 14 Table 1: On line databases of 2D PAGE maps of heart tissue and cell types of relevance in cardiovascular pathophysiology Source Human, dog Database rat HSC-2D PAGE Web-URL address http://www.harefield.nthames.nsh.uk/nhli/protein/ HEART-2D PAGE http://userpage.chemie.fu-berlin.de/~pleiss/dhzb.html HP-2D PAGE http://www.mdc-berlin.de/~emu/heart/ TMIG, Proteome http://www.proteome.jp/2D/XML/Endothel/endothel_menu.html Database of HUVEC Human Rat SWISS-2D PAGE (U937 cells) http://www.expasy.org/ch2dothergifs/publi/u937.gif SWISS-2D PAGE (red blood cells) SWISS-2D PAGE (platelets) OGP-WWW database (platelets) HUVEC-2D PAGE http://www.expasy.org/ch2dothergifs/publi/rbc.gif http://www.expasy.org/ch2dothergifs/publi/platelet.gif http://proteomewww.glycob.ox.ac.uk/2d/2d.html http://www.huvec.com (in construction) RAT HEART-2D PAGE http://www.mpiib-berlin.mpg.de/2D-PAGE/ 15 Table 2: Proteomic studies of relevance in vascular pathobiology SPECIES Bovine EXPERIMENTAL APROACH REFERENCES Control vs glucocorticoid-treated aortic ECs [43,44] and SMCs EC cultures exposed to plaque-free vs plaque- [48] prone flows. Rat Control vs glucocorticoid-treated SMCs and [44] ECs Mitogen-starved vs mitogen-stimulated aortic [42] SMCs Newborn vs old SMCs [49] Mouse Serum from atherosclerosis prone [57] apolipoprotein E*3-Leiden mice vs wild-type mice Human Control vs atherosclerotic coronary artery Atheroma-free thoracic aorta from young vs old individuals Media vs atheroma (aorta, femoral and coronary artery) Aortic intima from lesion free vs fibro- fatty lesions Proteins secreted by normal vs atheroclerotic tissue Quiescent HUVECS Control vs oxLDL-treated U937 cells Rabbit [60] [65] [62] [63,64] [61] [41] [45] Proliferating vs nonproliferating SMCs in [40] culture 16 Table 3: Proteomic analysis of cultured cardiomyocytes and cardiac tissue SPECIES EXPERIMENTAL APROACH Bovine Control and glucocorticoid-treated cultured [44] cardiomyocytes Control and DCM ventricular myocardium [38] Rat Mouse Human Control and glucocorticoid-treated cultured cardiomyocytes Control, isquemic and isquemic-reperfusion heart Cardiac tissue from control and alcohol-treated animals Control and phenylephrine-induced hypertrophic cardiomyocyte REFERENCES [44] [52] [56] [47] Cardiac tissue from PKC- transgenic and wild- [58,59] type mice Murine model of AIDS to asses the effect of [55] chronic alchohol comsumption on cardiac tissue Identification of cardiac proteins Left ventricular and right atrial samples from end-stage explanted and healthy heart Control and hypertrophied ventricular myocardium Control and diseased heart (DCM, IHD) [29-31] [66] [67] [68,70-73] Rabbit Control and pharmacologically preconditioned [46] ventricular cardiomyocytes Myocardial protein expression following [53] ischemia and reperfusion, with or without FUT175 Dog Cardiac tissue from regions subjected to low and [54] high blood flow Control and pacing-induced heart failure [50,51] 17 GENE GENOME Transcription Introns I II III IV V pre mRNA Exons 1 2 3a 3b 3c 4 Alternative splicing mRNA 1 2 3a 4 Translation Protein 3a 1 2 3b 4 1 2 Translation Protein 3b 3c TRANSCRIPTOME 4 Translation Protein 3c Post-translational modifications Expressed proteins PROTEOME Phenotype Fig.1: Phenotype versus genotype complexity. Gene transcription results in the generation of a precursor messenger RNA (pre-mRNA) that includes both coding (exon) and non-coding (intron) gene sequences. Unless alternative transcriptional starting sites are present, each gene is transcribed in a single premRNA transcript. Mature messenger RNAs (mRNA) are generated by splicing of pre-mRNAs, a process that involves the excision of introns and joining of exon sequences. The example shows a hypothetical gene with 5 introns (I-V), 6 exons (1, 2, 3a, 3b, 3c and 4). Note that alternative splicing can give rise to three distinct mRNAs each bearing a different variant of exon 3. mRNA translation by the ribosome will generate structural and functional diverse proteins from the respective mRNA species. Once expressed, proteins undergo posttranslational modifications like three-dimensional folding and chemical protein modifications that can greatly affect protein function, localization and stability. To date, more than 200 different protein modifications have been described [4], including phosphorylation, methylation, glycosilation, prenylation, and sulfatation. Moreover, individual proteins often function as parts of large multiprotein complexes and networks, thus adding complexity to the regulation of protein function and stability. Taken into account the diversity of posttranslational modifications, the complexity of the proteome greatly exceeds that of the underlying transcriptome and genome. 18 kDa TISSUE SAMPLING 200 115 80 50 35 27 18 Control Pathologic “Control” .…... .. . . . . .. . … … .. . . kDa 200 115 80 50 35 27 18 “Pathologic” . . . .…... .. . . . . . .. . … … .. Protein extraction and solubilization 2 - 4 6 8 10 pH + Staining and image analysis 1st DIMENSION: Isoelectrofocusing (pH gradient) Excision of differentially expressed proteins Partial proteolysis (i.e. trypsin) Peptide digestion mix kDa Mass spectrometry 200 115 80 50 35 27 18 Bioinformatics (protein data base) 2nd DIMENSION: SDS-PAGE (molecular weight) Identification of proteins and post-translational modifications DIAGNOSTIC MARKERS THERAPEUTIC TARGETS Functional proteomics Fig. 2: Usual steps in proteomic analysis. Control and pathological tissues are collected for protein extraction and solubilization prior to bidimensional separation. In the first dimension (isoelectric focusing), solubilized proteins are applied to an IPG (Immobilized pH Gradient) strip. In the second dimension, IPG strips are subjected to SDS-PAGE. Gels are then stained and image analysis with suitable software is performed. Spots that display differential patterns when comparing control and pathological specimens are excised from the gel and digested with a specific protease (i.e. trypsin). The resulting peptide mixtures are analyzed by mass spectrometry in order to identify the corresponding proteins by searching in available protein databases. Conventional proteomic analysis and functional proteomics not only shed significant insight into the mechanisms underlying basic biological processes, but also help identify diagnostic markers and therapeutic targets. 19