Termites in the Nation's Service (part 2): More details than you wanted
advertisement
: More details than you wanted")
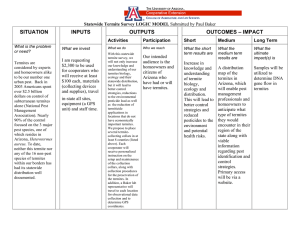
Termites in the Nation's Service (part 2): More details than you wanted Prof. Nina H. Fefferman Visiting DIMACS from : Tufts Univ. School of Medicine, Dept. Public Health and Family Medicine Remember from last time: Temporary Immunity Zootermopsis angusticollis Spores land on termite Metarhizium anisopliae Allogroomed off Burrow through cuticle Death Not a termite What I didn‘t tell you last time: We’ll go through the details for the first round of models – simple, two dimensional, circular nest • Termites have 7 age stages (6 instars, nymph), and they age over time (how long they were in each stage was empirically determined) You can just look at them to determine stage in the real world These aren’t the right termites, but close enough to show you what it looks like http://creatures.ifas.ufl.edu/urban/termites/dampwood_life_cycle.htm • Each 3rd instar and older termite was allowed, but not required, to move one cell per iteration at random in any direction (unless they were at the outer border, naturally) Again, I’m lying with this picture - we were modeling natural nest cavities, but I thought you’d like to see what the lab setup can look like • Health was set at random (0h100) for each individual before the first iteration • Immune status during an iteration was naïve, inoculated, immune, or diseased • Pathogen infection status was defined as either diseased or healthy • Termites determined as dead or alive according to health Termites died either because their health decreased to 0 or to less than a stage specific threshold used to represent a health threshold below which sick individuals were removed/cannibalized Details of disease transfer: these rules applied to each cell (and the termites occupying it) in order • (In the baseline model, all termites are initially defined to be naïve) • Naïve or inoculated (can happen by step 2) termites in cells with primary exposure became diseased • A naïve termite became diseased if the % of diseased termites the cell with it was greater than a defined stage-specific threshold • For each diseased termite in a cell, each naïve termite had an independent stage-specific probability of receiving a dose of fungal spores • Termites that received this inoculum became inoculated • Termites receiving an inoculum were restricted from moving for two iterations (empirically determined) • Termite health values decreased by 10 (representing the cost of mounting the immune response) The sorts of experiments that can be run to get these parameters: Remember that diseased individuals die, so the difference in survival has to do with rates of infection Traniello JF, Rosengaus RB, Savoie K. Proc Natl Acad Sci U S A. 2002 May 14;99(10):6838-42. Survival distributions of Tween 80 controls (□), naïve/challenged nymphs (■), and socially immunized/challenged nymphs (•). (Inset) Histogram illustrating the relative hazard ratios of death of naïve/challenged Using experiments like that when we could to determine threshold values: • Naïve termites had a stage-specific probability of becoming inoculated if the number of immune termites in the same cell with them was > a different stage-specific threshold • Inoculated termites in the same cell with a diseased termite became diseased with a 90% probability • Inoculated termites occupying a cell with no disease present become immune with a 70% probability • The duration of immunity was specified as 300 iterations (30 days), after which the termite would again become naïve Little Details • • • • • • 1 “day” = 10 iterations Only disease affects health value Initially, each termite has an equal probability of being any instar Models run with a starting population of 1000 Model allowed to run for 3600 iterations (one year) Dead termites assumed to be removed, walled off, or cannibalized incapable of infecting other termites • Clutches of 25 eggs were added every 300 iterations (equivalent to 30 days) • New eggs and first-instar larvae were placed in a small circle at nest center. As they developed into second instars from first, they were allowed to move ‘outward’ by one cell (in order to prevent an artificially dense center) • The model placed older instar larvae randomly throughout the nest, though older individuals had a higher probability of being located farther from the center Model Modifications Difference from Baseline Model Adult-biased Demography 70% of ‘worker’ at the outset of the first iteration were adults Early Instar Biased Demography 70% of ‘workers’ at the outset of the first iteration were in instars 1 and 2 Random Spatial Assignment of Individuals Each worker is assigned to a random position in the nest, regardless of developmental stage No Nest Hygiene The threshold for ‘artificial death’ = 0 for all stages No Social Hygienic Behavior Stage dependent thresholds for inoculation from either disease exposure or socially triggered immunity are set to 0 No Nest Hygiene or Social Hygienic Behavior The threshold for ‘artificial death’ = 0 for all stages and Stage dependent thresholds for inoculation from either disease exposure or socially triggered immunity No Immunity Inoculated workers who did not become diseased reverted to naïve status 60% of population immune prior to presence of disease 35% of population immune prior to presence of