Treatment Plan Example
advertisement

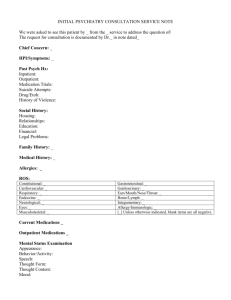
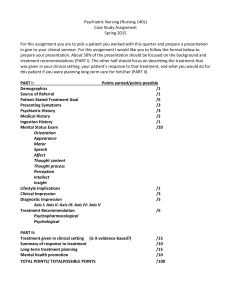
TREATMENT PLAN ADMITTING DIAGNOSES [From psychiatric evaluation, if available] Axis I: 1. __296.32 Major Depressive Disorder, Recurrent, Moderate Axis III: 1. __Deferred to appropriate specialty_____________________ 2. __309.81 Posttraumatic stress disorder (provisional)_______ 2. ________________________________________________________ 3. ________________________________________________________ 3. ________________________________________________________ Axis II: 1. __799.90 Diagnosis deferred_____________________________ Axis IV: ___No obvious current psychosocial stressors______ 2. ________________________________________________________ Axis V: Current G.A.F. _55___ Highest G.A.F. in last year __65______ Prognosis: []Good [x]Fair []Guarded []Poor Estimated Date of Discharge: ____9-15-02______________ Plan Date: ___1-15-02_________ Assessment elements reviewed: [x}psychosocial [x]medical history []psychiatric assessment []________________________________________ Clinician’s integration of assessment findings: Key Findings: 1. Complaints of depressed mood for two months. 2. Intrusive recollection of previous trauma. 3. Passive suicidal wishes. Background: 1. Father committed suicide when client was three. 2. Sexually molested at twelve. 3. Pattern of conflicted relationships with multiple male partners. 4. Three previous episodes of treatment for depression. Formulation: 1. Genetic predisposition for depression. 2. Had little role modeling for effective relationships with men. 3. Unresolved feelings over molestation. 4. Poor coping skills in general. Plan: 1. Counseling to help resolve feelings and teach coping skills. 2. Referral to AMAC. 3. Refer for psychiatric evaluation. Prioritized Problem List: 1. Suicidal wishes 2. Depressed mood 3. Intrusive ideation 4. ___________________________________ Discharge Criteria: 1. The client will report absence of suicidal wishes for three months. 2. The client will report adequate restful sleep 22 or more days per month for three months. 3. The client will report intrusive ideation less than twice per week for eight weeks. 4. ________________________________________________________________________ Strengths to be used in developing treatment plan: Limitations – Special Needs – Barriers to Learning [x]acknowledges illness [x]verbalizes desire for treatment [x]self-reflective [x]insightful [x]able to read [x]able to problem-solve [x]follows directions []accepts responsibility for choices []support system in place Other: familiar with treatment procedures; knows she is a survivor __________________________________________________________ []denies illness []in treatment under duress []denies responsibility for self []hearing impaired []vision impaired []mobility impaired []health problems []reading difficulty []primary language other than English ____________ [x]lacks support system []cognitive limitations [x]emotional limitations Other: discouraged by recurrence of symptoms and apparent intractability of problems _________________________________________________________ NAME: _____Yu__________________Itcudbe______________________________ LAST, FIRST MIDDLE CLIENT NO. ____99999_______________ GOAL Target Date 9-15-02 The client will report that she has had no suicidal wishes for three consecutive months. Objective(s) 1. The client will keep a daily journal and review it with the counselor at each meeting. 2. The client will identify three primary sources of distress and demonstrate at least one coping strategy for each. GOAL The client will report adequate restful sleep for 14 consecutive nights. Objective(s) 1. The client will prepare a personal good sleep habit plan. 2. The client will follow her good sleep habit plan every night, including weekends. 3. The client will document her sleep patterns in her daily journal. GOAL The client will report intrusive ideation less than twice per week for one month. Objective(s) 1. The client will demonstrate thought stopping skills in session. 2. The client will practice thought stopping skills each time she has intrusive thoughts. begin 1-15-02 and continue through treatment 9-15-02 Target Date 4-15-02 1-31-02 3-28-02 begin 1-31-01 and continue through treatment Target Date 5-15-02 2-15-02 begin 2-15-02 and continue through treatment begin 2-15-02 and continue through treatment Target Date 3. The client will document her intrusive thoughts and thought stopping skills in her journal. GOAL Date Resolved Date Resolved Date Resolved Date Resolved Objective(s) FROM TO 1-15-02 4-15-02 TYPE OF SERVICE (individual, group, medication, case management) Individual counseling FREQUENCY AMOUNT of TIME CONTACT weekly 50 minutes R. Goode, LCSW Treatment Plan Reviewed By _______________________________________________________Client Date: _________________________ Treatment Plan Reviewed By _______________________________________________________Staff Date: _________________________ Treatment Plan Reviewed By _______________________________________________________C.M. Date: _________________________ Treatment Plan Reviewed By _______________________________________________________ M.D. Date: _________________________ Six month review by ______________________________________________________________ M.D. Date: _________________________ NAME: _______Yu_____________________Itcudbe_________________________________ LAST, FIRST MIDDLE CLIENT NO. ________________________