Income and Benefits Policy Center

www.urban.org
aPrIl 2012
Income and Benefits
Policy Center
I N s I d e T h I s I s s u e
• Over the past decade, WIC has been one of the fastest growing federal nutrition programs.
•half of infants and a quarter of young children, pregnant women, and postpartum women receive WIC.
•WIC provided $6.7 billion of nutritional support in 2009.
•sixty-one percent of all persons eligible for WIC participated in the program in 2009.
WIC Participants and Their Growing
Need for Coverage
Michael Martinez-Schiferl
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) provides low-income pregnant women, postpartum mothers, infants, and children up to age 5 with select foods, nutrition education, and health care and government service referrals. WIC helps ensure that those most at risk of not receiving adequate nutrition get assistance at a critical time in their development. Early intervention aims to improve the health of participants and prevent later health problems.
W IC serves many in need. More than half of all infants and more than a quarter of all children through age 4 , pregnant women, and postpartum women participate. Nearly two-thirds of all WIC participants live below the federal poverty level (FPL) even though individuals with incomes less than 185 percent of FPL are eligible to participate.
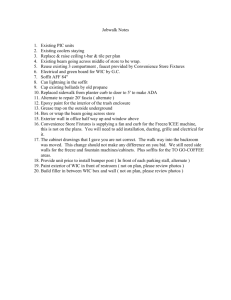
WIC is a central component of the federal food nutrition safety net. It is the third-largest federal food nutrition program, accounting for 7 .
0 percent of the spending on food and nutrition assistance during FY 2010 (figure 1 ).
More than $ 6 .
7 billion was spent through
WIC ($ 4 .
6 billion in food costs and $ 1 .
9 billion in administration expenses 1 ) on food and other services for a monthly average of 9 .
2 million participants.
This brief summarizes key features of the
WIC program, including eligibility rules, participation, benefits, and administration. It presents the 2009 estimates of WIC eligibility and coverage for the nation and the states.
2 Also summarized are recent improvements in WIC administrative practices and nutrition outcomes.
What Is WIC?
WIC was established in 1972 to assist lowincome women, infants, and children at nutritional risk. This is accomplished through supplemental foods, nutrition education, and referrals to health care and other government services (Food and Nutrition
Service 2011 c). WIC was last authorized in
December 2010 through the Healthy,
Hunger-Free Kids Act.
3
Studies suggest that WIC dollars translate into cost savings on health spending for the government, and new changes in
WIC
food packages should further improve health outcomes.
WIC Participants and Their Growing Need for Coverage
Figure 1. u.s. expenditures for Food and Nutrition assistance
Programs, FY 2010
Total food and nutrition program expenditures in FY2010: $95.3 billion
Source: U.S. Department of Agriculture, Food and Nutrition Service, Program Information Report (Keydata): fy2010 – fy2011 .
Note: Program expenditures include administrative costs.
WIC is a discretionary spending program and therefore participation may be limited by annual funding established by Congress. In recent years nearly all eligible applicants have received benefits, reflecting Congress’s desire to fully fund the program. A seven-point priority system ensures that those with the greatest nutritional risk receive benefits in the event of a funding shortage. Highest priority is given to infants, pregnant women, and breastfeeding women with nutrition-related medical conditions.
The U.S. Department of Agriculture, Food and Nutrition Service, administers WIC by providing states with grants for supplemental foods and services. States use grants to supply vouchers that program participants redeem at authorized food stores for certain nutritious foods.
4
SNAP
71.7%
Commodity
Food Distribution
2.1%
All other programs
2.1%
More than 46 , 000 merchants nation-
Child and Adult Care
Food Program
2.8%
School Breakfast
3.0%
WIC
7.0%
School
Lunch
11.3% wide accept WIC vouchers (Food and
Nutrition Service 2011 c). WIC voucher amounts are based on WIC supplemental food packages. With the exception of vouchers for fresh fruit and vegetables, WIC vouchers are typically for a specified quantity of a particular good (e.g., one dozen eggs), and therefore the value of the vouchers varies with local food costs.
