Outline Ankylosing Spondylitis in 2014! 12/2/14
advertisement

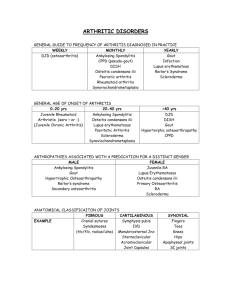
12/2/14 Outline Ankylosing Spondylitis in 2014! Lianne S. Gensler, M.D.! Associate Professor of Medicine! Director, Ankylosing Spondylitis Clinic! UCSF Rheumatology! • Ankylosing Spondylitis defined • Epidemiology in the U.S. • Assessment & diagnosis in primary care • Initial treatment & treatment advances • Comorbidities to remember ICD9 code – clinical diagnosis Diagnosis vs. Classification • Diagnostic criteria are developed to be highly sensitive to identify as many patients with the disease as possible • The value of diagnostic tests/ parameters depends on the prevalence of the disease (pretest probability) • Should allow for flexibility in diagnostic confidence (definite, probable, possible) • Applied to the individual patient • Classification criteria are developed to define a homogeneous group for the purpose of research • High specificity to avoid misclassification • No dependence of disease prevalence as patients are already diagnosed • Applied to a group Evidence based medicine Outline • Ankylosing Spondylitis defined • Epidemiology in the U.S. • Assessment & diagnosis in primary care • Initial treatment & treatment advances • Comorbidities to remember 1 12/2/14 Age = 26 years! Bilateral THAs! Spondyloarthritis: a family of diseases 30-40%! Acute Anterior Uveitis Ankylosing Spondylitis: sacroiliitis & spondylitis Inflammatory Bowel Disease PSORIASIS 10%! American College of Rheumatology, Image Bank (#99-07-0014 ) 8-10%! Subclinical Colitis ! 25-60%! Lin P et al., PLoS One. 2014; 9(8) Outline • Ankylosing Spondylitis defined • Epidemiology in the U.S. • Assessment & diagnosis in primary care • Initial treatment & treatment advances • Comorbidities to remember Reveille JD Nat. Rev. Rheumatol. (8)296–304 (2012)! 2 12/2/14 HLA B27 in the U.S. population! NHANES 2009-2010 • 19.2% chronic axial pain • In patients with chronic axial pain, 28-35.5% had IBP • Prevalence of IBP 5-6% • Between non-Hispanic white persons and non-Hispanic • black persons: (5.9 vs 3.3%; t=3.99, p<0.01). Weisman MH et al., Ann Rheum Dis. 2013 Mar;72(3):369-73. • Self-reported prevalence of AS = 0.55 Reveille JD et al., Arth Rheum Vol. 64, No. 5, May 2012, pp 1407–1411! Reveille JD et al, Arthritis Care & Res. Vol. 64, No. 6, June 2012, pp 905–910 Axial SpA in Chronic back pain populations • Primary Care clinics (n = 364) • In chronic low back pain patients 20 to 45 yrs of age Van Hoeven L., Arthritis Care Res (Hoboken). 2014 Mar;66(3):446-53. ! 3 12/2/14 Outline Case ! • Ankylosing Spondylitis defined • Epidemiology in the U.S. • Assessment & diagnosis in primary care • Initial treatment & treatment advances • Comorbidities to remember • 24 year old man with low back pain that started 7 years ago. He has seen several chiropractors and an orthopedic surgeon with ongoing symptoms.! • Initially alternating buttock pain, worse in the morning with associated am stiffness lasting 60 minutes. Pain would awaken him from sleep around 3am. The pain is made better with ibuprofen and exercise and he feels almost normal by midday.! Your next step is to…! Inflammatory Back Pain: hallmark feature ! Feature! Feature Insidious onset ! Insidious onset Odds Ratios! Odds Ratios 12.7 12.7! Pain (withimprovement improvement upon getting Painat at night night (with upon getting up) up) ! 