10 Medical History and Physical Examination in Parkinsonian Syndromes
advertisement

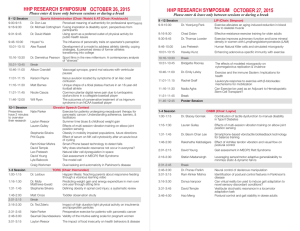
Medical History and Physical Examination 155 10 Medical History and Physical Examination in Parkinsonian Syndromes How to Examine a Parkinsonian Syndrome Marie Vidailhet, Frédéric Bourdain, and Jean-Marc Trocello The current chapter was prepared to help clinicians examine patients with parkinsonian syndromes and to detect clinical signs and clues that should alert to the appropriate diagnosis. For the main clinical diagnosis criteria of various parkinsonian syndromes (Parkinson’s disease [PD], multiple system atrophy [MSA], progressive supranuclear palsy [PSP], corticobasal degeneration [CBD], and dementia with Lewy bodies [DLB],), the semiology will be detailed. The validity and reliability of these criteria will not be touched upon, as they were extensively reviewed recently in a reference paper by Litvan and colleagues (1). We will consider (a) medical history and clinical description of the cardinal signs and helpful clues and (b) how they relate to the established diagnostic criteria of various parkinsonian syndromes. PARKINSONISM Major signs are resting tremor, rigidity, akinesia, and postural instability (2). Advanced PD rarely presents a diagnostic problem, but careful medical history and clinical examination is necessary at an early stage of a parkinsonian syndrome and in very old patients, especially because of other superimposed neurological or non-neurological disturbances (vascular lesions, musculoskeletal disease, vision and auditory problems). Interview of Patient and Spouse or Family • Lack of spontaneous gestures and smiling commented on by the family. • Slowing of activities of daily living with increase in the length of time needed to get up and to get dressed, difficulties using the involved hand (buttons, toothbrush, lack of dexterity), slowness of gait, dragging of the involved leg, stooped posture; and insidious, and progressive and mistaken by the patient as related to “normal aging.” • Difficulties in sports (altered tennis and golf swing, lack of coordination while swimming). • Micrographia and slowness of handwriting (the size of the handwriting progressively decreases after a few words or sentences in patients with PD; there is a fast micrographia with small letters from the beginning in PSP patients). • Uncomfortable sensation of fatigue, tightness, stiffness of the limbs. From: Current Clinical Neurology: Atypical Parkinsonian Disorders Edited by: I. Litvan © Humana Press Inc., Totowa, NJ 155 156 Vidailhet, Bourdain, and Trocello • Mild depression and withdrawal. • Resting tremor when sitting in an armchair or while walking. • Miscellaneous: profuse sweating or dry skin; sleep disturbances; daytime sleepiness; pain, numbness, or tingling in the limbs; shoulder arthralgia; radiculopathy. In all cases, the examiner has to obtain a complete drug history as drug-induced parkinsonism and PD can present with the same clinical signs. Clinical Examination Tremor The 4–5 Hz tremor is most apparent when the arm is fully relaxed (supported and at rest, in an armchair). It is increased by mental calculation and stress and best seen during walking. It is reduced by action and intention (tricks used by the patients to hide the tremor). The classical description is the “pill-rolling” rhythmic alternating opposition of the thumb and forefinger. Some patients have postural tremor in particular conditions (holding a phone) with a different frequency (6 Hz). Bradykinesia This is the most disabling feature in PD as it involves the whole range of motor activity with a decrease in amplitude and rhythm of movement. Automatic movements disappear. Bradykinesia is well explored in the motor items of UPDRS III, the Unified Parkinson Disease Rating Scale (finger tapping, alternating pronation/supination movements, foot tapping, etc.), with rapid decline in amplitude and frequency. Rigidity Abnormal tone is observed when the patient is relaxed and the limb passively flexed and extended. Passive circling movements are better to test rigidity, as the patient cannot voluntarily “help” the passive movement (whereas active movement is sometimes superimposed to the passive movement during simple flexion–extension movements). The Froment sign is classically described as an increase in tone of the limb during contralateral active movements. The actual sign, described by Jules