WIC food packages supplement participants with foods high in nutrients often lacking in their diets. In 2009 , FNS revised WIC food packages to narrow the possibility of both inadequate and excessive nutrient intakes and to be more flexible with dietary preferences. The new WIC packages include more fresh fruits and vegetables, more whole grain foods, and less formula during the first six months of an infant’s life. The change in the infant formula allotments aimed to encourage partially breastfeeding mothers to increase breast milk use.
WIC food packages are tailored for infants, children, and women (table 1 ), and benefit packages are the same for participants throughout the nation. Partially and fully formula-fed infants are provided monthly allotments of iron-fortified formula. For all infants starting at 6 months, baby food fruits and vegetables and iron-fortified infant cereal are introduced; fully breastfed infants also receive an allotment of baby food meat.
Children receive vitamin-C-rich juice, fruits and vegetables, milk, iron-fortified whole grain cereal, whole wheat bread, eggs, and legumes. Pregnant, postpartum, and partially breastfeeding women receive many of the same foods as children but different quantities. Fully breastfeeding women receive an additional allotment that includes eggs, cheese, canned fish, and peanut butter (Food and Nutrition Service 2011 d).
WIC provides participants and caretakers with nutrition education that emphasizes the relationship between nutrition, physical activity, and health. Information on nutritional needs is targeted for infants, children, and pregnant and postpartum women. Pregnant and postpartum women are made aware of the benefits of breastfeeding and the dangers of substance abuse.
Participation in nutrition education classes is not mandatory in order to receive benefits, but state agencies are required to offer classes.
Local WIC agencies also assist WIC participants through referrals for other health care services such as immunizations or
Medicaid, as well as assistance from other safety net programs like the Supplemental
Nutrition Assistance Program (SNAP).
Who Is eligible and Who Participates?
WIC eligibility is based on categorical, residential, income, and nutritional risk requirements
(table 2 ). Only pregnant and postpartum women, infants, and children through age 4 are categorically eligible, and their family
2.
WIC Participants and Their Growing Need for Coverage
Table 1. summary of WIC Food Package Monthly allotments
Foods
Iron-fortified infant formula
Juice
Milk
Iron-fortified whole grain cereal eggs
Fruits and vegetables
Whole wheat bread legumes
Other
Infants
364 –884 fl oz a,b
(none for those fully breastfed)
1 dozen
128–256 oz a starting $6 in cash at 6 months value vouchers
Source: Food and Nutrition Service ( 2011 d).
a. Exact quantity dependent on breastfeeding status.
b. Reduced quantities for younger and partially breastfed infants.
income must be below eral poverty income guidelines ($ family of four in the continental United States from July 2011 to June
24 oz starting at 6 months
Fully breastfed infants:
77.5 oz baby food meat starting at 6 months
185
2012 percent of the fed-
41 , 348 for a
). However, if a categorically eligible person participates in SNAP
(formerly Food Stamps), Medicaid, Temporary
Assistance for Needy Families (TANF), or certain other state-administered programs, the income requirement is waived and she becomes adjunctively eligible. Eligibility also
Children
(age 1 – 4)
128 fl oz
16 qt
36 oz
2 lb
1 lb dry (or 64 oz canned) or 18 oz peanut butter
Women
96–144 fl oz a
16–24 qt a
36 oz
1 dozen
$10 in cash value vouchers
1 lb (none for postpartum women)
1 lb dry (or 64 oz canned) or 18 oz peanut butter
Postpartum fully breastfeeding women: additional 1 dozen eggs, 1 lb cheese, 30 oz canned fish, and 18 oz peanut butter depends on a person experiencing “nutritional risk,” either through poor diet or medical conditions. In practice, though, nearly all persons income eligible are considered to be at nutritional risk due to the relationship between income resources and an adequate diet.
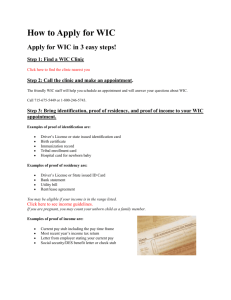
In CY 2009 , an estimated 2 .
