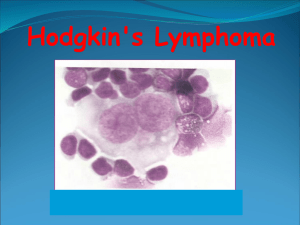
Hodgkin's lymphoma
advertisement

Lymphoma- 1 Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma’ah University Lymphoma 1- Goals • Lymphoma: definition & Classification. • Hodgkin lymphoma: etiology, morphology, clinical features and diagnosis. • Hodgkin lymphoma: management & prognosis. • Lymphoma • Lymphoma: WBC neoplastic proliferations that arise as discrete tissue masses, of clinically important group of cancer (USA 100,000 new cases diagnosed annually) • Cells components: diverse group of lymphoid cells of B-cell, T-cell origin, closely resembles to the various stages of differentiation “lymphocyte maturation”. • Diagnosis, phenotyping, classification, staging, • Lymphoma versus Leukemia (BM,PB,SOLID) Lymphoma-clinical presentation • Clinical presentation of > 2\3 Lymphoma appear as enlarged non-tender lymph node. • Symptoms& signs of malignant lymphoma are due to: • (1) pressure to adjacent structure (skin, stomach, brain) . • (2) through the secretion of circulating factors (in plasmacytoma-destruction of skeletal bone, skull- lytic lesions) • 3) Immunity disturbances Lymph node – cortex and medulla some important principles relevant to the lymphoid neoplasms • ML- Suspicious clinical features, but histologic examination of lymph nodes or other involved tissues is required for diagnosis. • ML- cells clone share similar antigen receptor gene transformation;& configuration. • 85-90% OF ML are B-cell neoplasm, the remainder being Tcell tumors; only rarely are of NK cell origin. • ML- associated with immune abnormalities. (autoimmunity, immunodeficiency) • Neoplastic B and T cells tend to recapitulate the behavior of their normal counterparts(follicular lymphoma, T-cell& skin,etc…). • HL spreads in an orderly fashion. NHL spread widely. ALL CLL Lymphomas MM naïve B-lymphocytes Lymphoid progenitor AML Hematopoietic stem cell Myeloid progenitor Plasma cells T-lymphocytes Myeloproliferative disorders Neutrophils Eosinophils Basophils Monocytes Platelets Red cells B-cell development CLL stem cell mature naive B-cell germinal center B-cell memory B-cell lymphoid progenitor MM progenitor-B ALL pre-B immature B-cell DLBCL, FL, HL plasma cell The current World Health Organization (WHO) classification scheme Based on clinical features, morphology, immunophenotype, genotype, separate neoplasm according to cells of origin 1. Precursor B-cell neoplasms (neoplasms of immature B cells). 2.Peripheral B-cell neoplasms (neoplasms of mature B cells). 3.Precursor T-cell neoplasms (neoplasms of immature T cells). 4.Peripheral T-cell and NK-cell neoplasms (neoplasms of mature T cells and NK cells). 5.Hodgkin lymphoma (neoplasms of Reed-Sternberg cells and variants) Lymphoma classification (WHO) • B-cell neoplasms – precursor – mature • T-cell & NK-cell neoplasms NonHodgkin Lymphomas – precursor – Mature • Hodgkin lymphoma Principle of ideal classification: Accurate Morphology, Re-producibitly , Easy, All types, biological knowledge, Clinical & prognostic relevant Relative frequencies of different lymphomas Non-Hodgkin Lymphomas Diffuse large B-cell Hodgkin lymphoma NHL Follicular Other NHL ~85% of NHL are B-lineage age adjusted incidence/100,000/yr Incidence of lymphomas in comparison with other cancers 70 60 lung colorectal breast 50 40 30 20 NHL 10 Hodgkin lymphoma 0 1985 1990 1995 Year 2000 Lymphoma 1- Goals • Lymphoma: definition & Classification. • Hodgkin lymphoma: etiology, morphology, clinical features and diagnosis. • Hodgkin