O Obese Zucker rat Opportunistic infection
advertisement

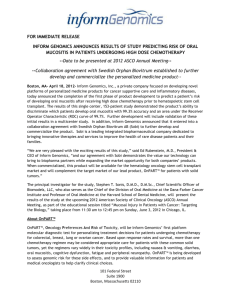
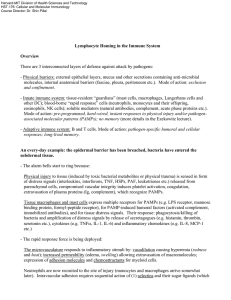
O 3 Oily Fish Species of fish which store fat throughout their flesh (for example salmon, herring and mackerel)s. Fatty Acids and the Immune System 3 Oliguria A urine volume insufficient to sustain life, usually less then 400 ml per 24 hours. Septic Shock Opsonin A molecule that binds to antigen and phagocyte to enhance phagocytosis. C3b and C4b along with their degradation products are opsonins derived from the complement system. Immunoglobulins also function as opsonins. Complement, Classical Pathway/Alternative Pathway Opsonins All factors by which bacteria or other microorganism are altered by the attachment to the surface so that they are more readily and more efficiently engulfed by phagocytes, are collectively called Opsonins. Respiratory Infections 3 Organization for Economic Co-operation and Development, an international organization helping governments solve the economic, social and governance challenges of a globalized economy. Testing guidelines of the OECD recommend procedures for testing chemicals. Immunotoxicology 3 3 OECD Infections with bacteria, viruses, fungi, or protozoa to which individuals with a normal immune system are not usually susceptible. That is, infections that are caused by microbes that are not very infectious, but that can be so when the normal immune system is not functioning properly. Lymphoma Leukemia 3 Diabetes and Diabetes Combined with Hypertension, Experimental Models for Opportunistic infection 3 Obese Zucker rat 3 Opsonization Oncogenes Mutated genes that are the cause of a cancer. The normal gene is called the proto-oncogene. These genes are usually involved in the regulation of cell growth or survival or the intermediate steps in those processes. Lymphoma Leukemia Phagocytosis of microorganisms such as bacteria can be enhanced by binding of antibodies, complement factors (mainly C3b), or blood plasma proteins, which are also collectively termed opsonins. These endogenous proteins cover a pathogen and thereby make it “visible” for sentinel cells (macrophages, dendritic cells, or neutrophilic granulocytes) which posses specific receptors for the opsonins. 3 3 Opsonization and Phagocytosis 3 3 3 3 Opsonization and Phagocytosis Charles J Czuprynski Department of Pathological Sciences University of Wisconsin 2015 Linden Drive W Madison, WI 53706 USA dies) that are specific for antigenic determinants on that organism, or with complement proteins (particularly C3b) deposited on the surface of the organism via either the classical or alternative activation pathways. The presence of these plasma proteins on the surface of the microbe facilitates their sequential interaction with immunoglobulin receptors (Fc receptors) or complement receptors (CR) on the phagocyte surface. These interactions result in encirclement of the particle by the cytoplasmic membrane of the phagocytic cell, until the particle is contained within a membrane-bound vacuole (phagosome) within the cell. 3 Immune Response Fish Immune System Complement Deficiencies Streptococcus Infection and Immunity 3 488 Characteristics In general, the term phagocytosis refers to ingestion of microbes or other particles by professional phagocytic cells. These include granulocytes (principally neutrophils) and monocytes in the bloodstream, and mononuclear phagocytes ( macrophages) that are distributed throughout the various tissues of the body. Opsonization of a microbe by immunoglobulins (antibodies) reflects a specific immune response against antigenic epitopes on that microbe, as a result of natural infection or immunization, or a cross-reaction with antibodies against related antigens. Activation of the complement cascade on the surface of the microbe via the classical pathway, occurs following binding of certain immunoglobulin isotypes (usually IgG) to the surface of the microbe. This event leads to deposition of the C1 complex, which has C3 convertase activity and cleaves C3 to C3b on the surface of the microbe. The alternative pathway of activation occurs when a different C3 convertase (composed of C3 and factor B) forms on the microbial surface. Once the IgG or C3b are deposited on the microbial surface, they can interact with specific receptors (Fc and CR, respectively) on the cytoplasmic membrane of phagocytic cells. There are subtypes of both receptors present on various leukocyte populations, that may demonstrate either activating (immunoreceptor tyrosinebased activation motif or ITAM) or inhibitory (immunoreceptor tyrosine-based inhibition motif, or ITIM) activity. Other plasma proteins that have been reported to opsonize and facilitate ingestion of particles by phagocytic cells include fibronectin, fibrinogen, and Creactive protein. The interactions amongst plasma proteins and phagocytic cells provides the