7 million infants, 9 .
5 million children, and 2.9
million women were WIC eligible (figure 2 ). Of those,
2 .
2 million infants, 4 .
8 million children, and
2 .
2 million women participated, for coverage rates of 82.9
percent, 50.6
percent, and 74.3
percent, respectively. Nationally, 51 .
2 percent of all infants, 27 .
4 percent of children age 1–4 , and 28 .
9 percent of all pregnant and postpartum women received WIC benefits in 2009 .
Growth in WIC eligibility from 2000 to
2009 is the result of several factors, including population growth and changes in income and participation in other means-tested programs (figure 3 ). The number of infants and children in the United States grew from 19 .
7 million in 2000 to 21 .
6 million in 2009 (an increase of 9 .
4 percent). The number of WIC income-eligible infants and children grew from 8 .
1 million in 2000 to 9 .
7 million in
2009 (an increase of 19 .
8 percent). The number of WIC adjunctively eligible infants and children grew from 1 .
4 million in 2000 to 2 .
2 million in 2009 (an increase of 61 .
1 percent).
The total number of eligible infants and children both income and adjunctively eligible grew by 25 .
8 percent from 2000 to 2009 .
Changes in eligibility since the recession began (comparing 2008 to 2009 ) show that a
7 .
7 percent growth in total number eligible was almost completely due to changes in income and an increase in the number of WIC income eligible.
WIC 2010 participant data indicate that nearly two-thirds of WIC enrollees lived below the federal poverty level; 31 .
7 percent in deep poverty (below 50 percent of the poverty level) and 32 .
1 percent between 50 and 100 percent of the poverty level (Conor et al. 2011 ).
Many enrollees also participated in other means-tested programs. In 2010 , over twothirds of WIC participants ( 69 .
2 percent) reported receiving benefits from Medicaid,
SNAP, or TANF, up from only half ( 50 .
2 percent) in 2000 (Conor et al. 2011 ).
5 This increase follows general trends of increasing participation in these other safety net programs.
Over time, the race/ethnicity composition of WIC enrollees has steadily changed, with Hispanics now representing the largest
3.
WIC Participants and Their Growing Need for Coverage
Table 2. summary of WIC eligibility requirements
requirement
Categorical residential
Income
Nutritional risk description
Families with infants and children through age 4, pregnant women (up to six weeks after birth or end of pregnancy), postpartum breastfeeding women (up to infant’s first birthday), or postpartum women not breastfeeding (up to six months after child’s birth).
Must apply in own state of residence. No minimum residency requirements. Citizenship or legal residency is not a federal requirement for eligibility; however, states may choose to impose such requirements.
Income cannot exceed 185 percent of the federal poverty income guidelines. Participants in sNaP, Medicaid, TaNF, and certain other stateadministered programs are not subject to this income requirement.
Must be determined to be at “nutritional risk” based on poor diet or medical conditions. Nearly all income-eligible applicants meet the nutritional risk requirement.
Figure 2. WIC eligibility and Participation by Group, CY 2009
20,000
15,000
10,000
5,000
4,330
2,674
2,218
0
Infants
Source: Betson et al. ( 2011 ).
17,509
9,469
4,789
Children
(Age 1–4)
Total
Eligible
Participants
7,548
2,932
2,179
Pregnant and postpartum women portion of those enrolled. The proportion of
Hispanic WIC recipients grew from 35 .
3 percent in 2000 to 41 .
9 percent in 2010 while the proportions of black and white WIC recipients have declined from 37 .
4 to 31 .
8 percent for whites and 21 .
9 to 20 .
1 percent for blacks (Conor et al. 2011 ). This increase in
WIC enrollment among Hispanics, relative to whites and blacks, corresponds with a large growth in the Hispanic population from 33 .
7 million in 2000 to 49 .
9 million in 2010 (a
47 .
9 percent increase) and a large increase in the number of Hispanic poor from 7 .
1 million in 2000 to 13 .
2 million in 2010 (an 85 .