lymphoma: management & prognosis. • Hodgkin’s Lymphoma • HL was discovered centuries ago. - 1832- written paper: • “enlargement of the glands • appeared to be a primitive affection • of those bodies, rather than the result • of an irritation... from some ulcerated • surface or other inflamed texture. Hodgkin’s Lymphoma - HL HL- has distinctive pathologic features and is treated in a unique fashion. More often localized to a single axial group of nodes (cervical, mediastinal,) Orderly spread by contiguity Extra-nodal - rare Mesenteric nodes rarely +ve. Epidemiology • less frequent than non-Hodgkin lymphoma • overall M>F • occurrence shows two peaks: the first in young adulthood (age 15–35y) and the second in those over 55 years old HL-WHO CLASSIFICATION • WHO recognized 5 sub-types: 1. 2. 3. 4. 5. Nodular sclerosis Mixed cellularity Lymphocyte-rich Lymphocyte depletion Lymphocyte predominance Note: RS for the 1st four have similar Immunophenotyping, lump together in (classical form HL), Lymphocyte predominance- RS has B-cell phenotype “non-classical” Hodgkin’s Disease- etiology • Genetic alterations: Ig gene of RS cells- undergone chromosome abnormality & hypermutation- RS- confirm to be of B-cell origin of the cells, derived from germinal center – (crippled immunoglobulin genes) + lead to inhibition of apoptosis . • Immunosuppression&Infection (EBV, Human Herpes Virus 6, CMV). • $ Epstein-Barr virus - activate gene promote lymphocytes survival - EBV genome identified in RS, in the M-HL,D-HL,R-HL. • Hodgkin’s Disease- etiology Furthermore, epidemiologic studies have documented an increased risk of HL in patients with a history of infectious mononucleosis. • It is believed that neoplastic RS cells secrete cytokines (eg, IL-5) and chemokines that attract the non-neoplastic inflammatory cell- support RS to survive. A possible model of pathogenesis transforming event(s) EBV? loss of apoptosis cytokines germinal centre B cell RS cell inflammatory response Primary Tumours (MALIGNANT LYMPHOMAS) HODGKIN'S LYMPHOMA- morphology The commonest type of malignant lymphomas Develop at almost any age although it is more common in early adult life and in old age. Gross Picture: (1) Starts localized in a group of lymph nodes usually the cervical, axillary or inguinal and later becomes generalized. (2) The lymph nodes are enlarged, firm & discrete but after infiltration of capsule & perinodal C.T., the nodes become fused forming an irregular fixed mass. (3) The cut surface is homogenous pinkish grey. Primary Tumours (MALIGNANT LYMPHOMAS) (1) HODGKIN'S LYMPHOMA- morphology Gross Picture: The spleen is enlarged, firm & the cut surface shows localized nodules of Hodgkin's tissue. (5) The other viscera may show infiltrate of Hodgkin's tissue. (4) Primary Tumours (MALIGNANT LYMPHOMAS) HODGKIN'S LYMPHOMA- morphology Microscopic Picture: The affected lymph nodes show: Loss of the normal nodal architecture. (2) The normal lymphoid tissue is replaced by a pleomorphic cellular infiltrate formed of: Histiocytes, lymphocytes, plasma cells, eosinophils, neutrophils and (RS cells) Reed-Sternberg. (3) Areas of necrosis and fibrosis. (1) Primary Tumours (MALIGNANT LYMPHOMAS) HODGKIN'S LYMPHOMA Microscopic Picture: Cells closely related to the RS cell are: (a) The lacunar cell which shows shrinkage of cell cytoplasm towards cell wall and nucleus leaving a clear space. (b) Mononuclear Hodgkin's cell which shows a nuclear characteristic similar to RS cell but is smaller. (c) Multinucleated giant cell which shows