CP application form
advertisement

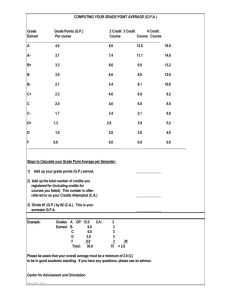
Application for Admission Coordinated Program in Dietetics-(CP) School of Nutrition and Dietetics College of Health Professions The University of Akron Please submit by February 1 Name (Mrs., Miss, Ms., Mr.) Present Address City State Zip Permanent Address City Telephone Home: Email: State Zip Cell: Student ID# To what address should application correspondence be sent? Present address Permanent Address Education: High School City/State Dates Attended Major College/University (List all attended) City/State Dates Attended Major College Awards: Rev. 10/1/15 Page 1 of 8 Recommendations: List the names of all individuals who will complete your recommendation forms (Minimum 2/Maximum 3- At least one must be from an instructor/professor and one from an employer.) Name Title Address Phone Extracurricular/Volunteer Activities: List memberships (specify year(s) of membership), appointed or elected offices you held in organizations. Volunteer activities NOT related to dietetics. __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Paid work experience in the past 3 years (you may include work experience in the past 5 years if applicable to your situation): List paid work experience beginning with the most recent experience. Do not list experiences that were part of required practicum/field experience. Briefly describe responsibilities. (We reserve the right to contact references and work supervisors). Use additional pages as needed. Organization Name City/State Position/ Title Inclusive Dates (Mo./Yr.) Hr./Wk Name and Title of Supervisor/ Phone # 1. Key Responsibilities 2. Key Responsibilities 3. Key Responsibilities Volunteer Experience related to dietetics (food service, community nutrition, etc.) in the past three years: List volunteer experience related to dietetics, beginning with most recent experience. Use additional pages as needed. Organization Name City/State Position/ Title Inclusive Dates (Mo./Yr.) Hr./Wk Name and Title of Supervisor/ Phone # 1. Key Responsibilities 2. Key Responsibilities 3. Key Responsibilities Rev. 10/1/15 Page 2 of 8 Instructions for completion of course work section of application: 1. Complete information about coursework completed or it’s equivalent under each category on the following pages. 2. Specify if you are currently taking a class. 3. To calculate grade point average: i) Enter number of credits for course in Column A. ii) Using the table below, enter the quality points for course in Column B. iii) Multiply Column A x Column B to get Total Points Earned. Enter amount in Column C. iv) Enter totals for Column A and Column C in space provided. Divide Total Points Earned by No. of Credits. Grade A AB+ B BC+ C C- Quality Points 4.0 3.7 3.3 3.0 2.7 2.3 2.0 1.7 College Prerequisite Courses: Lab (X) Grade D+ D+ D D DDF Course No. Term & Year Quality Points 1.3 0.0 (Graduate courses only) 1.0 0.0 (Graduate courses only) 0.7 0.0 (Graduate courses only) 0.0 (Failure) Grade Earned A B No. of Credits Quality Points C Total Points Earned (A x B) If retaken, Previous Grade Earned Microbiology Anatomy and Physiology I Anatomy and Physiology I Lab Anatomy and Physiology II Anatomy and Physiology II Lab GOBC I GOBC I Lab GOBC II GOBC II Lab Statistics Psychology Sociology Accounting Totals: Total Credits in Column A: Total Points Earned in Column C: Grade point average in above courses (divide Total Points Earned by No. of Credits): Rev. 10/1/15 Page 3 of 8 College Lab (X) Course No. Term & Year Grade Earned Nutrition Courses: A B No. of Credits Quality Points C Total Points Earned (A x B) If retaken, Previous Grade Earned Nutrition Fundamentals Career Decisions Nutrition Communication Mgmt Principles & Concepts Intro to Health-Care Mngt Food Science Food Systems Mgmt I Food Systems Mgmt I Clinical Food Systems Mgmt II Human Nutrition Nutrition Assessment Intro to Medical Nutr. Therapy Medical Nutrition Therapy I Nutrition in the Life Cycle Community Nutrition I Community Nutrition II Sports Nutrition Totals: Total Credits in Column A: Total Points Earned in Column C: Grade point average in above courses (divide Total Points Earned by No. of Credits): SAT or ACT Score: (circle one) GRE Score: Date Take: (If Applicable) Date Taken: Verbal: Quantitative: Analytical: Undergraduate Course work: Cumulative grade point average based on 4.0 system: (Total from all schools attended) Grade point average for Nutrition and Prerequisite course work based on 4.0 system: (nutrition total points earned + pre-req total points earned) / (nutrition total credits + pre-req credits) Please respond to each of the following statements: Rev. 10/1/15 Page 4 of 8 1. What is the advantage to you, personally, in participating in the Coordinated Program in General Dietetics? 