20.4 20.4! Ageat at onset onset <40 years Age <40 years ! 9.9 9.9! Improvement with exercise 23.1 Improvement with exercise ! No improvement with rest No improvement with rest ! 7.7 23.1! 7.7! Sensitivity 79.6% & Specificity 72.4%! Positive LR = 79.6/(100-72.4) = 2.9 ~ Probability = 14%! Sieper J, et al. Ann Rheum Dis. 2009; Rudwaleit M, et al. Ann Rheum Dis. 2009; Ozgocmen S, Akgul O, Khan MA. J Rheumatol. 2010! 1. Check HLA B27! 2. Check ESR/CRP! 3. Order imaging study! 4. Obtain additional history! Evaluate for other symptoms:! peripheral joint pain, heel pain, bloody stools/ diarrhea, rashes! Evaluate for other diagnoses:! Acute anterior uveitis, IBD, Psoriasis! Assess Family history:! 20% AS pts will have a FDR with AS! ! 4 12/2/14 Probability of Spondyloarthritis Using Multiple Clinical and Lab Features! Case cont.! • The patient tells you his father has Ankylosing Spondylitis! • How does this additional data change your assessment?! AS in Chronic Low Back Pain Population 5%! Inflammatory back pain ! LR 3.1! Heel pain (enthesitis) ! LR 3.4! Peripheral arthritis ! LR 4.0! Dactylitis ! LR 4.5! Acute anterior uveitis LR 7.3! Positive Family history LR 6.4! Good response to NSAIDs LR 5.1! Elevated ac. phase reactants HLA-B27 MRI ! Pr = 98%! LR 2.5! ! LR 9.0! ! LR 9.0! LR 101 à ! Probability =! 84%! ! ! ! ! ! LR 15.81 à! Probability = 45%! 3.1 multiplied by 5.1 gives a likelihood product of 15.81. fam hx à LR 15.81 x 6.4 = 101 ! Rudwaleit M, et al. Arthritis Rheum 2005; 52:1000-8! Slide courtesy of Walter P. Maksymowych, with permission 5 12/2/14 Axial SpA Epidemiology! Prevalence ~ 1% Axial SpA Ankylosing Spondylitis! Non-radiographic Axial SpA! : :! (Milder disease ! Or ! early disease)! Radiographic ! sacroiliitis! 1 : 2-3 HLA B27 85-95%! Age of onset 16 – 40! ! Bamboo spine! DAMAGE! Helmick CG et al, Arthritis Rheum 2008; 58: 15-25! Reveille JD et al., Arth & Rheum Vol. 64, No. 5, May 2012, pp 1407–11! Reveille JD et al., Arthritis Care Res. 2012; 64:905! Inflammatory ! Back pain! AP pelvis! L spine MRI misses SI joints! 6 12/2/14 AS Physical Exam! Occiput to wall measure (normal = 0cm) Chest expansion score (normal = ≥ 1.9 cm) Anterior lumbar flexion (modified Schober test) Threshold = 2.0 cm Assassi S et al., Arthritis Rheumatol Vol. 66, No. 9, September 2014, pp 2628–2637 AS Physical Exam! Modified Schober test or Anterior Lumbar Flexion (normal ≥ 2cm increase) Thoracic (Chest) Expansion Threshold = 1.9 cm Assassi S et al., Arthritis Rheumatol Vol. 66, No. 9, September 2014, pp 2628–2637 7 12/2/14 Outline • Ankylosing Spondylitis defined • Epidemiology in the U.S. • Assessment & diagnosis in primary care • Initial treatment & treatment advances • Comorbidities to remember Case The patient returns to see you with a new diagnosis of AS. He is most bothered by the night pain and has 90 minutes of morning stiffness. A rheumatology appointment is scheduled for 6 weeks. He asks if you can prescribe something while he waits to be seen. When I was an intern…! • Only drugs approved for AS were NSAIDs! • No biologics shown to be effective in AS! ! 