Morbidity & Mortality Grand Rounds Department of Medicine September 29, 2015

Morbidity & Mortality
Grand Rounds
Department of Medicine
September 29, 2015
2
Upcoming M&M Dates
December 1, 2015
February 2, 2016
March 15, 2016
April 26 th , 2016
May 24 th , 2016
If you have a case for our M&M conference please email: Omar Darwish, DO at odarwish@uci.edu
Goals & Objectives
Goals
• Opportunity for learning and reflection
• Improve quality and safety for our patients
• Learn from medical errors, complications and unanticipated outcomes (without blame)
Objectives
• To improve our medical knowledge
• To recognize clinical reasoning errors
• Improve communication and documentation among the hospitalist, medicine specialist and other departments
3 Department of Medicine| September 29, 2015
Resident’s HPI- Day of Admission (1300)
29 year old male presents with a 1 week history of RUQ pain after eating. He states that the pain lasts for about 10 minutes, does not radiate, and is a 6/10 in severity. He has had several episodes of this pain over the past week, and it is also associated with some dizziness and sweating.
A few days later, he also noticed darkening of his urine, yellow
coloring in his eyes, and for the past 3 days, he has had nonbloody, non-bilious vomiting in the mornings. This prompted him to come to the emergency room. He denies any changes in bowel movements, fevers, chills, chest pain or shortness of breath.
In the ED, evaluation was significant for transaminitis (ALT 480s,
AST 200s), elevated Alkaline Phosphatase, and Total bilirubin of
~7. Abdominal ultrasound showed cholelithiasis without CBD dilation or stone.
4 Department of Medicine | September 29, 2015
Physical Exam
Vital Signs: Tc: 36.6 HR: 82 (76 - 89) BP: 145/82 (144 - 164 / 82 -
99) RR: 18 (16 - 18) SpO2: 98% Wt: 92.5kg, 160.0cm, BMI: 36.1
General: Young male, sitting up in bed, in no acute distress
HEENT: PERRL, EOMI, clear oropharynx
Neck: supple
Lungs: CTA bilaterally, no wheezing, or crackles appreciated
Heart: regular, S1 S2, no murmurs appreciated
Abdomen: Mild tenderness in RUQ, positive murphy's sign, no guarding or rebound tenderness, non-distended, normoactive bowel sounds
Extremities: lower extremities without edema
Neurological: CNII-XII grossly intact, no sensory or motor deficits
5
Skin: no suspicious lesions on gross examination
Department of Medicine September 29, 2015
6
Admission labs
138
3.9
104 8
26 0.8
100
9.1
8
15
44.5
213
PT: 10.6 / INR: 1.00
Prot: 7.7 / Alb: 4.3 / Bili: 7.1 / AST: 217 / ALT: 485 / AlkPhos: 255
Abdominal ultrasound
Admission Ultrasound
Common Bile Duct: 0.397 cm
7
Gallstones within the gallbladder
Assessment/Plan
29M without active past medical history:
#RUQ Pain - stable
- Elevated ALT/AST, alk phos, total bilirubin, Indicative of choledocholithiasis with obstructive hepatitis, No current infection
- GI Consulted, planning ERCP
- NPO
- Fluid hydration
- Pain control
- Eventual surgical evaluation
Day of Admission: Staffed in the
Emergency Room with Hospitalist
Attending Attestation: “Plan for
ERCP, no signs of infection.”
#VTE risk: Moderate
- SubQ heparin TID
8
Questions for Gastroenterologist- Dr. John Lee
• How sensitive is an EUS in ruling out the presence of stones within the biliary system? What about MRCP? Which is more sensitive?
• In places where EUS is done, is it common practice to perform
EUS first to make sure the presence of a stone exist within the biliary ducts before proceeding to ERCP?
• Can you please review the EUS images?
9 Department of Medicine| September 29, 2015
Endoscopic Ultrasound
10 Department Name | Month X, 201X
Endoscopic Ultrasound
11 Department of Medicine| September 29, 2015
Endoscopic Ultrasound
12 Department Name | Month X, 201X
Endoscopic Ultrasound
IMPRESSION: Given large number of small stones in the gallbladder, but nondilated duct, it is possible patient has passed a stone. LFTs should be trended and if no improvement, then a parenchymal liver disease process needs to be considered with possible Liver biopsy after serologic work up.