critical first line of cellular defense in innate immunity against microbial infection. Once it is internalized within the phagosome, the vacuole becomes acidified and the ingested microbe will be exposed to a variety of antimicrobial compounds. These include reactive oxygen intermediates and nitrogen intermediates that are produced in response to activation of ITAM-containing Fc receptors, and antimicrobial proteins and peptides (e.g. lysozyme, defen3 ingestion, uptake, internalization Definition Opsonization is the process by which a foreign particle, particularly a microbe, is coated with plasma proteins (opsonins) so as to facilitate the attachment and internalization of that particle by a professional phagocytic cell. In general, the process refers to coating of the microbe with immunoglobulin molecules (antibo- Opsonization and Phagocytosis. Figure 1 Simplified overview of how opsonization with IgG and C3b facilitates phagocytosis, phagolysosome formation, and release of reactive oxygen intermediates, defensins and other microbicidal peptides into the phagolysosome. 3 Synonyms Oral Mucositis and Immunotoxicology sins) that are present in preformed lysosomal granules in the phagocytic cell. Following granule fusion, the phagosome is referred to as a phagolysosome. Most microbes cannot survive in the hostile environment of the phagolysosome. Intracellular pathogens have evolved strategies to circumvent formation of this hostile environment (e.g. inhibition of phagosome acidification or phagolysosome formation), or resistance mechanisms to the toxic compounds contained within the phagolysosome (e.g. production of catalase or superoxide dismutase to scavenge reactive oxygen intermediates). Preclinical Relevance Experimental assessment of the effects of potential toxicants on innate immunity would include concerns about inhibition of the ability of the exposed individual to produce immunoglobulins that can opsonize pathogenic microbes, and the ability of their granulocytes and mononuclear phagocytes to ingest and kill the opsonized microorganisms. Various simple assays can be performed to assess phagocytosis of bacteria, yeast cells, or other particles. Opsonins (e.g. serum as a source of immunoglobulins and complement) might be added to facilitate evaluation of the phagocytic function of granulocytes and mononuclear phagocytes. Fluorescent beads (either opsonized or uncoated) can be used to evaluate phagocytosis by microscopy or flow cytometry. 489 duction of immunoglobulins or other plasma proteins required for opsonization of microbes. Although assessment of opsonization is not frequently done in a regulatory situation, production of immunoglobulins, as assessed either by ELISA or a plaque-forming cell assay, is heavily relied upon for assessment of potential immunotoxicants. If a weak antibody response occurred following toxin exposure, it might indicate a potential for decreased resistance against extracellular pathogenic microbes that must be opsonized, ingested, and killed by phagocytic cells. The draft EPA Health Effects Test Guidelines (OPPTS 870.1350) for Acute Inhalation Toxicity with Histopathology include assessment of phagocytic activity by alveolar lavage macrophages using a fluorescent bead assay and microscopy. References 1. Aderem AA, Underhill DM (1999) Mechanisms of phagocytosis in macrophages. Ann Rev Immunol 17:593–623 2. Janeway CA, Travers P, Walport M, Shlomchik M (2001) Immunobiology. Garland Publishing, New York, pp 24, 39–40, 49, 55–56, 371–373 3. Rosenberger CM, Finlay BB (2003) Phagocyte sabotage: disruption of macrophage signaling by bacterial pathogens. Nat Rev Mol Cell Biol 4:385–396 Oral Mucositis and Immunotoxicology Relevance to Humans Phagocytic cells are essential for innate immunity against microbial infection. Individuals afflicted with genetically determined defects in their phagocytic cells often experience significant problems in controlling infectious agents. In some instances, the defect may be of sufficient severity to cause repeated severe infections or premature death. There is concern that toxicants in the environment might alter the ability of humans to produce, mobilize, and regulate the activity of these phagocytic cells, and by so doing render individuals susceptible to infectious diseases. An additional concern for inhaled particulate toxicants is that their ingestion by phagocytic cells in the lung might elicit release of inflammatory mediators (e.g. cytokines, eicosanoids) that could damage nearby cells, or attract inflammatory leukocytes that trigger hypersensitivity responses. Regulatory Environment Assessment of phagocytic cells is not universally required as part of the assessment of immune function. Nonetheless, it is frequently listed on tiers of immune function assays, and its assessment may be prudent or required if the compound in question is known to have an adverse effect on phagocytic