1 percent increase) (Dalaker 2001 ; DeNavas-
Walt, Proctor, and Smith 2011 ).
Growth in WIC enrollment numbers from
2000 through 2010 has primarily come from an increase in the number children through age 4 , which increased by 36 .
2 percent ( 3 .
5 million in 2000 to 4 .
8 million in 2010 ). The number of women receiving WIC increased by 20 .
5 percent (from 1 .
8 million in 2000 to 2 .
1 million in 2010 ); enrolled infants increased by 13 .
2 percent ( 1 .
9 million to 2 .
2 million).
Coverage rates, the number enrolled divided by the number eligible, have increased slightly from 2000 to 2009 : 57 .
8 percent in
2000 to 60 .
9 percent in 2009 for all participants (figure 4 ).
6 Coverage rates for infants and women are higher than for all participants. For infants, coverage rates increased from 78 .
6 percent in 2000 to 82 .
9 percent in 2009 . For women, coverage rates increased from 66 .
1 percent in 2000 to 74 .
3 percent in 2009 . Coverage rates for children are lower than for all participants but still increased from 48 .
0 percent in
2000 to 50 .
6 percent in 2009 . The differences between these national-level coverage rates all fall within 90 percent confidence intervals.
7
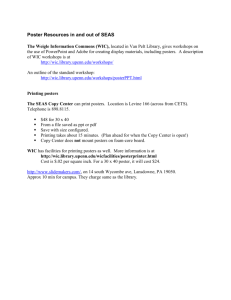
WIC coverage varies considerably by state
(figure 5 ). In 2009 , state coverage for all WIC participants ranged from 45 .
9 percent to 78 .
7 percent, compared to 60 .
9 percent for the nation. The five states with the lowest WIC coverage rates are Montana ( 45 .
9 percent),
4.
WIC Participants and Their Growing Need for Coverage
Utah ( 47 .
3 ), Colorado ( 48 .
5 ), Idaho ( 50 .
7 ), and Illinois ( 50 .
8 ). The five states with the highest WIC coverage rates are Puerto Rico
( 78 .
7 percent), Vermont ( 76 .
3 ), the District of
Columbia ( 76 .
2 ), California ( 73 .
7 ), and
Minnesota ( 73 .
5 ). Figure 5 also shows the 90 percent confidence intervals for each state’s coverage rate.
8 These confidence intervals depend on sampling variability of the surveys used to produce the estimates; 9 generally, states with larger populations tend to have smaller confidence intervals.
What do We Know about WIC Outcomes?
Research documents the positive benefits of
WIC. A recent literature review concluded that WIC participation has a positive impact on birth weight (Coleman et al. 2012 ). The study also found that WIC participation is associated with improved diets among children, including reduced intake of fats and added sugars and increased intake of fruits and vegetables. Research also suggests that
WIC participants are more likely to use both preventive and curative health care services.
Finally, Lee, Mackey-Bilaver, and Chin
( 2006 ) found that participation in WIC is associated with a reduced risk of child abuse and neglect. While more research is needed to confirm whether the effect is indeed causal, this finding suggests that nutrition assistance programs may help children in many ways.
Two studies on the effect of WIC on birth outcomes quantified the savings that WIC services provide in health care costs for newborns.
Devaney, Bilheimer, and Schore ( 1990 ) found that for each dollar spent on WIC prenatal services, $ 1 .
77 to $ 3 .
13 was saved in Medicaid costs for newborns and mothers within the first 60 days after birth. A report from the U.S. General
Accounting Office ( 1992 ) concluded that each dollar of WIC spending resulted in $ 3 .
50 in savings (in present value terms) in health care costs and other government program expenditures over 18 years. However, Besharov and Germanis
Figure 3. Trends for WIC eligibility for Infants and Children
(age 0–4), 2000 to 2009
25,000
20,000
15,000
10,000
Population of infants and children (age 0–4)
Income eligible
Adjunctively eligible
Income and adjunctively eligible
5,000
0
2000 2001
Source: Betson et al. ( 2011 ).
