CHAPTER 3 Birth and the Newborn Baby: In The New World

CHAPTER 3
Birth and the Newborn Baby: In The
New World
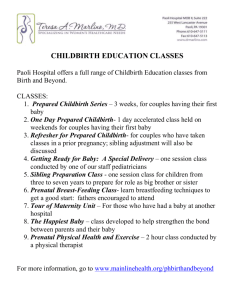
The Stages of Childbirth
• Stage 1
Stages of Childbirth
Effacement & dilation
• Stage 2 Crowning and delivery
• Stage 3 Placental stage
Fig. 3-1, p. 51
Stages of Childbirth
• Stage 1: effacement and dilation
– Begins when uterine contractions efface and dilate cervix , causes most childbirth pain
– Longest stage, lasts from few hours to more than a day
– Results in the widening of the passageway to 4 inches (10 centimeters)
– Transition begins: head of fetus begins to move into the vagina or birth canal
Stages of Childbirth (cont ’ d)
• Stage 2: crowning and delivery
– Baby ’ s head “ crowns ” when it begins to emerge from birth canal
– Contractions stretch the skin around birth canal and propel baby along
– Episiotomy takes place
– Lasts from minutes to hours
– Baby emerges from birth canal, and when breathing adequately on own, the umbilical cord is clamped and severed
Stages of Childbirth (cont ’ d)
• Stage 3: placental stage
– Lasts from minutes to an hour or more
– Placenta separates from the uterine wall and is expelled through birth canal
– Episiotomy is sewn (if performed)
Methods of Childbirth
Methods of Childbirth
• Midwife-assisted childbirth
• Anesthesia-assisted childbirth
• Natural childbirth
• Prepared childbirth
• Doula-assisted childbirth
• Cesarean section
Methods of Childbirth (cont ’ d)
• Midwife delivery
– Delivers baby in woman ’ s home
– More intimate
– Limited access to sophisticated medical instruments and anesthetics that may be needed during a high-risk delivery such as shoulder dystocia or breech birth
Methods of Childbirth (cont ’ d)
• General anesthetics:
– Deaden pain by putting the mother to sleep
– Includes tranquilizers and narcotics
• Local anesthetics:
– Deaden pain without putting mother to sleep
– Pudendal block numbs the mother ’ s external genitals.
– Epidural block and spinal block numb the body below the waist by injecting local anesthesia into the spinal canal or spinal cord.
Methods of Childbirth (cont ’ d)
• Natural childbirth
– Woman uses no anesthesia
• Prepared childbirth
(i.e. Lamaze method)
– Woman is taught breathing and relaxation exercises by a coach who will aid her in the delivery room
Methods of Childbirth (cont ’ d)
• Doula-assisted childbirth
– Doulas provide social and emotional support before and during delivery.
– Doulas may be used when a partner is not available.
– Women with doulas present during birth appear to have shorter labors than those without.
Methods of Childbirth (cont ’ d)
• Cesarean section (C-section)
– Physician delivers the baby by surgery
– Physician cuts through the mother ’ s abdomen and uterus and physically removes the baby
– Mostly used when the health of the baby or mother is at stake during delivery
Birth Problems
Birth Problems
• Prenatal oxygen deprivation (POD)
– Anoxia: absence of oxygen
– Hypoxia: less oxygen than required
• Preterm and low-birth-weight (LBW) infants
– Preterm: born prior to 37 weeks gestation
– Small for gestational age: born at full term, yet low birth weight
• Both conditions can lead to
– cognitive, motor, and psychological problems
Signs of Prematurity
• Preterm babies
– Relatively thin, covered in lanugo and vernix
– Immature muscles
– Weak breathing and sucking reflexes
– May suffer from respiratory distress syndrome (RDS)
– May suffer long-term impairments
Treatment of Preterm Babies
• Preterm babies are kept in incubators
– Maintain temperature controlled environment
– Afforded some protection from disease
– Oxygen has to be monitored because excessive oxygen can cause permanent eye injury
Parents and Preterm Neonates
• Preterm neonates
– look less appealing
– have high-pitched and grating cries
• Parents of preterm neonates
– do not treat preterm neonates as well as full-term neonates
– are more irritable
– can find it so demanding to care for such children that they have depressing effects for mothers
Intervention Programs
• Preterm infants profit from early stimulation.
– Cuddling, rocking, talking, and singing to
– Massage and kangaroo care
• Many positive effects for early stimulation
– Faster weight gain
– Fewer respiratory problems
– Greater advances
The Postpartum Period
Postpartum Period and Maternal Depression
• Some mothers may suffer from postpartum depression (PPD).
– Symptoms
– Causes
– Prevalence
– Treatment
Table 3-2, p. 58
Bonding
• Bonding refers to formation of parent-infant attachment.
• Bonding is essential for the survival and wellbeing of children.
Characteristics of Neonates
Assessing Neonates
• Apgar scale used to assess health of baby at birth
• A) the general a ppearance or color of the neonate
• P) the p ulse or heart rate
• G) g rimace
(the 1-point indicator of reflex irritability)
• A) general a ctivity level or muscle tone
• R) r espiratory effort, or rate of breathing
Table 3-3, p. 60
Assessing Neonates (cont ’ d)
• Brazelton Neonatal Behavioral Assessment
Scale
– Used to measure neonates ’ reflexes and other behavior patterns
• Motor behavior
• Response to stress
• Adaptive behavior
• Control over physiological state
Neonate Reflexes
• Reflexes are simple, automatic, stereotypical responses elicited by certain types of stimulation.
– Demonstrate the neural functioning of neonate
– Absence or weakness of a reflex may indicate immaturity, slowed responsiveness, brain injury, or retardation.
