Parasitology 3rd lecture
advertisement

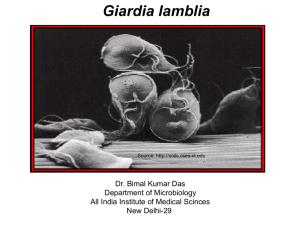
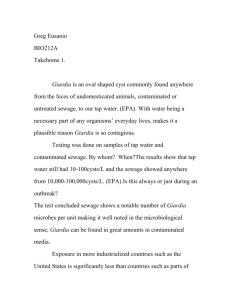
Giardia lamblia is a flagellated protozoan parasite that colonises and reproduces in the small intestine, causing giardiasis. The giardia parasite attaches to the epithelium by a ventral adhesive disc, and reproduces via binary fission. Giardiasis does not spread via the bloodstream, nor does it spread to other parts of the gastro-intestinal tract, but remains confined to the lumen of the small intestine. Giardia trophozoites absorb their nutrients from the lumen of the small intestine, and are anaerobes. If the organism is split and stained, it has a very characteristic pattern that resembles a familiar "smiley face" symbol. Giardia infection occurs worldwide, with an incidence usually ranging from 1.5 to 20%. Although people of all ages may harbor these organisms, infants and children are more often infected than are adults. Only1/3 of infected people exhibit symptoms. Carriers are probably more important in the spread of these organisms than symptomatic patients because cysts are less likely to be present in diarrheic stool. Like other diseases spread by the fecal-oral route, giardiasis can be a problem in institutions, nurseries, and day-care centers Recent outbreaks, some of epidemic proportions, have occurred, particularly in North America and the Soviet Union. These outbreaks have been caused by drinking contaminated water from community water supplies or directly from rivers and streams. It has been recognized only recently that Giardia infection may be transmitted by sexual activity, particularly among homosexual men, but also heterosexually. The trophozoite is easily recognized under a microscope: it is about 12 to 15 μm long, shaped like a pear cut in half lengthwise, and has two nuclei that resemble eyes, structures called median bodies that resemble a mouth, and four pairs of flagella that look like hair; these combine to give the stained trophozoite the appearance of a face. The flagella help these organisms to migrate to a given area of the small intestine, where they attach by means of an adhesive disk to epithelial cells. The Giardia cyst - the form usually seen in the feces - is ovoid, 6 to 12 μm long, and can often be seen to contain two to four nuclei at one end and prominent diagonal fibrils. Giardia infection can occur through ingestion of dormant cysts in contaminated water, food, or by the faecal-oral route (through poor hygiene practices). Giardia cyst can survive for weeks to months in warm water, and therefore can be present in contaminated wells and water systems. They may also occur in city reservoirs and persist after water treatment, as the Giardia cysts are resistant to conventional water treatment methods such as chlorination. The life cycle begins with a non infective cyst being excreted with the faeces of an infected individual. The cyst is hardy, providing protection from various degrees of heat and cold, desiccation, and infection from other organisms. Once ingested by a host, the trophozoite emerges to an active state of feeding and motility. After the feeding stage, the trophozoite undergoes asexual replication through longitudinal binary fission. The resulting trophozoites and cysts then pass through the digestive system in the faeces. While the trophozoites may be found in the faeces, only the cysts are capable of surviving outside of the host. Colonization of the gut results in inflammation and villous atrophy, reducing the gut's absorptive capability. Symptoms of infection include: diarrhea, malaise, excessive gas, steatorrhoea (pale, foul smelling, greasy stools), epigastric pain, bloating, and nausea, diminished interest in food, and weight loss. Pus, mucus and blood are not commonly present in the stool. It usually causes "explosive diarrhea“ and while unpleasant, is not fatal. Some studies have shown that giardiasis should be considered as a cause of Vitamin B12 deficiency, this a result of the problems caused within the intestinal absorption system. Giardia lamblia infection in humans is frequently misdiagnosed. Multiple stool examinations are recommended, since the cysts and trophozoites are not shed consistently. Human infection is conventionally treated with metronidazole, tinidazole or nitazoxanide. Attention to personal hygiene is the key to preventing the spread of giardiasis. Controlling the spread of Giardia in drinking water should be possible where community water treatment methods (e.g., disinfection and filtration) are available. For example, iodine and chlorine kill Giardia cysts under appropriate conditions. Destruction of Giardia cysts is more difficult if the water is near freezing or contains considerable organic matter, because under such conditions so much iodine or chlorine must be added that the water is not palatable. Boiling promptly inactivates Giardia cysts and is the best solution. THANK YOU