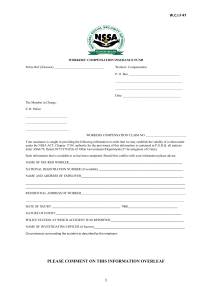
WORKERS’ COMPENSATION Witness Report Claim No.
advertisement

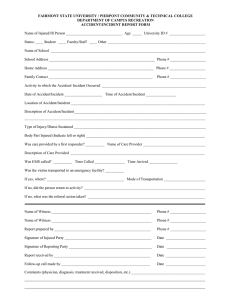
WORKERS’ COMPENSATION Witness Report Claim No. Employee Employer Date of Injury Name Address Employer On Phone Employer Phone , 20 , at a.m./p.m., I was at (state clearly your location) when an accident involving the above employee is alleged to have occurred. (check one) I saw the accident and it occurred in the following manner: I did not see the accident, but information was given to me by (injured employee or witness) indicates it occurred as follows: I have no knowledge of the alleged incident. Signature Date