Froment, was an increase of tone in the examined limb as the patient bent to reach a glass of water on the table (both postural adaptation and voluntary movement of the contralateral limb). The cogwheel phenomenon is not pathognomonic of PD or parkinsonism and reflects the underlying tremor (can be observed in severe and disabling postural tremor) (2,3). Impairment of Postural-Reflexes This is observed when the patient moves spontaneously (rising from a chair, pivoting when turning, etc.). The patient will take extra steps in pivoting and may have a careful gait. Postural challenge consists of a thrust to the shoulders (the examiner stays behind the patient to prevent a fall and the patient is instructed to resist the thrust). According to the UPDRS III score, one can observe a retropulsion (more than one step backward), but the patient recovers unaided (score 1); absence of postural response, the patient would fall if not caught by the examiner (score 2); the patient is very unstable, tends to lose balance spontaneously (score 3); the patient is unable to stand without assistance (score 4). This pull test is not standardized and each neurologist has his or her own technique. As a consequence, the examiner may adapt (consciously or not) the intensity of the thrust to the expected reaction of the patient! (see video segment 1.) Only scores 0 (normal) and 1 are observed in PD until a later stage. In contrast, early postural instability is observed in MSA (with walking difficulties) and particularly in PSP (cardinal sign). Spontaneous falls (without warning or obstacle, occasional then frequent) occur in PSP (4) with loss of anticipatory postural reflexes, reactive postural responses, or rescue and protective reactions (the patient does not use his arms to keep balance and does not throw out his arms to break the fall and protect the head from injuries). Medical History and Physical Examination 157 Gait Disorders At an early stage of parkinsonism, slowing and shuffling of gait with dragging of the affected limb is common. A flexed posture of the arms (unilateral then bilateral) with a loss of arm swing is observed. In contrast, in “vascular” parkinsonism or normal-pressure hydrocephalus, the arm swing is preserved or even exaggerated (to keep the balance) and the arms are not flexed. In that case, “parkinsonism” predominates in the lower limbs (thus the name of “lower body parkinsonism”). The “marche à petits pas” described by Déjerine is suitable for the description of these patients. The gait is characterized by short quick steps, initially without dragging or shuffling the feet on the ground (in contrast to PD), with start and turn hesitation (take several steps on turning), slight wide base (but can be narrow), and moderate disequilibrium (described by Nutt and colleagues as “frontal gait disorder”) (5). Visual clues (contrasted lines on the ground) do not help these patients (in contrast to PD). The diagnosis of vascular origin (differential diagnosis from degenerative parkinsonism) is made by the company it keeps: pyramidal signs, dysarthria and pseudo-bulbar signs, urinary disturbances, cognitive signs, and stepwise progression with past medical history of acute motor deficits. In time, patients may develop a magnetic gait (the feet are glued to the ground) and astasia-abasia (they do not know how to walk anymore). Overall, the gait is different from those of patients with late PD or even PSP or MSA. Gait disorders in PSP have been described as “subcortical disequilibrium.” This gait pattern is characterized by a severe postural instability, loss of postural reflexes (cf. supra), and inappropriate response to disequilibrium (e.g., when rising from a chair, the patient will extend the trunk and neck and fall backward). The gait is also impaired by the disequilibrium, and is characterized by a wide base. Some patients do not hesitate to walk briskly, and are careless of the risk of falls (as if they did not realize they were in danger of falling). Freezing and gait ignition failure are defined by a marked difficulty with initiating gait and difficulties maintaining locomotion in front of various obstacles (door, modification of the pattern of the floor, turning). They are observed at a late stage in PD or at earlier stages in MSA patients. They may be associated with various gait disturbances. Pure gait ignition failure is a different disorder, still poorly defined and, to date, with few