disease Maintenance of Immunity 20% of population immune prior to presence of disease 15% of population immune prior to presence of disease 10% of population immune prior to presence of disease Under two disease presence scenarios: Low level constant fungal presence - - Fungus was present in 20 cells chosen at random for each iteration Lasted, in each cell, a random number of days ranging from 1-10 Periodic high level fungal presence Fungus was present in 70 cells chosen at random every 90 days - Lasted, in each cell, for 10 days - Some results from the models: Notice that these studies looked at how well the colony did “overall” This is different from traditional studies of disease defense mechanism efficacy Traditional examinations of disease defense efficacy come mainly from studies of vaccine efficacy These models define the benefits of immune protection only in terms of the reduced probability of an individual getting a disease But in the models we’ve just discussed, we were looking at a total ‘societal immunocompetence’ Direct benefits (as with traditional models) and Indirect benefits associated with the prevention of cascading effects (e.g. deaths caused by breakdown of social infrastructure) An example : Pathogen Direct Individual Survival Indirect Sanitation Maintenance Mechanisms: • Few deaths Maybe we don’t upregulate sanitation • Lots of deaths Insufficient funds or manpower down regulation There is already a foundation for this population-wide concept There is the concept of indirect protection provided to susceptible individuals by the mere presence of many immune individuals Immune individuals don’t contract or transmit disease, so, if there are a lot of them in a population, the disease fails to propagate This effectively shields the susceptible individuals from ever coming in contact with the pathogen This is called ‘herd-immunity’, and is well studied But why stop there? Traditional approach : Benefit = ((Mortality rate of individual without immune response) – (Mortality of individual with immune response)) * (Average probability of exposure) Approach we just took: Benefit = ((% Surviving in population capable of an immune response) – (% Surviving in population incapable of an immune response)) / (Size of initial population) The benefit to the entire population in both cases = The sum of individual benefits taken over all members of the population Once we define societal immunocompetence, we can talk about the balance between physiological costs of an immune response and the protection it affords on a population-wide scale unlikely evolutionarily stable Benefits some vaccinations grooming selected against herd immunity crowding Costs Schematic of costs and benefits of disease resistant physiology and behaviors If we can find this equilibrium, we can understand how things like • Vaccination practices and/or • Periodicity of recurring epidemics (with associated induction of short term immunity) • Etc. shape the evolutionary interactions of hosts and pathogens on both an individual and group/societal level Where do these ideas lead? Hopefully many places, but initially: • Study of task allocation based on disease risks to maximize societal immunocompetence Social insect colonies need different tasks completed to make the society function – just like people, only simpler In the framework of costs and benefits, we can look at the influence of disease on the efficiency of the colony in completing these tasks Part of the problem is figuring out how tasks need to get done: We know not all tasks are constant (you don’t always have to clean up after a flood), but there are tasks that need to be done no matter what else has to happen (foraging for food) A lot of models have looked at optimal “recruitment”, but nothing has looked at optimal efficiency for colony task completion Also, each of these tasks are associated with their own risks, pathogen related and otherwise To start with, let’s look at the simplest trade-off system 4 Basic elements of concern: Amount of work in each task completed in each unit of time Age of worker Risk associated with task completion Is the task currently a limiting factor for the colony? How do they all relate? In social insects, there are three basic possibilities for task allocation decisions: 1) Determined by age 2) Repertoire increases with age 3) Completely random So which does better under what assumptions of pathogen risk? Just a few scenarios: 1) As you age, you learn more complicated tasks (i.e. produce more “work” in less time), but these more complicated tasks are riskier 2) The youngest individuals are put on the riskiest tasks so that the lost investment is minimized 3) Everything is completely random, risks, amount of work for each task, everything Additionally, we need to add into the mix – sometimes we need specific tasks more than usual, or more than any other… how do we hedge our bets to make sure that we can always have enough workers to devote to those when we need them? We’d also want to include the benefit in each task to “societal immunocompetence” And we want to check all of this under different probability distributions of “disasters” or “dire need” interfering with a status quo This research is in its infancy, so if anyone is interested… Thanks for listening to me once again I hope you’ve had fun Some of what I’ve talked about is work in collaboration with James Traniello, Rebeca Rosengaus and Sam Beshers