cells, or on the pro- Gary J Rosenthal Drug Development RxKinetix Inc. 1172 Century Drive, Ste # 260 Louisville, CO 80027 USA Synonyms Mucositis, stomatitis, ulcerative mucositis, ulcerative stomatitis, radiation mucositis, oral ulcer Definition Oral mucositis is a frequent toxicological complication of high-dose chemotherapy as well as head and neck radiotherapy. This insidious condition manifests as inflammation of the moist mucosal lining the mouth and back of the throat and ranges from redness to severe ulceration over vast portions of the region. Symptoms of oral mucositis vary from local pain and discomfort to the inability to chew and/or swallow food or fluids, or to communicate. Characteristics Oral mucositis induced from either chemotherapy or O 490 Oral Mucositis and Immunotoxicology radiotherapy is characterized by painful and often incapacitating ulcerative lesions of the oropharyngeal mucosa (1). Chemotherapy-induced mucositis often presents as lesions involving the buccal and tongue mucosa, the soft palate, and the floor of the mouth. In contrast to this broad area of injury associated with chemotherapy, patients being treated for head and neck cancers with ionizing radiation manifest mucositis on those oral mucosal sites that lie in the direct path of radiation beam. The targeted oropharyngeal mucosa is lined by mucus membranes with a high mitotic index and is exceptionally sensitive to the antiproliferative effects of chemotherapy and radiotherapy. At the tissue and cellular level, oral mucositis manifests initially as hypoplasia and destruction of superficial epithelial cells along with a lack of cell renewal. The subsequent erythematous areas proceed to desquamation and eventually ulcers covered by an exudate. From the host defense perspective, cancer treatment and resultant oral ulcers serve to weaken the defense system of the lining of the mouth leading to marked local infections. In addition, the potential for systemic infection due to opportunistic and acquired oral flora has been documented in cancer patients. This further complicates the already challenging health status of immunosuppressed patients where morbidity and mortality due to infection is of prime concern. While not considered life-threatening to the extent that chemotherapy-induced myelosuppression has historically been, oral mucositis is often identified by cancer patients as the single worst side effect of therapy. Symptoms may be so severe that they may limit a patient’s ability to tolerate their chemotherapy or radiotherapy, resulting in delayed or shortened treatment and limited efficacy (2). The early understanding of mucositis was of a disorder that simply resulted from non-specific toxicity of chemotherapy or radiotherapy against the basal epithelium. More recent research has broadened our understanding to suggest a more complex pathology with multifaceted interactions between connective tissue, endothelium and epithelium, myelosuppression and the oral microenviroment. A conceptual model for oral mucositis outlining the probable pathophysiology was published by Sonis in 1998 (3). In this model, mucositis is broken down into four phases (also see Figure 1): * inflammatory/vascular phase * epithelial phase * ulcerative/bacteriological phase * healing phase. Inflammatory/Vascular Phase In this early phase, chemotherapy or radiotherapy directly or indirectly induce events leading to local inflammatory events, including reactive oxygen-induced cell damage, NF-κB/early response gene activation, and proinflammatory cytokine induction, all of which serve as a foundation for local tissue damage and initiate the events leading to development of mucositis. Epithelial Phase Dividing cells of the epithelium begin to atrophy and cell renewal is diminished in the face of any continued antiproliferative cancer therapy. Inflammatory events serve to augment the negative effects of tissue destruction. Ulcerative/Bacteriological Phase This is generally considered to be the most symptomatic phase with ulcerative erosions of the mucosa and an altered opportunistic microbial microenviroment. Healing Phase This involves renewal of the epithelial cell population, re-establishment of microbial homeostasis and local immune function. While oral mucositis is biologically complex and progresses as a continuum of these phases, the depiction outlined by Sonis in 1998 allows a focus on the characteristic and likely primary events of the disorder as it progresses from initiation to healing. Research conducted over the last 5 years (4,5) has served to add support for the model put forth by Sonis and elucidates in greater detail the cellular and subcellular events associated with oral mucositis. Considering the involvement of reactive oxygen species (ROS) in mediating other manifestations of chemotherapy or radiation toxicity, it seems likely that ROS play a role in the initiation and