2002 2003 2004 2005 2006 2007 2008 2009
Figure 4. Coverage rates by Participant Group, 2000–2009 (%)
100
90
80
70
60
50
40
30
20
10
0
2000 2001
Source: Betson et al. ( 2011 ).
2002 2003 2004 2005 2006
Infants
Children
Women
Total
2007 2008 2009
5.
WIC Participants and Their Growing Need for Coverage
Figure 5. WIC eligibility and Participation by state, CY 2009
HOW MANY WERE ELIGIBLE FOR WIC IN CY 2009? WHAT PERCENTAGE PARTICIPATED?
Eligible people
(000)
Coverage Rates and Confidence Intervals
Coverage Rate = 100 X Number of Persons Participating / Number of Persons Eligible
(Estimated coverage rates are shown between the bounds of their confidence intervals.)
325
85
399
289
26
132
172
198
496
316
129
43
52
613
92
226
156
45
295
284
462
238
439
571
214
31
242
259
104
888
211
40
126
128
504
24
44
197
802
221
83
40
1,616
251
23
23
1,958
192
210
56
300
175
15,075
Arkansas
Mississippi
North Carolina
Indiana
Nevada
South Dakota
Tennessee
Nebraska
Arizona
Missouri
Wyoming
New Mexico
Wisconsin
New Hampshire
Alabama
Louisiana
Connecticut
Florida
New Jersey
Virginia
Pennsylvania
South Carolina
Michigan
Georgia
Maine
Illinois
Idaho
Colorado
Utah
Montana
Puerto Rico
Vermont
District of Columbia
California
Minnesota
Maryland
Hawaii
Washington
Oregon
Massachusetts
New York
Kentucky
West Virginia
Rhode Island
Texas
Oklahoma
Delaware
Iowa
Kansas
Ohio
North Dakota
Alaska
United States
36.9
38.6
55.2
54.9
71.8
48.3
50.0
54.3
53.4
54.6
60.0
58.4
58.7
58.5
61.3
56.6
63.8
66.2
66.1
65.3
65.1
65.1
64.7
64.5
60.1
64.0
63.1
62.8
65.5
61.2
62.5
60.7
70.8
70.5
68.2
68.4
68.0
44.0
43.0
45.2
45.8
48.2
47.5
53.4
51.6
51.8
54.5
53.4
53.5
50.3
53.1
54.8
52.2
49.9
50.1
50.3
53.0
52.6
52.8
56.6
55.7
55.5
55.4
60.7
60.5
60.3
60.2
64.4
58.0
57.8
57.7
56.8
56.8
56.7
56.5
56.2
60.1
59.4
58.7
58.6
60.6
60.3
59.7
61.7
65.7
60.8
62.4
61.5
63.9
63.6
65.6
61.5
60.9
67.9
54.6
53.9
53.8
59.0
58.9
60.3
64.6
49.5
48.9
53.7
53.5
52.7
56.4
57.9
61.2
73.7
73.5
70.5
71.8
71.4
70.5
73.5
72.1
74.1
73.7
78.7
76.3
76.2
76.6
77.2
76.2
76.5
77.9
42.4
42.1
43.6
44.1
46.0
47.9
47.8
48.5
47.3
45.9
52.2
52.1
52.1
52.0
50.8
53.8
50.7
52.9
52.4
54.9
56.4
58.2
57.7
61.6
65.6
59.1
60.9
62.8
80.7
85.5
Source: Betson et al. ( 2011 ).
Note: Figures displayed here are for the 90 -percent confidence intervals. Confidence intervals express the uncertainty about the true WIC coverage rate.
97.4
97.5
6.
WIC Participants and Their Growing Need for Coverage
( 2001 ) suggest that these estimates are overstated, pointing to inherent selection and simultaneity bias in the studies.
administering and Improving WIC
Numerous administrative and outcome-based issues persist in a program with the size and complexity of WIC. These issues include the need to stretch WIC funding by implementing cost-containment measures and to ensure that
WIC produces positive nutrition outcomes.
WIC cost containment.
