Treatment Evidence Form – Provide Self Tanning Unit 845
advertisement

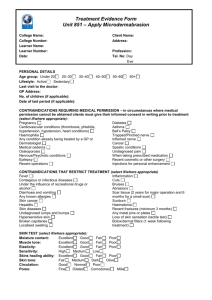
Treatment Evidence Form Unit 845 – Provide Self Tanning College Name: College Number: Learner Name: Learner Number: Date: PERSONAL DETAILS Age group: Under 20 20–30 Lifestyle: Active Sedentary Last visit to the doctor: GP Address: No. of children (if applicable): Date of last period (if applicable): Client Name: Address: Profession: Tel. No: Day 30–40 40–50 50–60 Eve 60+ CONTRAINDICATIONS REQUIRING MEDICAL PERMISSION – in circumstances where medical permission cannot be obtained clients must give their informed consent in writing prior to treatment (select if/where appropriate): Epilepsy Asthma Cardio vascular conditions (thrombosis, phlebitis, Any condition already being treated by a GP or hypertension, hypotension, heart conditions) dermatologist Recent scar tissue Medical oedema Diabetes Nervous/Psychotic conditions Bell’s Palsy Inflamed nerve Trapped/Pinched nerve CONTRAINDICATIONS THAT RESTRICT TREATMENT (select if/where appropriate): Fever Skin diseases Contagious or infectious diseases Vitiligo Under the influence of recreational drugs or Albinism alcohol Hypersensitive skins Diarrhoea and vomiting Highly vascular skins Skin cancer Undiagnosed lumps and bumps Photosensitive skins Pregnancy (sun beds only) Urticaria Cuts Medication which causes the skin to become Bruises photosensitive, e.g. antibiotics, some blood pressure Abrasions medication, tranquillisers Scar tissue (2 years for major operation and 6 months After any form of heat treatment for a small scar) After waxing Sunburn After electrolysis Areas of undiagnosed pain Excessive moles (more than 100) Any metal pins or plates Contact lenses (unless removed) Loss of skin sensation Epilepsy After a heavy meal (sun beds only) Recent operations Recent X-ray (3 months) Acute rheumatism Botox/dermal fillers (1 week following treatment) WRITTEN PERMISSION REQUIRED BY: GP/Specialist Informed consent Either of which should be attached to the consultation form Level 3 Unit 845 – Provide Self Tanning Treatment Evidence Form PATCH TEST: Self tanning: Yes No TREATMENT: (select if/where appropriate) Spray gun Compressor Buffing mitt PRODUCTS: (select if/where appropriate) Tanning cream Tanning gels Spray tan liquid Barrier cream Exfoliators Moisturisers Treatment details: Client feedback: After/Home care advice given: Client Signature………………………………………………………….… Learner Signature…………………………………………………………. Level 3 Unit 845 – Provide Self Tanning Treatment Evidence Form