clinical-pathological correlations (mostly associated with PSP). In summary, a parkinsonian syndrome is easily explored, and may take only a few minutes. Spontaneous movements (or the lack of them) are observed when the patient and spouse are providing the medical history. Clumsiness and slowness are detected when patients are searching for documents or glasses in their bag, and when they take off or put on their jacket and shirt (buttons). Writing a few sentences will demonstrate the micrographia; walking in the examination room or corridor will help to detect a resting tremor, loss of arm swing, flexed posture, general slowness, and difficulties of gait and turning. The pull test will explore postural instability. In the end, the UPDRS III motor score will give a quantification of the severity of the parkinsonian syndrome. FRONTAL SYNDROME Clinical Examination: Utilization and Imitation Behaviors (Video Segment 2) The classic signs of frontal syndrome are usually well known. Distractibility and attentional disturbances are easy to detect when several people are present in addition to the patient and the examiner. Therefore, it is very important that all of them remain completely neutral and indifferent toward the patient, and do not react during the clinical examination. As described by Lhermitte “the test begins with the solicitation of manual grasping behavior.” The examiner places his or her hands on the patient’s palms and stimulates them with slow and rapid rubbing movements. A bilateral grasping reflex is obtained, even if the patient is instructed not to 158 Vidailhet, Bourdain, and Trocello take the hands of the examiner. Moreover, the patient holds the hands so tightly that the examiner can lift the patient from the chair. Then, while the hands of the patient are free, the examiner displays various objects in the field of vision of the patient. The patient may grasp the object and collect as many objects as he or she can hold (collectionism). Moreover, he or she usually starts to use them in a proper manner (utilization behavior) (6). When the patients are asked why they took them and used them, the answer is “because I thought I had to take them and use them.” Normal subjects do not react this way. Moreover, even when the examiner tells the patient “whatever I do, do not imitate me,” the patient will still do it, all the same. The patient may copy funny behaviors, with or without actual objects (imitation behavior) (7). When asked why they imitated the examiner, they answer, “Because I thought I had to imitate.” Again, a normal subject never imitates the examiner (except to make fun of him!). These tests are very sensitive, easy to do at the bedside and take only a few minutes. EYE MOVEMENTS Bedside Examination (Video Segments 3 and 4) The patient may complain of problems with visual acuity as they cannot read properly anymore. Several pairs of glasses have been changed unsuccessfully. The upward- and downward-gaze impairment are rarely detected by the patient. In contrast, the family will observe “a reptilian” gaze, with a staring and terrified look. The bedside examination will mainly explore the visually guided saccades in four directions (up, down, left, and right). The targets should be at a certain distance (arm length). The best way to have the right distance and to prevent movements of the head is to hold the chin of the patient at arm length. The targets should be clearly visible (colorful balls or pens). The midline target should be neutral (e.g., the switch of the light) and the lateral should be 25° from the midline target. Voluntary saccades are made after verbal instruction: “look at the switch,” “look at the red pencil.” Note the time taken to initiate the saccade, its speed, and its amplitude (the target is reached with the initial saccade or correction with additional small saccades are needed). In normal subjects, the displacement of the eyes cannot be detected by the examiner (who sees the initial and the final positions of the eyes). Any perception of the displacement (like in oil) is abnormal. People usually focus on vertical gaze (because of the diagnostic criteria of PSP). However, horizontal saccades are impaired at a early stage of the disease and bedside examination can also detect this abnormality. In summary, as Drs. Leigh and Riley stated, “it is saccadic speed that counts and the key finding is slowing of the saccade” (8). This can be observed before