Over the past decade, WIC has been one of the fastest growing federal nutrition programs, and managing program costs has been key to its expansion.
Program administrators stretch program funds through cost-containment measures including state sole-source contracting for infant formula and other WIC foods.
Unlike other safety net programs, WIC does not require matching state funds. Federal administrators provide states with incentives to reduce WIC costs by establishing grants for
WIC food separate from WIC program administration. Federal regulations require each state establish a maximum payment to vendors for WIC food items (Neuberger and
Greenstein 2004 ).
State sole-source contracting with infant formula providers plays a vital role in ensuring that federal WIC dollars go further. In FY
2008 , infant formula rebates totaled $ 2 .
0 billion dollars, or a savings of nearly half of total actual WIC food expenditures (Oliveira,
Frazão, and Smallwood 2010 ). Infant formula rebates save enough program costs to cover one-quarter of the total WIC caseload
(Oliveira and Frazão 2009 ).
From 2000 through 2010 , the price of food at home has risen at an average annual rate of
2 .
6 percent per year, slightly outpacing growth in prices in general, which average 2 .
4 percent per year.
10 Since rising food costs strain program funds, many states only authorize WIC vendors that have lower food prices, require beneficiaries to purchase the lowest-cost WIC items (e.g., generic and store brand items), and negotiate rebates similar to those for infant formula with food manufacturers or suppliers.
Rising food prices also threaten to diminish the value of newly introduced cash value vouchers for fruits and vegetables.
While most states still provide paper vouchers for WIC benefits, it is expected that the transition to electronic benefits will help administrators monitor costs. The Healthy,
Hunger-Free Kids Act mandated the transfer to electronic WIC benefits by 2020 to improve administration. As of September 2011 , only five states and four tribal organizations had fully implemented a statewide WIC electronic benefits system (Food and Nutrition
Service 2011 b). States have received several grants to help them develop plans for transitioning to electronic benefits.
Improved nutrition outcomes. WIC aims to improve nutritional outcomes by increasing breastfeeding among WIC women, ensuring that WIC does not contribute to the increased prevalence of childhood obesity, and improving nutrition education and medical service referrals.
Historically, WIC participants have breastfed less than nonparticipants (Ryan and
Zhou 2006 ). The recent revisions to WIC food packages were intended to encourage partially breastfeeding women to increase the duration and intensity of breastfeeding, and
WIC now requires that local agencies highlight exemplary breastfeeding practices. The
Healthy, Hunger-Free Kids Act also awards performance bonuses for states with highest and most improved breastfeeding rates.
The rising incidence of childhood obesity has led some to question whether WIC participation could somehow be encouraging overeating. However, studies (Lin 2005 ;
Oliveira and Chandran 2005 ; Ver Ploeg,
Mancino, and Lin 2007 ) have found no evidence that childhood obesity is related to
WIC participation. Nevertheless, concerns about increasing childhood obesity played a part in revising WIC food packages to provide foods that are more nutritious and less likely to contribute to unhealthy caloric intake, including limiting the amount of juice and milk for young children.
summary
The WIC program provides supplemental food and services to some of the most vulnerable populations: low-income infants, young children, and pregnant and postpartum women. These supplemental foods supply the nutrients typically lacking in their diets.
Benefits come at a critical time, the early development of infants and children.
WIC has grown to be a central component of the federal food safety net, with half of all infants and a quarter of young children, pregnant women, and postpartum women receiving benefits. Coverage rates for the nation have slightly increased over the last decade. These rates vary across the country with the highest in Puerto Rico, Vermont, the District of Columbia, California, and
Minnesota and the lowest in Montana, Utah,
Colorado, Idaho, and Illinois.
Growing WIC enrollment represents a challenge to administrators as they seek to stretch WIC discretionary funding further. A number of cost-containment measures have been implemented, and it is likely that more will still need to be done to compensate for rising food costs and expanding WIC enrollment.
Studies suggest that WIC dollars translate into cost savings on health spending for the government, and new changes in WIC food packages should further improve health outcomes. Still, more needs to be learned about the effects of WIC foods and education on outcomes, especially given recent changes in participation and food package content.