RECOMMENDATIONS:
1. Return to floor
2. Trend LFTs
3. Serologies for chronic liver disease
4. Can consider EUS guided liver biopsy if jaundice does not resolve quickly
5. Recommend surveillance of pancreatic cyst. Consider repeat EUS or MRI in
1-2 years.
13 Department of Medicine | September 29, 2015
Hepatology Fellow Consult Note
Assessment Recommendation
#Hyperbilirubinemia send the following autoimmune serologies: ANA, AMA, SMA, LKM Ab
# Elevated transaminases
-send monospot and EBV PCR
# Elevated Alk P
# Mild intrahepatic ductal dilation on initial
US:
Differential diagnosis includes choledocholithiasis that has resolved (passed stone), viral hepatitis including EBV, autoimmune hepatitis, drug induced liver injury, and structural liver disease (Budd chiari). We favor a passed stone given evidence of cholelithiasis and a clinical pain syndrome that is very typical of biliary colic. Initial US also shows mild intrahepatic dilation, which may be sequela of a recently passed stone. Viral serologies for an acute hepatitis infection have been negative, although we should consider EBV given he works with small children as a bus driver. Autoimmune hepatitis is always possible, although does not usually present acutely in this manner, but is deserving of serologic rule out.- There is no laboratory or clinical evidence of portal hypertension or cirrhosis
-would complete viral workup with the following: HBV cAb total, HAV IgG trend LFTs and pain syndrome (ok to eat as no further GI procedures are planned at this point) if LFTs do not trend down, will likely require MRCP and possible liver biopsy pending results of the above workup
# NAFLD: as seen on US
# Hepatomegaly
-pt should be counseled on trying to lose a bit of weight given his underlying steatosis as seen on US
14 Department of Medicine| September 29, 2015
Hepatology Attending Attestation
The patient presented with acute RUQ pain associated with jaundice, and US report of bile duct dilatation and cholelithiasis.
However, EUS yesterday reported multiple gallstones and the biliary system was non-dilated and had no endosonographic abnormalities. The CBD was 6 mm in diameter. His abdominal pain has resolved, but t bili has not improved in the past 24 hours. If this is due to passed stone, would expect improvement of hyperbilirubinemia.
Suggest continuing monitoring LFTs for at least one more day. He also has underlying NAFLD, likely due to obesity. We have reviewed our above A/Rs with the patient and his family.
15 Department Name | Month X, 201X
Questions for Hepatologist- Dr. Hu
• This patient has pain with eating that is supportive of a biliary colic presentation. Are there other diseases that can give similar presentations such as autoimmune hepatitis, Wilson’s disease and viral hepatitis?
• Is it recommended to do an autoimmune workup at this time?
• Does a serum ANA have a high sensitivity for autoimmune hepatitis?
16 Department Name | Month X, 201X
17
Intern’s Note: Hospital Day #2
Seen sitting up comfortably in bed. Noted some typical RUQ pain after dinner last night, lasted for
<1hr, resolved when fluids restarted. No pain since, no chest pain, shortness of breath, nausea, vomiting.
Exam: unchanged
Prot: 7.1 (7.1)/ Alb: 4.2 / Bili: 7.0 / Dir: 4.3 / AST: 265 (217) / ALT: 586 (485) / AlkPhos: 222 (255)
Assessment/Plan:
#Transaminitis and cholestasis
- No stone seen on EUS, ERCP not pursued by GI
- Markers indicative of ongoing or resolving cholestasis vs hepatitis
- Fluid hydration
- Pain control
- Will continue to monitor LFTs for improvement
Attending’s Note: “we will see where the LFT’s go tomorrow. Given the patient’s gallstones, we suspect patient passed a stone. Will hold off sending out test for liver disease.”
Hepatology Fellow Note- Hospital Day #3
Recommendation f/u AMA, SMA
Primary team has chosen not to send monospot, EBV studies, ANA, or LKM ab and instead will wait for LFT studies would complete viral workup with the following: HBV cAb total, HAV IgG trend LFTs and pain syndrome (ok to eat as no further GI procedures are planned at this point) if LFTs do not trend down, will likely require MRCP and possible liver biopsy pending results of the above workup pt should be counseled on trying to lose a bit of weight given his underlying steatosis as seen on US if LFTs trend down, we can reasonably assume that this episode was related to a biliary stone. In this case, he needs to be evaluated by a surgical service for cholecystectomy
Please ensure that pt has followup with PCP after he is discharged (CM and SW may need to assist with this). Does not require hepatology follow up unless autoimmune labs are positive or LFT pattern is inconsistent with passed stone. Recommend stay overnight for one more round of labs tomorrow morning to ensure LFTs continue to improve.
