LUDWIGS ANGINA, OSTEOMYELITIS LECTURE
advertisement

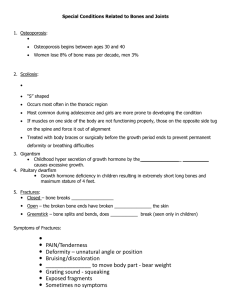
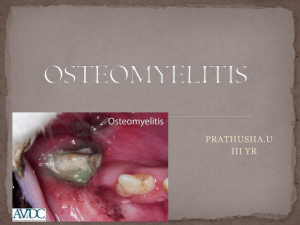
LUDWIG’S ANGINA Definition • Ludwig’s angina is a form of firm, acute, toxic and severe diffuse cellulitis that spreads rapidly, bilaterally, affecting the submandibular, sublingual and submental spaces and resulting in a woody swelling. Etiology Dental infection most commonly the mandibular 3rd molar in 90% of cases. Oral soft tissue lacerations. Puncture wounds of the floor of the mouth. Submandibular gland sialadenitis. Secondary infections of oral malignancies. MICROBIOLOGY Streptococci are most commonly reported Clinical Features Bilateral suprahyoid swelling with hard consistency,non fluctuating & painful on palpation Swelling is characterized by rapid onset Difficulty in breathing (dyspnea), Difficulty in swallowing (odynophagia) Restricted tongue movements, elevated tongue, inability to open the mouth, salivation Patients may exhibit muffled voice due to edema of vocal apparatus (hot potato voice) Firm, brawny swelling in bilateral submandibular & submental and sublingual spaces, non fluctuant,tender with ill defined borders Open mouth due to edema of sublingual tissue Airway obstruction due to edema of the glottis and floor of the mouth Infection can spread to involve the masticator space and Para pharyngeal space in the latter stages of the disease Signs & Symptoms General examination: 1) Patient looks toxic 2) Marked pyrexia 3) Chills and malaise 4) Dysphagia 5) Impaired speech 6) Hoarseness of voice 7) Patient looks dehydrated 8) Respiratory rate is raised. The cardinal signs of Ludwig’s angina are: 1. Bilateral involvement of more than a single deep tissue space 2. Putrid infiltration but little or no frank pus 3. Involvement of connective tissue, fascia, and muscle but not glandular structures 4. Spread via facial space continuity rather than by lymphatic system Diagnosis and Investigations • Ultra-Sonography : Used to identify fluid collection in the soft tissues. • O.P.G • C.T. Scan • M.R.I • Culture & sensitivity • Blood investigations: a) WBC count b) Hb% c) ESR ….. ALWAYS RAISED IN INFECTIONS d) HIV & Hbs-Ag e) RBS PRINCIPLES OF MANAGEMENT • Early diagnosis. • Maintenance of patent airway. • Intense and prolonged antibiotic therapy. • Extraction of the offended teeth. • Surgical drainage / decompression of facial spaces. • Proper post operative care. Antibiotic Therapy • Antibiotic therapy (intravenous) should be intense • Choice of antibiotics include Penicillin+metronidazole or Clindamycin METRONIDAZOLE • Immediate infusion of Metronidazole - 500mg • Brings about rapid improvement • Repeated every 8 hours Steroids • Reduce edema • Used routinely when airway compromise suspected • Dexamethasone- 10 - 20mg IV 4 - 6mg 6th hourly for 8 doses Complications • Septicemia. • Obstruction of upper respiratory airways. • Aspiration pneumonia. • Spread of infection into Para pharyngeal spacesmediastinum-produce thoracic empyema OSTEOMYELITIS DEFINITION In Greek osteon means bone myelos means marrow itis means inflammation “ Osteomyelitis may be defined as an inflammatory condition of bone, that begins as an infection of medullary cavity and haversian systems and extends to involve the periosteum of the affected area ” CLASSIFICATION • Simplest and the most used is based on presence or absence of suppuration • Based on clinical course Based on suppuration SUPPURATIVE ACUTE SUPPURATIVE CHRONIC SUPPURATIVE - PRIMARY - SECONDARY INFANTILE NON SUPPURATIVE CHRONIC SCLEROSING - FOCAL - DIFFUSE GARRE’S SCLEROSING ACTINOMYCOTIC SPECIFIC INFECTIVE - TUBERCULOSIS - SYPHILIS RADIATION CLASSIFICATION • BASED ON CLINICAL COURSE ETIOPATHOGENESIS Infection 3 culprits Trauma Ischemia PROCESS OF OSTEOMYELITIS Acute inflammation following infection ⇃ Hyperemia, ⇃ Capillary permeability ↑and infiltration of granulocytes ⇃ Tissue necrosis ⇃ Destruction of bacteria, vascular thrombosis & Pus forms ⇃ Intramedullary pressure ↑ as pus accumulates -> anesthesia compression ⇃ Vascular collapse, venous stasis and ischemia ⇃ Pus accumulates with Stripping of periosteum ⇃ vascular supply reduced ⇃ periosteum penetration and mucosal fistulas ⇃ chronic Inflammation->granulation tissue & lysis of bone ⇃ separation of necrotic bone (sequestra) ⇃ sheath of new bone (involucrum) CLINICAL FEATURES INCIDincidENCEe: 10 / 100,000 AGE: 10 – 30 YEARS SITE: MANDIBLE > MAXILLA (83% : 1%) BODY - 20% ANGLE - 18% RAMUS - 7% CONDYLE - 2% Acute oml GEN. CONSTITUTIONAL SYMPTOMS DEEP, BORING, INTENSE CONTINUOUS PAIN PARAESTHESIA OR ANAESTHESIA OF LIP FACIAL CELLULITIS OR INDURATED SWELLING FOETID ODOUR TEETH – TENDER TRISMUS Chronic oml PAIN IS MINIMAL NONHEALING WOUNDS WITH INDURATION INTRA ORAL OR EXTRA ORAL SINUS THICKENED OR WOODEN CHARACTER OF BONE ENLARGEMENT OF MANDIBLE PATHOLOGICAL #S LOOSE , TENDER TEETH Radiographic evaluation • 30-60% destruction min 4-8 days to 3 wks. • Mouth eaten appearance, scattered areas of bone destruction • Islands of sequestrae in radiolucent areas surrounded by involucrum INVESTIGATIONS Histopathology • Blood and aspirate culture. • FNAC (infants.) • Samples for culture should be taken from infected cavity wall, sequestrum, granulation tissue, involucrum and sinus tract (misleading). • Organism can be identified and tested for antibiotic sensitivity. MANAGEMENT A. Conservative B. Surgical CONSERVATIVE MANAGEMENT • Supportive therapy- e.g. nutrition. • Control of pain- using analgesics and sedatives. • Antimicrobial agents. ANTIMICROBIAL THERAPY • Penicillin remains the time- honoured antibiotic of choice for osteomyelitis. • Then after obtaining culture and sensitivity report specific therapy is started. Surgical management – Incision & drainage Extraction of teeth Closed wound irrigation & drainage Intra-arterial antibiotics Sequestrectomy Sequestrectomy with saucerization Trephination or Fenestration Decortication Resection Hyperbarbic oxygen therapy