reduced amplitude is detected. Testing visual pursuit is not very useful as pursuit is frequently altered (including by drugs). Moreover, testing pursuit is testing the velocity of the target, more than those of the eyes. Vestibular ocular reflexes (VORs) are normal in PSP patients, by definition (supranuclear palsy). In summary, eye movement examination is very helpful for the diagnosis of PSP (9), and does not help as much for PD or MSA. Useful clues are: • Slowing of vertical or horizontal saccades. • Decreased amplitude of saccades (vertical and/or horizontal). Several small and slow saccades are needed to reach the target (steplike displacement of the eyes). • Square-wave jerks can be observed in the neutral (central position), and better seen through the use of an ophtalmoscope (small movements take the eye away from the fixation point). • Patients often blink before they move their eyes when they have mild supranuclear gaze palsy, or they use their VOR (vestibular ocular reflex) to help movement of the eyes at more severe stages. • In all cases, the VORs are normal. Although pathologically proven cases of PSP without “abnormal eye movements” have been described, eye movements were usually not quite “normal.” Indeed, these patients did not have a Medical History and Physical Examination 159 downward oculomotor palsy, but Birdy and colleagues (10) observed that they had a slowed downward-command saccades, square-wave jerks, slow horizontal saccades, and blepharospasm. This should be considered probable PSP, even if the best specificity for PSP (NINDS-SPSP) criteria are postural instability leading to falls within the first year of onset coupled with a vertical supranuclear gaze paresis (1,4). DYSAUTONOMIA Dysautonomia is characterized by urogenital and/or orthostatic dysfunction. Orthostatic hypotension is defined by an orthostatic fall in blood pressure by 20 mmHg systolic or 10 mmHg diastolic, but a 30-mmHg systolic or 15-mmHg diastolic is required for the consensus diagnosis criteria by Gilman (11). Although this is considered to be a frequent and early sign in the disease (12,13), it is rarely symptomatic (syncope or faintness), and autonomic nervous system testing may not distinguish MSA from PD (14). Urinary disturbances often appear early in the course of the disease, or are a presenting symptom (impotence common in men). Urinary incontinence (70% of MSA) or retention (30%) may be detected by medical history, leading to more refined explorations. MSA, PSP, as well as PD patients complain of urgency, frequent voiding, or dysuria. Some describe difficulties voiding but are not aware of chronic urinary retention. Incontinence is never observed in patients with PD and rarely in late stages in PSP. In all cases, additional laboratory tests such as urodynamic tests and sphincter electromyogram (EMG) may make the association between urinary symptoms and urinary tract denervation (13). Patients with PD have less severe urinary dysfunction, by contrast with these common findings in MSA. However, sphincter EMG does not distinguish MSA from PSP. In summary, the detection of autonomic and urinary features by medical history and, if necessary, laboratory tests, may be a good clue at early stages of the parkinsonian syndrome, but the diagnosis should take into account other clinical clues to reach the diagnostic criteria for PD, MSA, or PSP. HALLUCINATIONS Most of the time, the patient does not spontaneously report hallucinations and only a small portion of them are detected by the spouse (emerged part of the “iceberg”). Patients should be specifically questioned on the presence of minor, visual, and auditory hallucinations. As reported by Fénelon and colleagues, (15) the most frequent type are visual hallucinations. The patient has a vivid sensation of the presence of somebody either somewhere in the room or, less often, behind him or her. The presence is often a relative (alive or deceased) who is often perceived as benevolent like a “guardian angel.” However, the patient is ready to accept that the “presence” is not real. Formed visual hallucinations are more complex with vivid scenes “like a film,” sometimes close to real (members of family), sometimes full of fantasy (ninja turtles, dancing Russians, medieval stories), but soundless. In some cases, the hallucinations may be frightening (house burning, wild animals). Auditory hallucinations are rare and tactile hallucinations often involve