•
7.
WIC Participants and Their Growing Need for Coverage
Notes
1 .
Note that administration expenses include the cost of all nonfood services provided by WIC, including nutrition education, breastfeeding support, and other government service referrals.
The Center on Budget and Policy Priorities estimated that actual program administration accounts for approximately 9 percent of federal
WIC costs (Neuberger 2011 ).
2 . For detailed estimates of WIC eligibility see
Betson et al. ( 2011 ).
3 . See Food and Nutrition Service ( 2011 a) for a summary of the Healthy, Hunger-Free Kids Act.
4 . The Healthy, Hunger-Free Kids Act mandated that states transfer to an electronic WIC benefit system by 2020 .
5 . As noted earlier, participation in Medicaid,
SNAP, TANF, or other state-administered programs can confer WIC eligibility. With the exception of Medicaid in some states, these programs have income eligibility standards below 185 percent of FPL. That is, most participating in other low-income programs would be eligible for WIC just on the basis of their income.
6 . Calendar year 2009 is the most recent year for which WIC coverage rate and eligibility estimates are currently available.
7 . The spike in the coverage rates in 2002 is due to a drop in the national-level infant eligibility estimate for that year. This is a noted anomaly in the WIC estimates time series data.
8 . These confidence intervals depict the level of uncertainty around each estimated coverage rate and are important for trying to compare state coverage rates. If a state coverage rate is within the confidence interval of another state’s rate, the two cannot be considered statistically different. For example, West Virginia and Delaware have different estimates of coverage, but since West Virginia’s rate falls within Delaware’s confidence interval, they are not significantly different statistically.
9 . See Betson et al. ( 2011 ) for details.
10 . Author’s calculations based on monthly, seasonally adjusted consumer price index
(CPI) data from the Bureau of Labor and
Statistics for the cost of food at home (Series
ID: CUSR 0000 SAF 11 and CUSR 0000 SA 0 ): http://www.bls.gov/cpi/.
references
Besharov, Douglas J., and Peter Germanis. 2001 .
Rethinking WIC: An Evaluation of the Women,
Infants, and Children Program.
Washington, DC:
American Enterprise Institute Press.
Betson, David, Michael Martinez-Schiferl, Linda
Giannarelli, and Sheila Zedlewski. 2011 . “Nationaland State-Level Estimates of Eligibility and
Program Reach, 2000 – 2009 .” Washington, DC:
U.S. Department of Agriculture, Food and
Nutrition Service. Republished http://www.urban.org/publications/ 412482 .html.
Coleman, Silvie, Ira P. Nichols-Barrer, Julie E.
Redline, Barbara L. Devaney, Sara V. Ansell, and
Ted Joyce. 2012 . “Effect of the Special Supplemental
Nutrition Program for Women, Infants, and
Chlldren (WIC): A Review of Recent Research.”
Washington, DC: U.S. Department of Agriculture,
Food and Nutrition Service.
Conor, Patty, Susan Bartlett, Michele Mendelson,
Kelly Lawrence, and Katerine Wen.
Dalaker, Joseph. 2001 . “Poverty in the United
States: 2000 .” Washington, DC: U.S. Census
Bureau.
DeNavas-Walt, Carmen, Bernadette D. Proctor, and Jessica C. Smith. 2011 . “Income, Poverty, and
Health Insurance Coverage in the United States;
2010 .” Washington, DC: U.S. Census Bureau.
Devaney, Barbara, Linda Bilheimer, and Jennifer
Schore. 1990 . “The Savings in Medicaid Costs for
Newborns and Their Mothers Resulting from
Prenatal Participation in the WIC Program.”
Washington, DC: U.S. Department of Agriculture,
Food and Nutrition Service.
2011
Participant and Program Characteristics
Washington, DC: U.S. Department of Agriculture,
Food and Nutrition Service.
Food and Nutrition Service.
———. 2011
September
2011 b. “WIC EBT Activity Map—
2011 .” http://www.fns.usda.gov/wic/ebt/EBTActivity
Map.pdf. (Accessed December 1 , 2011 .)