8 12/2/14 AS: Treatment! NSAIDs! Axial disease only! NSAID × NSAIDs TNF inhibitors sulfasalazine If peripheral ! disease! • First line therapy! • NSAIDs better than placebo! • No difference in efficacy across NSAIDs (FDA approved)! ! Response to NSAIDs! 80 60 40 20 0 Ankylosing Spondylitis! Mechanical back pain! Physical Therapy Braun J, et al.,, Ann Rheum Dis 2011; 70: 896-904! van der Heijde D, et alAnn Rheum Dis 2011; 70:905-08! Boulos P et al., Drugs 2005;65 (15):2111-27! Amor B et al., Rev Rhum Engl Ed. 1995 Jan;62(1):10-5! ! AS: Efficacy of TNFα inhibitors! Do TNFi slow down damage? ASAS 40 Responses in 5 separate trials! TNF inhibitor! 47 45 Etanercept 13 adalimumab 48 44 39 14 Placebo! 15 12 Infliximab Golimumab Davis et al, Arthritis & Rheum, 48 (11), Nov 2003: 3230-3236! Van der Heijde et al., Arthritis & Rheum, 54, 7. July 2006: 2136-2146 [ATLAS]! Van der Heijde et al., Arthritis & Rheum, 52, 2. Feb 2005: 582-591 [ASSERT]! Inman et al., Arthritis & Rheum, 58 (11) Nov 2008: 3402-12 [GO-RAISE]! Landewe et al., Annals Rheum Dis. 2014 Jan;73(1):39-47 [RAPID-axSpA ]! ! 16 Certolizumab Van der Heijde et al., Arth Res & Ther 2009 9 12/2/14 TNFi use: OR: 0.52; CI: 0.30-0.88; p=0.02 Benefit shown after 3.8 years Haroon N et al., Arth Rheum 2013 Flare after withdrawal Haroon N et al., Arth Rheum 2013 Glucocorticoids not recommended in AS! • Double blind RCT 2 week trial! • Prednisolone 20mg vs. 50mg vs placebo! • Only 50mg/day à short-term response sig higher than placebo! 50mg 20mg placebo Haibel et al. Barkam et al. Song et al. Sieper et al. Arthritis Rheum Ann Rheum Dis Ann Rheum Dis Ann Rheum Dis 2013; 65: 2211-3 2009; 68 (Suppl. 3):72 2012; 71(7): 1215-15 2013 Jun 5 Haibel H, et al. Ann Rheum Dis 2013;0:1–4! 10 12/2/14 Smoking Physical Therapy & Exercise! • • • • • 1. 2. 3. 4. 5. 6. PT meta-analysis showing benefit! Exercise improves function! Tai chi improves disease activity & flexibility! Aerobic & pulmonary exercise! Interaction between exercise & TNFα inhibitors to improve long term function! Dagfinrud H et.al., 2008; Cochrane Collaboration! Brophy S et al., Semin Arth Rheum 2013 Jun;42(6):619-26! Lee EN et al., 2008 Evid Based Complement Alternat Med 5, 457–62! Fernandez-de-Las-Penas C, et al. (2006) Phys Rehabil Med 18, 39–61.! Ince G et al., Phys Ther 86, 924–35! Patterson S et al., ACR 2014! • Earlier onset of Inflammatory Back Pain • ñ inflammation • ñstructural damage (x-ray) • ñradiographic progression (dose-related) 1. Chung HY et al., Annal Rheum Dis 2012; 71:809-816 2. Ward MM et al., Arth Care & Res 2009; 61 (7): 859-866 3. Poddubnyy D et al., Arth Rheum 2012; 64(5): 1388-1398 4. Haroon N et al., Arth