progression of mucosal injury (5). Preclinical Relevance Oral mucositis remains under extensive laboratory investigation. Animal models of mucositis have been developed in a variety of species using radiation alone or both chemotherapy and radiation protocols. Possessing a cheek pouch accessible to treatment and observation, the hamster has provided much of the currently available preclinical information, though rodents have also been used with some success. Critical understanding into the roles of mucosal immune dysregulation and wound healing are imperative areas of preclinical research that will improve prospects for effective prophylactic or treatment strategies. Relevance to Humans Myelosuppression was previously the major dose-limiting toxicity associated with of cancer therapies. With therapeutic advances in the 1980s relative to infection prevention and reduced myelosuppression via growth factors such as granulocyte colony stimulating factor Oral Ulcer 491 Oral Mucositis and Immunotoxicology. Figure 1 A conceptual model for oral mucositis outlining the probable pathophysiology. Adapted from Sonis (1998). Regulatory Environment A plethora of approaches have undergone clinical assessment around the world with no single approach showing any consistent benefit. Currently no medication is approved by the Food and Drug Administration (FDA) to prevent or treat oral mucositis. While clinical trials investigating a variety of novel approaches continue, most patients and clinics manage symptoms with morphine or other narcotic analgesics, with mouth rinses, changes in diet, and cold liquids. The FDA recognizes that oral mucositis is a serious illness that needs to be addressed expeditiously and as such has granted Fast Track designation to some candidate therapeutics in clinical development. Fast Track designation is intended to expedite the regulatory re- view and approval process for a product and claim that addresses a significant unmet medical need. References 1. Berger AJ, Kilroy TJ (1997) Oral complications. In: Devita VT, Hellman S, Rosenberg SA (eds) Cancer Principles and Practice of Oncology, 5th ed. Lippincott Williams & Wilkins, Philadelphia, pp 2714–2725 2. Ohrn K, Sjoden P, Wahlin Y, Elf M (2001) Oral health and quality of life among patients with head and neck cancer or hematological malignancies. Supp Care Canc 9:528–538 3. Sonis ST (1998) Mucositis as a biological process: a new hypothesis for the development of chemotherapy-induced stomatotoxicity. Oral Oncol 34:39–43 4. Sonis ST, Scherer J, Phelan S et al. (2002) The gene expression sequence of radiated mucosa in an animal mucositis model. Cell Prolif 35 (Suppl 1):93–102 5. Blonder JM, Etter J, Samaniego A et al. (2001) Topical bioadhesive antioxidants reduce the severity of experimental radiation induced oral mucositis. Proc Amer Soc Clin Oncol 20:1606 Oral Ulcer 3 (G-CSF), thrombopoietin and erythropoietin, non-hematologic toxicities have now become significant dose-limiting concerns. Of these non-hematologic toxicities, oral mucositis has emerged as one of the most problematic toxicities associated with current therapeutic regimens with direct impacts on cure rates and long-term survival (2). Considering the frequency of oral mucositis, which is determined by the type of cancer therapy ( e.g. approximately 40% in patients treated with systemic chemotherapy to nearly 100% of patients treated for head and neck cancer), this unmet clinical need remains an active area of clinical investigation. Oral Mucositis and Immunotoxicology O Organ-Specific Autoimmunity Organ-Specific Autoimmunity Autoimmune disease which affects a single organ in the body such as the pancreas in type 1 diabetes. Systemic Autoimmunity Oryctolagus cuniculus 3 492 Rabbit Immune System 3 Oxidative Stress Organogenesis The formation of the various organs of the body from embryonic tissues during gestation. Developmental Immunotoxicology 3 Organotypic Murine or Human Skin Explant System Oxidants released by phagocytes such as neutrophils or macrophages play an important role in early immune defense against pathogens. Free radicals are any atom that contain one or more orbital electrons with unpaired spin states. Some radical species are very reactive with other biomolecules (proteins, DNA) and others, like the normal triplet state of molecular oxygen, are relatively inert. Cells have multiple protective mechanisms against oxidative stress, e.g. protective agents like antioxidants to prevent cell damage. Rodents, Inbred Strains 3 Three-Dimensional Human Skin/Epidermal Models and Organotypic Human and Murine Skin Explant Systems 3 Oxy-PAH A birth defect in which the palate and/or associated structures fail to close along the midline during fetal development. Cleft palate is an orofacial cleft defect. Birth Defects, Immune Protection Against 3 Orofacial Cleft Polycyclic Aromatic Hydrocarbons (PAHs) and the Immune System 3