INCLUDE:
• Rooting reflex
• Moro reflex
• Grasping reflex
• Stepping reflex
• Babinski reflex
• Tonic-neck reflex
• Rooting reflex
– Baby turns head and mouth toward a stimulus that strokes the cheek, chin, or corner of the mouth; important for locating mother ’ s nipple in preparation for sucking; can be lost if not stimulated
• Moro reflex
– Back arches, and the legs and arms are flung out and then brought back toward the chest, with the arms in a hugging motion; can be elicited when baby ’ s position is changed or when support for head and neck is lost; can be elicited by loud noises, bumping the baby ’ s crib, or jerking the baby ’ s blanket; lost within 6 to 7 months after birth; absence of Moro reflex indicates immaturity or brain damage
• Grasping reflex (palmar reflex)
– Refers to the increasing tendency to reflexively grasp fingers or other objects pressed against the palms of hands; babies support their own weight this way
• Stepping reflex
– Mimics walking; demonstrated 1-2 days after birth and disappears 3-4 months of age
• Babinski reflex
– Occurs when underside of foot from heel to toes is stroked; toes are fanned or spread
• Tonic-neck reflex
– Observed when baby is lying on its back and turns head to one side
Neonate Sensory Capabilities - Vision
• Infants are nearsighted, seeing best at 7-9 in.
• Can detect movement
– Prefer moving objects to stationary objects
• Have little or no visual accommodation
• See through fixed-focus camera
• Unable to converge their eyes on an object that is close to them
Neonate Sensory Capabilities - Hearing
• Fetuses respond to sound months before they are born.
• Normal neonates hear well unless their middle ears are clogged with amniotic fluid.
• Respond to sounds of different amplitude and pitch
– More to high-pitched sounds than to low-pitched sounds
• Discriminate different and new speech sounds
Neonate Sensory Capabilities - Smell
• Can discriminate distinct odors
• Show more rapid breathing patterns and increased bodily movement in response to powerful odors
• Use smell for mother-infant recognition and attachment
• Neonate ’ s sensitivity
– Neonatal sensitivity to the smell of milk (Macfarlane)
– 15-day-old infants sensitive to the smell of mother ’ s underarm odors vs. odors produced by other milk-producing women
(Porter)
Neonate Sensory Capabilities - Taste
• Show preferences similar to adults
• Discriminate between salty, sour, and bitter tastes, as suggested by reactions in the lower part of the face
• Sweet solutions have a calming effect on neonates.
Neonate Sensory Capabilities - Touch
• Skin on skin
– provides feelings of comfort and security
– may contribute to bonds of attachment between infants and their caregivers
• Many reflexes are activated by pressure against the skin.
Classical and Operant Conditioning of
Neonates
Classical conditioning
• Involuntary responses are conditioned to new stimuli.
• Typical study (Lipsitt)
– Neonates taught to blink in response to a tone
– Indicates they are equipped to learn associations in their environment
Operant conditioning
• Responses can be strengthened through reinforcement
• Typical study (DeCasper, et al.)
– Neonates can be conditioned to suck on a pacifier in such a way to activate a recording of their mothers reading The Cat in the Hat
Neonate Sleeping and Waking
• Most neonates spend about 2/3 of their time in sleep.
– 16 hours per day, not consecutively
• Neonates go through different stages of sleep.
• Typical infant has six cycles of waking and sleeping in a 24-hour period
Sleeping and Waking (cont ’ d)
• Neonates spend about half of their sleeping time in REM sleep, yet will decline as they develop
– By 6 months, REM sleep accounts for only 30% of the baby ’ s sleep
– By 2-3 years, REM drops off to 20-25% of sleep
• Preterm babies spend even more time in REM sleep.
Table 3-4, p. 65
Fig. 3-6, p. 65
Crying
• Babies cry due to pain and/or discomfort.
• Some crying among babies is universal.
• Parents can distinguish between cries of hunger, anger, and pain.
• Infants ’ crying motivates others to take care of them.
Crying (cont ’ d)
• Certain prolonged, high-pitched cries may indicate health problems.
– Chromosomal abnormalities, infections, fetal malnutrition, and exposure to narcotics
• Peaks of patterned crying occur in later afternoon and early evening.
• Response of the caregiver influences crying
• Persistent crying can strain mother-infant relationship
Soothing
• Sucking (breast, bottle, pacifier) has a soothing effect.
• Parents soothe infants by
– picking them up, patting them, caressing and rocking them, swaddling them, speaking to them in a low voice
• How to soothe an infant is learned via trial and error.
• Crying decreases as the infant matures and learns.
Sudden Infant Death Syndrome (SIDS)
• 2,000 to 3,000 annual US infant deaths from SIDS
• Most common cause of death during the first year
– Mostly occurring between 2 and 5 months of age
• More common among the following:
– babies aged 2-4 months
– babies who sleep on their stomachs or sides
– premature and LBW infants
– male babies
– babies from lower SES
– African-American babies
– babies of teenage mothers
– babies whose mothers smoked or used narcotics during or after pregnancy
Children ’ s Hospital Boston Study
• Conducted SIDS study to learn about causes
• Study focused on the medulla ’ s role in sleep/wake cycles
– Compared medullas of babies that died from SIDS to medullas of babies that died from other causes
– Results found SIDS babies ’ medullas were less sensitive to the brain chemical serotonin; boys ’ brains less sensitive
• Prevention includes
– do not smoke during or after pregnancy
– do not use narcotics during pregnancy
– obtain adequate nutrition and health care
– baby needs to sleep on back
– keep current on SIDS data