Chikungunya Retinitis Dr Padmamalini Mahendradas Head, Uveitis and Ocular Immunology Narayana Nethralaya
advertisement

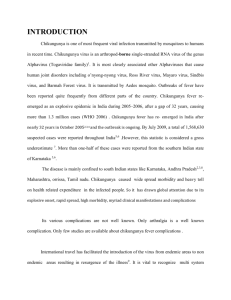
Chikungunya Retinitis Dr Padmamalini Mahendradas Head, Uveitis and Ocular Immunology Narayana Nethralaya Bangalore. Ocular History 45 years female • presented first on 12/2006 • decreased vision in the OS since 15 days • eye pain since 4 days • Chikungunya fever 4 weeks back Examination OD OS • EOM Normal Normal • Vision 6/60, N18 CF 1 mtr • Anterior segment Normal RAPD • IOP 10 mmHg 10 mmHg Fundus Examination: Right Eye Fundus and red-free photograph of the right eye shows multiple areas of retinal opacification suggestive of retinitis with retinal hemorrhages Fundus Examination : Left Eye Fundus photograph shows vitreous haze 1+, mild hyperemic disc with multifocal retinitis and hemorrhages in the posterior pole of the left eye and red-free photograph also showing the presence of retinitis and hemorrhages in the left eye. Investigations • • • • • • • • • • • Hb 10.5 gm% , TC & DC – within normal limits ESR-20 mm /hr Malarial Parasite -absent Dengue rapid test - negative Leptospirosis - negative Chest x-ray - normal TPHA- non reactive Toxoplasma IgM & IgG - negative HIV I &II - negative Mantoux - negative Chikungunya IgM - positive Fundus Fluorescein Angiography Early Phase Capillary non perfusion corresponding to the area of retinal whitening with vascular leakage in the posterior pole Hyperfluorescence with capillary non perfusion in the macular area Fundus Fluorescein Angiography Late Phase Hyperfluorescence due to vascular leakage Leakage from the optic disc with widespread vasculitis and staining of retinal infiltrates Clinical Diagnosis • Bilateral Multifocal Retinitis due to Viral etiology (? Chikungunya ) was made Treatment Systemic acyclovir 800 mg 5 times a day was started with systemic corticosteroids (oral prednisolone 60 mg/day) with Chikungunya positive Ig M titer and after ruling out other infections Acyclovir was stopped Oral prednisolone 60mg/day was continued for one week and then it was tapered over a period of 8 weeks. H2 receptor blocker (Ranitidine 150 mg bd) & calcium supplements for 8 weeks Follow up: after 6 Months Resolved retinitis with pigment epithelial changes at the foveal area VA 6/9, N6. Temporal pallor of the disc with pigment epithelial changes VA CF 1 meter ,<N36 Discussion • Chikungunya retinitis may morphologically mimic herpetic viral retinitis • the history of fever, joint pains, and skin rash before the onset of visual symptoms is helpful in the diagnosis, particularly in endemic regions. Mahendradas P, Ranganna SK, Shetty R, Balu R, et al. Ocular Manifestations Associated with Chikungunya. Ophthalmology, 2007; 115:287-291. Discussion • Ocular manifestations may be due to inflammatory response to Chikungunya virus or direct ocular involvement by the virus. • We were able to obtain serologic evidence in our case and molecular diagnostic test such as RT- PCR could not be done due to non availability of the test in 2006. Discussion • Strong clinical association was established based on the temporal association between the systemic manifestations, ocular manifestations & positive serology allowing us to make a diagnosis of Chikungunya retinitis. • Patients with retinitis showed improvement with corticosteroids Conclusion • Chikungunya can cause ocular manifestation such as retinitis. • Ophthalmologists need to be aware of these features in geographic regions Asia, Africa and French reunion where the chikungunya fever is prevalent.