three or more nuclei Classic (Typical) RS cells & variants Diagnostic •30-60um diam •Amphophilic cytoplasm •Binucleated •Large owel eye esinophilic nucleoli •Mirror image nuclei Popcorn cell LH cell •Polypoid nucleus resembling Popcorn kernels •LP •Mulinucleated •LD •Nuclear Characteristic Similar to RS cells • Shrinkage of cell cytoplasm towards cell wall & nucleus leaving a clear space • Nodular sclerosis Reed-Sternberg Variants Primary Tumours (MALIGNANT LYMPHOMAS) HODGKIN'S LYMPHOMA Microscopic Picture: (4) Typical Reed-Sternberg (RS) cell is a malignant giant cell pathognomonic for Hodgkin's disease. It measures > 40 u in diameter. The cytoplasm is abundant and amphophilic (purple with haematoxylin-eosin stain). The cell contains double nuclei showing the mirrorimage appearance. The nuclei have vesicular appearance due to condensation of chromatin peripherally and a large central eosinophilic nucleolus. HL, WHO Classification-Histologic subtype 1. Nodular sclerosis (65-70%) → Good (excellent) prognosis – Young + adolescent • Thick bands of collagen separating Hodgkin’s tissue into nodules • Lacunar cells are numerous(CD15,30 +VE B-Ve) • More common in women-adolescence (M=F) • Often mediastinal, lower cervical presentation. 2. Mixed cellularity (20-25%) → Fair prognosis (more aggressive) • More common in men – bimodal age distribution (young adults and adults older than 55) • Heterogenous infiltrates: T cells, Plasma cells and eosinophils present • Plentiful RS cells& mononuclear- infected by EBV Hodgkin’s Disease , WHO Classification 3. Lymphocyte depletion (< 5%) → Poor prognosis • Very numerous RS , mononuclear Hodgkin’s cells and pleomorphic variants, infected with EBV=90% • Few lymphocytes & ± Diffuse fibrosis.& +ve HIV 4. Lymphocyte- rich HL: un-common, diffuse effacement, residual nodularity, mononuclear variants and diagnostic Reed-Sternberg cells +. 5. Lymphocyte predominant (NLPHD) (5%) → Good (excellent) prognosis, Nodular infiltrates, small lymphocytes • Hardly any RS cells * Very numerous lymphocytes * Scattering of “popcorn cells” or L & H (lymphocytic and histiocytic) cells-multilobed nuclei &eosinophilic cytoplasm B-marker +ve (CD97alpha, CD20), BCL6- like germinal cente. • N.B: Lymphocyte predominant HD may progress to a B cell lymphoma (large cell type) Classical Hodgkin’s lymphoma histological variants I. classical type of HL Nodular sclerosis – HL broad collagen bands separate into nodules Hodgkin’s lymphoma, mixed cellularity plenty of classical RS+ mononuclear cells Eosinophils Reed-Sternberg cell Lymphocyte- rich Hodgkin’s lymphoma Classic RS cells and variants Hodgkin's disease (lymphocyte depletion type) Many Reed-Sternberg cells and pleomorphic variants are present Classical Hodgkin’s lymphoma histological variants I. Non-classical type of HL Nodular lymphocyte predominant HL with H&L cells (H&E stain+ positive for B-cell marker: CD20&CD45 ) Primary Tumours (MALIGNANT LYMPHOMAS) HODGKIN'S LYMPHOMA type Mixed cellularity Lymphocyte Predominant Lymphocyte depletion Scanty or absent Scanty or absent *Neutrophils *Esinophils *Macrophages *plasma cell Fibrosis Prognosis Mixed cellularity Nodular scleroses ++ + +++ +++ +++ +++ +++ +++ +++ Scanty or absent Scanty or absent Abundant Predominant The best The worst Intermediate Remain the same Capsule thickened & node subdivided by collagen bands into nodules of variable sizes Primary Tumours (MALIGNANT LYMPHOMAS) HODGKIN'S LYMPHOMA Classification of Hodgkin's Lymphoma: For prognostic purposes, Hodgkin's