animals. As they are more frequent in the evening they may be associated with vivid dreams and sleep disorders (15). In all cases, the main risk factor for hallucinations is cognitive impairment. Therefore, it is important to detect them as they are among features used for the diagnostic criteria of dementia with Lewy bodies (DLB) in addition to cognitive impairment, attentional and visuospatial deficits, fluctuating cognition, and parkinsonism (16). MOVEMENT DISORDERS Dystonia Dystonia associated with parkinsonian syndromes is often manifested by dystonic postures (video segments 5 and 6) more than abnormal movements and they are rarely modified by a “geste 160 Vidailhet, Bourdain, and Trocello Fig. 1. Clinical examination at a glance from head to feet. antagoniste.” They include limb dystonia (from writer’s cramp to a dystonic posture of the arm or foot), blepharospasm (and/or eyelid apraxia), orofacial dystonia, stridor, axial dystonia, and cervical dystonia. Axial dystonia is sometimes difficult to differentiate from rigidity, especially in the neck. In cervical dystonia, torticollis, retrocollis, or laterocollis are easy to define but antecollis can range from severe bent neck (considered to be a good clue for MSA) to abnormal neck flexion; in such cases, cervical dystonia can be found in up to 25% of MSA patients (17) and in most PSP patients (18). As a rule of thumb, dystonia predominantly affects cranio-cervical musculature in MSA and PSP, although limb dystonia may be observed in PSP (leading to misdiagnosis of CBD). In fact, in CBD, the best predictors for the diagnosis are limb dystonia, ideomotor apraxia, myoclonus, asymmetric akinetic-rigid syndrome with late-onset gait or balance disturbances (19). Levodopa-induced dyskinesias are observed in PD but are not infrequent in MSA. In MSA the presence of painful, dystonic, postural as well as orofacial and cervical dyskinesias are good clues for its diagnosis. Myoclonus Myoclonus is sometimes difficult to differentiate from irregular tremor by clinical examination. Stimulus-sensitive myoclonus is elicited by either pinprick or light touch of the skin. It can be observed in MSA and in CBD patients. In PD patients, myoclonus is rare and may be related to levodopa (levodopa-induced myoclonus). Electrophysiologic testing helps to differentiate the stimulus-sensitive myoclonus in CBD with a pattern characteristic of cortical myoclonus (20) (video segments 5 and 6). CONCLUSION: EXAMINATION AT A GLANCE Very simple tests will help to get the most out of the clinical examination and medical history. This is particularly true for the bedside neuropsychological examination and eye movement exploration, which appear complicated but are not (video segments 3 and 4). Moreover, a refined and precise Medical History and Physical Examination 161 evaluation will increase the accuracy of the diagnostic criteria in clinico-pathological studies. For example, the precision of the information in the “clinical vignettes” is of great importance. This may allow clinicians to rename probable criteria into clinically definite or clinically probable. This high specificity of criteria is important for research studies, especially genetics or therapeutic studies. As a rule of thumb, we suggest examining the patient “from head to feet” (see Fig. 1) in order to check all the diagnostic features included in the criteria for PD, MSA (video segment 7), PSP (video segments 1–4), CBD (video segments 5 and 6), and DLB. VIDEO LEGENDS Video 1: Corticobasal degeneration with myoclonus. Right upper limb dystonia with shoulder abduction, and elbow + wrist + fingers flexion, associated with myoclonic jerks (at rest and triggered by posture and action). Polygraphic EMG recordings show brief and synchronous bursts on the upper arm muscles. Video 2: Corticobasal degeneration with apraxia. Tremor, akinesia, myoclonic jerks and left hand dystonia. Symbolic motor sequences are not properly performed: cross sign is performed from right to left shoulder, thumbing one’s nose is replaced by a kiss, showing that someone is a fool is done uncompletely and cross sign is not possible with left hand. Video 3: Multiple system atrophy (MSA-P). At an early stage, DOPA-resistant akineto-rigid syndrome is associated with inability to walk without aid and postural instability. Video 4: Progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome). Vertical voluntary saccades are slow and with limitation