Rheum 2013; 65(10):2645-54 ! ! Outline Extra-articular manifestations Depression 30% • Ankylosing Spondylitis defined • Epidemiology in the U.S. • Assessment & diagnosis in primary care • Initial treatment & treatment advances • Comorbidities to remember Arachnoiditis Cauda equina syndrome Pulmonary Fibrosis (apical) Restrictive lung disease Sleep apnea IgA nephropathy Amyloidosis Aortitis First Degree AVB Aortic Insufficiency Ischemic heart disease Osteoporosis Vertebral fractures & pseudo-fractures Bremander et.al., Arthritis Care Res, 63:550, 2011 Klingberg et.al., Arthritis Res Ther, 14:R108, 2012 Berdal et.al., Arthritis Res Ther, 14:R19, 2012. Rudwaleit et al. Best Practice & Research Clinical Rheumatology 20:451, 2006 11 12/2/14 Bone Health : AS! • Osteoporosis! • Osteoporosis! – 21% age > 50! • Low Bone mass! – 21% age > 50! • Low Bone Mass! – 44%! – 44%! ! ! 28 year old man with 3 years of disease ! ! Klingberg et al., Arthritis Res Ther, 14: R108,2012 ! et al., Int J Rheum Dis 14:68-73! Vasdev Ghoslani et al., Bone 2009 44:772-77 !! ! ! ! ! ! !! Bone Health : AS! ! ! !! ! ! ! TNF inhibitors effects on BMD ! ! ! ! Klingberg et al., Arthritis Res Ther, 14: R108,2012 ! et al., Int J Rheum Dis 14:68-73! Vasdev Ghoslani et al., Bone 2009 44:772-77 !! ! ! ! ! 43 year old man with long standing AS ! ! !! ! ! ! ! !! Case • 50 year old man with AS presents with acute on chronic neck pain • Minor fall 2 months before N.N. Haroon et al., Seminars in Arthritis and Rheumatism 44(2014)155–161 12 12/2/14 Fracture in AS! Fracture in AS! ! 2012 2011 2 3 2 4 3 4 5 6 1 year • Vertebral fractures in 30% Normal BMD (11.1%)! ! • Population studies :OR 3.26 -7.7! – Men > women! – ↑after the 5 yrs of diagnosis! ! • Fracture risk: Low BMI, Rigidity, balance & fall risk! ! • C spine fracture & fall, MVA & ETOH! Cooper et al., J Bone Miner Res 7: 221-227! Cooper et al., J Rheumatol 21:1877-1882! Vosse et al., Annals Rheum Dis 68:1839,2009! Wysham KD et al. ACR 2014! ! Clinical variables associated with mortality in discharged AS patients: multivariable analysis Variable Sepsis Pneumonia Cardiovascular disease C-­‐Spine Fracture w/ SCI C-­‐Spine Fracture w/o SCI Thoracic spine fracture Lumbar spine fracture Lymphoma in TNFα inhibitor users Odds Ra-o 95% CI p-­‐value 7.95 2.00 1.35 13.82 2.81 0.99 2.02 5.86-­‐10.79 1.47-­‐2.73 1.03-­‐1.77 8.23-­‐23.20 1.61-­‐4.88 0.56-­‐1.73 0.92-­‐4.45 <0.0001 <0.0001 0.031 <0.0001 <0.0001 0.960 0.078 Adjusted for all variables Wysham KD, ACR 2014 Hellgren K et al., Arthritis Rheumatol. 2014 May;66(5):1282-90 13 12/2/14 Summary Age = 26 years • Genetics & Microbiome • U.S. prevalence ~ 0.55 -1.4 • Consider a diagnosis with inflammatory axial pain • Start NSAIDs (+/- PT) if no contraindications while referral pending • Smoking cessation • Osteoporosis & Fracture – Screen for osteoporosis & Fall assessment American College of Rheumatology, Image Bank (#99-07-0014 ) Acknowledgements 2014 2024 2034 2034 2044 2032 Patients American College of Rheumatology, Image Bank (#99-07-0014 - adapted) 14