Witness name Last: First: Residence address:
advertisement

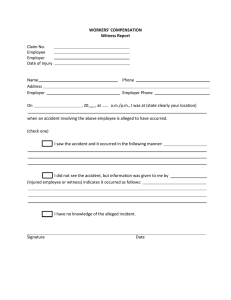
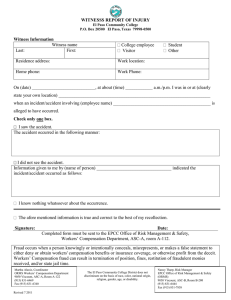
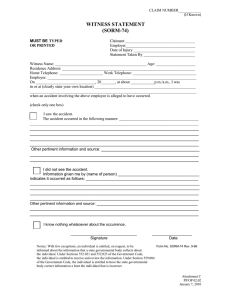
Reset Form Print Form WITNESSS REPORT OF INJURY El Paso Community College P.O. Box 20500 El Paso, Texas 79998-0500 Witness Information Witness name Last: First: College employee Visitor Residence address: Work location: Home phone: Work Phone: Student Other On (date) ____________________________, at about (time) ____________ a.m./p.m. I was in or at (clearly state your own location) ___________________________________________________________________ when an incident/accident involving (employee name) ___________________________________________ is alleged to have occurred. Check only one box. I saw the accident. The accident occurred in the following manner: I did not see the accident. Information given to me by (name of person) _________________________________ indicated the incident/accident occurred as follows: I know nothing whatsoever about the occurrence. The afore mentioned information is true and correct to the best of my recollection. Signature: Date: Sign completed form and mail (College mail OK) to the Risk Management Department at ASC-B. Fraud occurs when a person knowingly or intentionally conceals, misrepresents, or makes a false statement to either deny or obtain workers' compensation benefits or insurance coverage, or otherwise profit from the deceit. Workers’ Compensation fraud can result in termination of position, fines, restitution of fraudulent monies received, and/or state jail time. The El Paso Community College District does not discriminate on the basis of race, color, national origin, religion, gender, age, or disability.