. “WIC
2010 .” a. “Summary of the Healthy, Hunger-Free Kids Act of 2010 .” http://www.fns.usda.gov/cnd/governance/legislation/
PL 111 296 _Summary.pdf. (Accessed December 1 , 2011 .)
———. 2011 d. “WIC Food Packages—Maximum
Monthly Allowances.” http://www.fns.usda.gov/wic/benefitsandservices/ foodpkgallowances.htm. (Accessed December 1 , 2011 .)
Lee, Bong Joo, Lucey Mackey-Bilaver, and Meejung
Chin. 2006 . “Effects of WIC and Food Stamp
Program Participation on Child Outcomes.”
Washington, DC: U.S. Department of Agriculture,
Economic Research Service.
Lin, Biing-Hwan. 2005 . “Nutritional and Health
Characteristics of Low-Income Populations: Body
Weight Status.” Washington, DC: U.S. Department of Agriculture, Economic Research Service.
Neuberger, Zoë. 2011 . “Claim Regarding High WIC
Administrative Costs Is False.” Washington, DC:
Center on Budget and Policy Priorities.
http://www.cbpp.org/cms/index.cfm?fa=view&id= 3514 .
Neuberger, Zoë, and Robert Greenstein. 2004 .
“WIC-Only Stores and Competitive Pricing in the
WIC Program.” Washington, DC: Center on
Budget and Policy Priorities.
Oliveira, Victor, and Ram Chandran. 2005 .
“Children’s Consumption of WIC-Approved Foods.”
Washington, DC: U.S. Department of Agriculture,
Economic Research Service.
Oliveira, Victor, and Elizabeth Frazão.
2009 . “The WIC
Program: Background, Trends, and Economic Issues,
2009 Edition.” Washington, DC: U.S. Department of Agriculture, Economic Research Service.
Oliveira, Victor, Elizabeth Frazão, and David
Smallwood. 2010 . “Rising Infant Formula Costs to the WIC Program: Recent Trends in Rebates and
Wholesale Prices.” Washington, DC: U.S. Department of Agriculture, Economic Research Service.
Ryan, Alan S., and Wenjun Zhou. 2006 . “Low
Breastfeeding Rates Persist among the Special
Supplemental Nutrition Program for Women,
Infants, and Children Participants, 1978 – 2003 .”
Pediatrics 117 ( 4 ).
U.S. General Accounting Office. 1992 . “Early
Intervention: Federal Investments Like WIC Can
Produce Savings.” Washington, DC: U.S. General
Accounting Office.
———. 2011 c. “About WIC.” http://www.fns.usda.gov/wic/aboutwic/mission.htm.
(Accessed December 1 , 2011 .)
Ver Ploeg, Michele, Lisa Mancino, and Biing-Hwan
Lin. 2007 . “Food Nutrition Assistance Programs and Obesity: 1976 – 2002 .” Washington, DC: U.S.
Department of Agriculture, Economic Research Service.
8.
WIC Participants and Their Growing Need for Coverage
about the author
Michael Martinez-Schiferl is a research associate with the
Income and Benefits Policy
Center at the Urban Institute.
Income and Benefits Policy Center
www.urban.org/center/ibp/
The Income and Benefits Policy Center studies how public policy influences the behavior and economic well-being of families, particularly the disabled, the elderly, and those with low incomes.
Scholars look at income support, social insurance, tax, child-support, and employee-benefit programs.
The author would like to thank Sheila Zedlewski and Pam Loprest at the Urban Institute and
David Betson at the University of Notre Dame for providing helpful comments on an earlier draft.
Nonetheless, the author is responsible for the content.
The views expressed are those of the author and do not necessarily reflect those of the Urban Institute, its trustees, or its funders. Permission is granted for reproduction of this document, with attribution to the Urban Institute.
Copyright © April 2012 urBaN INsTITuTe
2100 M street, NW ●
Washington, dC 20037-1231
(202) 833-7200 ● publicaffairs@urban.org ● www.urban.org