disease has been classified by Rye into 4 types: type Lymphocyte Predominant Lymphocyte depletion Mixed cellularity Nodular scleroses Frequency 15% 15% 30% 40% Lymphocyte ++++ + scanty +++ +++ + +++ +++ +++ ++++ +++ ++ RS cells Typical Atypical *Mononuclear *Lacunar *Pleomorphic M. giant cell +++ +++ +++ +++ Clinical Presentation • I. Asymptomatic painless cervical lymphadenopathy. -Painless, firm, not inflammatory -Stage (I,II)- HL-nodular sclerosis+ HL-lymphocyte predominate • II. Constitutional “Systemic” symptoms (fever, weight loss, night sweat, anorexia, pruritis) (weeks and months) - Disseminated disease (stages III–IV) or the mixed-cellularity or lymphocyte depletion subtypes • III. Contiguous spread - Extension from one lymph node group to another. • 2/3 of patients-mediastinal adenopathy at presentation (Cough or SOB if significant compression.) • IV. Infrequently presents as axillary or inguinal adenopathy. • V. Extranodal spread is serotyped: nodal disease first, splenic disease, hepatic disease, finally BM. Classical Hodgkin Lymphoma Clinical presentation HL- Diagnostic Workup • Tissue excisional biopsy: Adequate (FNAC,open biopsy) for definitive histologic diagnosis. • Apply Immunohistochemical stains for classical RS confirmation CD30(+ve), CD15(+ve), CD45(-ve) • L&H cells: CD97alpha (+ve), CD20(+ve) • Cytogenetic and molecular techniques. • Labs investigations: CBC,ESR,LFT,RFT, • Diagnostic imaging for Staging purpose: CT, MRI, US, X-RAY, Lymphangiogram (for Abdominal, chest and neck screening). Immunohistochemical stains CD30 positive CD15 positive Lymphoma 1- Goals • Lymphoma: definition & Classification. • Hodgkin lymphoma: etiology, morphology, clinical features and diagnosis. • Hodgkin lymphoma: management & prognosis. • HODGKIN'S LYMPHOMA Clinical Staging of Hodgkin's Disease(Ann Arbor Classification): physical examination, radiologic imaging of the abdomen, pelvis, and chest, and biopsy of the bone marrow . Treatment and prognosis HL is classified into 4 stages: Stage I: Involvement of a single lymph node region or a single extra-lymphatic organ or site. Stage II: The disease is limited to two of more region on same side of the diaphragm or localized involvement of an extra-lymphatic organ or site. Stage III: Involvement of lymph node regions on both sides of the diaphragm without or with localized involvement of an extra-lymphatic organ or site. Stage IV: Diffuse involvement of one or more extra-lymphatic organs or sites with or without lymphatic involvement. Staging of lymphoma (Ann Arbor system) Stage I Stage II Stage III Stage IV Treatment • tailored according to the HL disease type, disease stage, and an assessment of the risk of resistant • HL is curable at most- therapies have long term toxicity. • Chemotherap:y Multi-agents& regimens, e.g. : -ABVD: (Adriamycin, Bleomycin, vinblastine, Dacarbzine) - MOPP (mechlorethamine, vincristine, procarbazine, prednisone) • (+) Radiation therapy: stages III, IV, NLPHL (I,II). • No. of courses of chemo according to stage 2-4 early stage, 4-6 aadvanced stage disease. • HEMATOPOIETIC STEM CELL TRANSPLANTAION: used for refractory or relapse cases of HL Prognosis • Stratified into risk groups – The cure rate of stage I,II is close 90%, even with advanced disease Stage IV. – The 5 years survival is 60 to 70%. Late complication: (1)Chemotherapy and radiation therapy have an increased risk of developing second cancers. AML, MDS (2) Drugs toxicity e.g. hypthyrodism, heart& lung toxicity, infertility.