18 Department of Medicine | September 29, 2015
Primary Team Progress Note- Hospital Day #3
S: tolerating liquid only
Exam: non-tender abdomen
Labs: ALT 586 (657), AST 245 (265), T. Bilirubin 5.8 (7.1), D. bili 4.3, alk phos 211 (222), GGT 503. Hepatitis Panel negative, and monospot negative
“MRCP and CT abdomen with contrast to see if patient has abscess/hematoma/blood clot within the liver”
Attending’s addendum:
“Enzymes are not coming down the way we would like. Suspect initially patient passed a stone, but maybe there is another process. Will order some imaging of liver/biliary system.”
19 Department of Medicine| September 29, 2015
MRCP
20
Department of Medicine | September 29, 2015
MRCP
21 Department Name | Month X, 201X
MRCP Results
The gallbladder is distended with numerous small stones to the level of the origin of the cystic duct.
Cholelithiasis without evidence of acute cholecystitis or
choledocholithiasis. Variant anatomy with an aberrant right posterior bile duct draining into the cystic duct before it joins the common hepatic duct.
A 6 mm nondependent hypointense focus in the anterior fundal wall.
Liver is enlarged at 18 cm. No intrahepatic duct dilation. CBD 6 mm.
22 Department of Medicine| September 29, 2015
CT Abdomen w/ IV Contrast
• The liver is borderline enlarged measuring 18 cm in the craniocaudal dimension with mild fatty infiltration at the falciform ligament. No focal lesions. Normal hepatic vascular enhancement. No evidence of intra and extra hepatic biliary ductal dilatation and no definite stone or mass.
•
Gallbladder and Biliary Tree: The gallbladder is distended containing stones, most of which are radiolucent and better evaluated on MRI from the same day. No CT evidence of acute cholecystitis.
23 Department of Medicine| September 29, 2015
Primary Team Progress Note- Hospital Day #4
S: RUQ pain after 3 hours of eating
Exam: unchanged, no TTP abdomen
Labs: T.bili 7.9 (5.8), AST 207 (245), ALT 637 (657), alk phos 234
(211)
A/P: #Transaminitis with cholestasis - ongoing
Pain syndrome typical of biliary colic
Spoke with GI fellow today, recommended involving hepatobiliary surgery team for further evaluation
Continue pain control PRN
24 Department Name | Month X, 201X
Hepatology Progress Note: Day #4
A: Negative studies thus far include viral a B and C serologies anti smooth muscle antibody and anti mitochondrial antibody. Endoscopic ultrasound did not show any sort of obstructing biliary stone. The etiology of the patient's liver disease is unclear. The differential idiopathic, atypical viral infection, PSC, choledocholithiasis.
Recommendations:
-would recommend EBV studies, ANA, or
LKM ab
- would complete viral workup with the following: HBV cAb total,
- trend LFTs and pain syndrome (ok to eat as no further GI procedures are planned at this point)
- we recommend surgical evaluation with hepatobiliary service for cholecystectomy
The patient's LFTs are stable but his T bili has increased and he continues to have right upper quadrant abdominal pain.
- if LFTs do not trend down will consider
MRCP tomorrow
Mixed cholestatic/hepatocelluar LFTs
- if LFTs continue to trend upward then may consider IR guided liver biopsy
25 Department Name | Month X, 201X
Hospital Day #5 Labs
Labs: T.bili 9.3 (7.9), AST 209 (207), ALT 596 (637), alk phos 259
(234).
ANA: negative
Ferritin 390
Leptospira Ab < 1:50
EBV PCR negative
26 Department of Medicine | September 29, 2015
Hepatobiliary Surgery Consult Note (Day #6)
A/R: No acute surgical intervention at this time. Variant anatomy and gallstone likely not the etiology of elevated LFTs.
Continue workup to include autoimmune and viral panels
Trend labs including LFTs
Plan for IR biopsy today
Care per Primary
Attending Attestation: While imaging studies have demonstrated cholelithiasis, there is no intra or extrahepatic biliary ductal dilatation. It appears to be extremely unlikely that the patient's hyperbilirubinemia is secondary to gallstones or gallbladder inflammation. The patient's symptoms and laboratory tests appeared to be more consistent with acute hepatitis.