2. How would you pursue your professional goals if not accepted in the Coordinated Program? 3. Are you acquainted with any practicing dietitians? In what area of dietetics are they employed? 4. With what type of personality do you enjoy working? What type of personality do you find it difficult to work with? Please explain how you are ready to work with those who lack schooling or who are socially or economically deprived. 5. What strengths do you and/or others recognize in your personality? Rev. 10/1/15 Page 5 of 8 6. Participation in the Coordinated Program includes evaluation of student work and progress. How have you handled constructive criticism in the past? Cite an example. 7. It is recognized that each of us, as individuals, learns in different ways. Some prefer reading, self-learning manuals, lectures, etc. Please describe what methods you feel would best promote your learning and retention of concepts and skills in the science and art of dietetics. Rev. 10/1/15 Page 6 of 8 Application Requirements Coordinated Program in Dietetics Initial each statement verifying your understanding: ______I understand I must successfully complete all of the first two-year course requirements prior to the academic year in which admission to CP is requested. ______I understand I must include an official transcript (un-opened and mailed directly to Program Director) of all my grades through the past fall. ______I understand my GPA must be at least 3.0 on a 4.0 scale. ______I understand I must have completed 60 shadowing hours with a dietitian or approved alternate. ______I understand I must calculate my prerequisite and nutrition grade point averages according to directions provided. ______I understand I must attach a photocopy of my ACT or SAT Scores. If I am a post baccalaureate or graduate student, I have attached a copy of my graduate transcript. ______I understand I must include a maximum of three letters of recommendation; at least one from an employer and one from an instructor. ______I understand all letters of recommendation must include a signed waiver. ______I understand I must meet with the Academic Advisor and include a copy of my academic agreement in my application. ______I understand that I must complete a writing lab during the scheduled day and time. ______I understand that I must complete an interview during the scheduled day and time. ______I understand that if I am an international student, I must provide a TOEFL, or Michigan Test Score as an objective measure of English as a foreign language. ______I understand that if I am a transfer student from another institution or from another college within The University of Akron, I have applied to The College of Health Professions and have included The University College Evaluation of my courses. (Transfer students should allow at least six weeks to receive evaluations). ______I understand that I must pass a background check in order to be in the Coordinated Program. ______I understand all the steps in the application process for The University of Akron Coordinated Program. Rev. 10/1/15 Page 7 of 8 Program Requirements Coordinated Program in Dietetics Initial each statement verifying your understanding: If accepted into The University of Akron Coordinated Program in Dietetics…. ______ I understand I must assume the expense of Health Insurance (if not already covered) and Liability Insurance for the length of the program; and will have verification by the beginning of the fall term. (Applications provided when accepted into the program). Please allow at least eight weeks for processing. ______I understand I must take the prescribed medical examination required by affiliated agencies. (Forms provided upon acceptance into the program). ______I understand if I have any extenuating circumstances (physical conditions, etc.) that should be considered I must submit a separate sheet describing. ______I understand it is my responsibility to assume the expense of CP Clinical lab fees, uniforms, name tags, transportation costs to and from the clinical sites and any other incidental expenses associated with the program. All information provided in this application is true and accurate and recognize that any false or incorrect statements made herein will be grounds for my dismissal from the program. Signature Rev. 10/1/15 Date _________________ Page 8 of 8