of the amplitude of the saccades. Horizontal voluntary saccades are reduced and several ocular movements (several small saccades) are needed to move the eyes from side to side. Oculocephalic reflexes (VOR) are normal, demonstrating the supranuclear location of the dysfunction. Postural instability is observed. Video 5: Abnormal eye movements in progressive supranuclear palsy. Vertical and horizontal voluntary saccades are reduced. Several saccades are needed to reach the target. Perseverations are observed, the patient looks at a previous target when asked to look to another direction. Frontalis muscle contractions are associated with upward saccades. Oculocephalic reflexes are normal (but difficult to perform because of distractibility and cervical stiffness), demonstrating the supranuclear location of the dysfunction. Video 6: Frontal behavior in Progressive supranuclear palsy. As described by Lhermitte, frontal behavioral signs include grasping reflex (even when discouraged), utilization behavior and collection of the examinator’s personal stuff without order, imitation behavior with imitation of all the gestural activities of the examinator, including nonsense as eating a metallic object. Video 7: Postural instability in Progressive supranuclear palsy. Spontaneous postural instability. A gentle pulling test would make the patient fall, without any attempt or ability to recover his balance (loss of postural reflexes). REFERENCES 1. Litvan I, Bhatia KP, Burn DJ, et al. SIC task force appraisal of clinical diagnostic criteria for parkinsonian disorders. Mov Disord 2003;18:467–486. 2. Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol 1999;56:33–39. 3. Rao G, Fisch L, Srinivasan S, et al. Does this patient have Parkinson disease? JAMA 2003;289:347–353. 4. Litvan I, Campbell G, Mangone CA, et al. Which clinical features differentiate progressive supranuclear palsy (Steele– Richardson–Olszewski syndrome) from related disorders? A clinicopathological study. Brain 1997;120:65–74. 5. Nutt JG, Marsden CD, Thompson PD. H walking and higher-level gait disorders particularly in the elderly. Neurology 1993;43:268–279. 6. Lhermitte F. Utilization behaviour and its relation to lesions of the frontal lobe. Brain 1983;106:237–255. 7. Lhermitte F, Pillon B, Serdaru M. Human autonomy and the frontal lobes. Part I: imitation and utilization behavior: a neuropsychological study of 75 patients. Ann Neurol 1986;19:326–334. 8. Leigh RJ, Riley DE. Eye movements in parkinsonism. It’s saccadic speed that counts. Neurology 2000; 54:1018–1019. 9. Rivaud-Pechoux S, Vidailhet M, Gallouedec G, Litvan I, Gaymard B, Pierrot-deseilligny C. Longitudinal oculomotor study in corticobasal degeneration and progressive supranuclear palsy. Neurology 2000;54:1029–1032. 162 Vidailhet, Bourdain, and Trocello 10. Birdi S, Rajput AH, Fenton M, et al. Progressive supranuclear palsy diagnosis and confounding features: report on 16 autopsied cases. Mov Disord 2002;17:1255–1264. 11. Gilman S, Low PA, Quinn N. Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci 1999;163:94–98. 12. Chaudhuri KR. Autonomic dysfunction in movement disorders. Curr Opin Neurol. 2001;14:505–511. 13. Wenning GK, Scherfler C, Granata R, et al. Time course of symptomatic orthostatic hypotension and urinary incontinence in patients with postmortem confirmed parkinsonian syndromes: a clinicopathological study. J Neurol Neurosurg Psychiatry 1999;67:620–623. 14. Riley DE, Chelimsky TC. Autonomic nervous system testing may not distinguish multiple system atrophy from Parkinson’s disease J Neurol Neurosurg Psychiatry 2003;74:56–60. 15. Fenelon G, Mahieux F, Huon R, Ziegler M. Hallucinations in Parkinson’s disease: prevalence, phenomenology and risk factors. Brain 2000;123:733–745. 16. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47:1113–1124. 17. Boesch SM, Wenning GK, Ransmayr G, Poewe W. Dystonia in multiple system atrophy. J Neurol Neurosurg Psychiatry 2002;72:300–303. 18. Barclay CL, Lang AE. Dystonia in progressive supranuclear palsy. J Neurol Neurosurg Psychiatry 1997;62:352–356. 19. Litvan I, Grimes DA, Lang AE et al. Clinical features differentiating patients with postmortem confirmed progressive supranuclear palsy and corticobasal degeneration. J Neurol 1999;246(Suppl 2):II1–II5. 20. Monza D, Ciano C, Scaioli V, et al. Neurophysiological features in relation to clinical signs in clinically diagnosed corticobasal degeneration. Neurol Sci 2003;24:16–23.