27 Department of Medicine | September 29, 2015
Hospital Day #6
Laboratory studies:
T.bili 9.5 (9.3), AST 196 (209), ALT 596 (580), Alk phos 269 (259)
Liver biopsy is performed by IR. No complications
Hepatology recommends ordering ceruloplasmin.
28 Department of Medicine| September 29, 2015
34
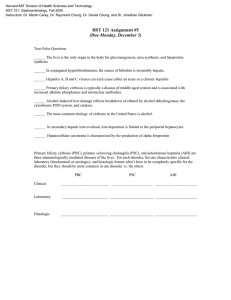
Lab Trends and Events
Day 5:
Liver Bx
35
T. Bili Trends Up
Hepatology Attending Note
“I have reviewed his liver biopsy slides with the pathology attending: mild background fatty liver, some cholestasis and portal inflammation, and in 2-3 portal areas with occasional bile duct damage, and more portal areas with reactive changes. Overall, can not differentiate intrahepatic vs extrahepatic cause. I have also reviewed his MRCP with Radiology and HBS Attendings.
It seems to have a very short segment of distal CBD stricture, thus indicated for MRCP. Due to history of recent uncooked seafood
(not raw oyster), reasonable to check anti-HEV antibody. He also have some herbal tea from herbal life, but unlikely the source of his liver injury.”
36 Department of Medicine| September 29, 2015
Hospital Day #9- EUS/ERCP Performed
EUS: The CBD was dilated 10 mm. Four stones were found in the distal common bile duct, the largest stone measuring 4 mm.
Cholangiogram showed multiple filling defects in the bile duct.
With guidewire in the bile duct, a biliary sphincterotomy was performed using the sphincterotome. Using a stone extraction balloon the bile duct was swept three times. Four stones were removed from the bile duct successfully. Multiple smaller stones and debris was also removed.
Under endoscopic and fluoroscopic guidance a 10 Fr x 7 cm
CookCotton-Leung Sof-Flex stent was placed in the bile duct.
37 Department of Medicine| September 29, 2015
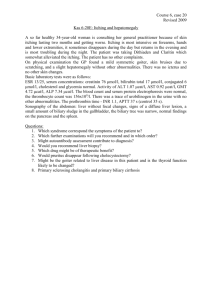
38
Post ERCP Labs
Diagnosis: Choledocholithiasis/Gallstone Hepatitis
GI Attending Note: “I discussed this case with the hepatobiliary service about possible inpatient surgical removal of his GB. He stated that the patient has complex anatomy and the team would like to do his surgery as an outpatient and should follow up with them. “
Questions for Dr. Victor Joe, General Surgery, Director of the
Burn Center:
This patient presented with biliary colic, elevated liver enzymes but no signs of infection. When is it best to perform a cholecystectomy?
Does the degree of enzyme elevation play a role in you decision on when to operate?
•
Does the complications/manifestations of cholelithiasis matter
(gallstone pancreatitis, cholangitis) in determining this?
What makes this patient have complicated anatomy and how does this change your decision for inpatient versus outpatient surgery?
39
Post Discharge Follow Up
LFT’s
Alk phos 119
Total Bili 1.4
AST 26
ALT 55
• Seen for follow up by Family Medicine (Santa Ana Clinic)
• Unable to schedule GI follow up for stent removal “due to insurance issues”
• Has not been scheduled to see hepatobiliary surgery (instructed to call their clinic)
40 Department of Medicine| September 29, 2015
Summary
• Patient was hospitalized for total of 11 days
• Total of 2 CT Scans Abdomen
• Abdominal Ultrasound, MRCP performed
• Underwent two EUS, one ERCP
• Liver Biopsy Performed
• Multiple serology and studies sent for evaluation of transaminitis
• Still awaiting cholecystectomy
Total Cost: ?
41 Department of Medicine| September 29, 2015
Key Learning Points
• Don’t forget about rare manifestations of common conditions
• Clinical Reasoning Error: Overreliance on imaging resulted in an alternative pathway, i.e. liver disease.
•
Anchoring & Availability Heuristic
•
Framing Effects
•
Blind Obedience
• If clinical suspicion is high and initial findings don’t corroborate, re-review studies earlier rather than later
• Communication between different services is key
•
If there is disagreement in diagnosis/management, a conversation is better than documenting the differences.
42
High-Value Care= providing the best care possible while also reducing unnecessary costs to the health care system