interventionalradiologyangiography-140219074619-phpapp02.ppt
advertisement

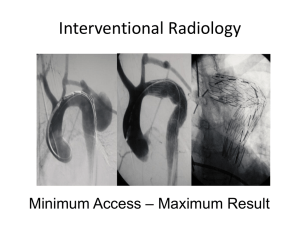
INTERVENTIONAL RADIOLOGY & ANGIOGRAPHY DR. Walid Asaad, MBBS, MD, DABR,CAQ Diagnostic &Interventional Radiology King Abdulaziz University Hospital INTERVENTIONAL RADIOLOGY A subspecialty which provides minimally invasive techniques with the help of imaging modalities to diagnose or treat a condition. Minimally invasive Local anesthesia Early recovery 8 out of 10 procedures use skin incisions smaller than 5 mm. 9 out of 10 procedures use only local anaesthetic, sometimes with sedation. Up to 8 out of 10 patients go home the same day INTERVENTIONAL RADIOLOGY Stent placement Embolization Thrombolysis Balloon angioplasty Atherectomy Electrophysiology Percutaneous biopsy Abscess drainage Percutaneous nephrostomy Percutaneous Biliary drainage Radiofrequency ablation ANGIOGRAPHY The radiologic examination of vessels after the introduction of a contrast medium. HISTORY The first angiogram was performed only months after Roentgen's discovery of X rays. Which was when? Two physicians injected mercury salts into an amputated hand and created an image of the arteries Post mortem injection of mercury salts in Jan,1896. Interventional radiologic procedures began in 1930s with angiography. In early 1960s Mason Jones pioneered transbrachial selective coronary angiography. Later in 1960s transfemoral angiography was developed. BASIC PRINCIPLES Arterial access In 1953 Seldinger described a method for catheterization of vessels. A percutaneous technique for arterial and venous access. Femoral artery is most commonly used. SELDINGER TECHNIQUE Seldinger needle. 18gauge single use,sterile needle. 2 parts-- a solid inner needle(stylet) & an outer thin wall needle for smooth passage. a hub---good instrument balance winged handle---good control. Site cleaned, area draped, local anesthetic given. The seldinger needle is introduced into the artery. When pulsating blood returns, the stylet is removed. A guide wire is inserted through the needle. With guide wire in vessel, needle is removed. Catheter is threaded onto the guide wire. Under fluoro, the catheter is then advanced and the guide wire is removed. GUIDEWIRES Guide the catheter. Allow safe introduction of catheter into the vessel. Made of stainless steel. Usually about 145cm long An inner core wire that is tapered at the end to a soft flexible tip. Covered by a coating—teflon, heparin and recently hydrophilic polymers(glide wires) are used. Coating reduces friction, gives strength to GW. Tips at the end of GW Straight J- tipped—prevents subintimal dissection of artery. CATHETERS •Many shapes and sizes. •diameter is given in French(Fr)—3Fr=1mm. •Straight- end hole only—smaller vessels/minimal contrast. •Pigtail- circular tip with multiple side holes — larger vessels/ more contrast. H1 or Head hunter tip– used for femoral approach to brachiocephalic vessels. Simmons catheter is highly curved --- for sharply angled vessels--cerebral and visceral angiography. C2 or Cobra catheter has angled tip joined to a gentle curve—celiac, renal & mesenteric arteries. Judkins catheters Right(lesser curve) & left(greater curve) for right & left coronary arteries. Amplatz catheters Right & left coronary arteries Contrast Media Initially ionic iodine compounds were used. Now non ionic contrast media in practice—low adverse reactions and low physiologic problems. INDICATIONS Diagnosis & presence of ischemic heart disease. After revascularization procedures Congenital heart lesions & anomalies of great vessels. Valve disease, myocardial disease & ventricular function. Atheroma Aneurysms Arteriovenous malformations Arterial ischemia Trauma Patient preparation Explain procedure & risk to the patient. History & physical examination. Lab tests. Consent Pre procedure I/V fluids. Medication to relieve anxiety. Monitoring during and after procedure ECG, Automatic BP measurement & pulse oximetry. Life saving drugs and equipments. Immobile for minimum 4hrs after. Vital signs monitored. Puncture site inspected. Contra-indications Contrast allergy Impaired renal function Blood- clotting disorders Anti coagulant medication Unstable cardio pulmonary/ neurological status Risks Bleeding at puncture site Thrombus formation Embolus formation –plaque dislodged from vessel wall by catheter Dissection of vessel Puncture site infection ( contaminated sterile field) Contrast reaction INTERVENTIONAL RADIOLOGY SUITE Specifically designed to accommodate the quantity of equipment needed & the large number of people involved in the procedure. Interventional radiology suite Procedure Room Room size- 400-600 square feet Easily cleaned (floors, wall, etc.) Outlets needed for O2, suction. At least three means of access. Control Room 100-150 square feet Easy access and communication to procedure room Operating console with Computers, monitors . EQUIPMENTS The X-ray apparatus for interventional radiology is more massive,flexible,expensive & advanced. More heat load and serial images. X RAY TUBE Two ceiling track-mounted X-ray tubes alongwith an image intensified fluoroscope mounted on C or an L arm. A large diameter massive anode disc(15cm diameter, 5cm thick) to accommodate heat load. Cathodes designed for magnification & serial radiography. A large focal spot of 1mm for heat load. A small focal spot( no more than 0.3mm) is necessary for spatial resolution of small vessel magnification. Power rating of 80kW—for rapid sequence serial radiography. Anode heat capacity of 1 MHU—to accommodate heat load. Generators High frequency and high voltage generators Three phase,12 pulse power. Patient couch Stationary couch with a floating,tilting or rotating table top. Controls for couch positioning are located on side of table and also on a floor switch. May also have a computer controlled stepping capability. Image receptor 2 different types. Cinefluorographic camera—now obsolete. Nowadays Digital image receptors are used with a television camera pickup tube or a charge-coupled device(CCD). THANKS