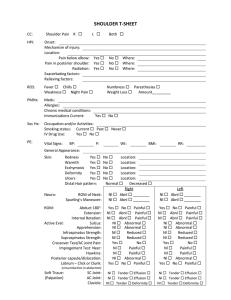
HIP T-SHEET
advertisement

HIP T-SHEET R L CC: Hip Pain HPI: Onset: Mechanism of injury: Location: Groin Radiation: Yes Exacerbating factors: Relieving factors: Both Posterior Lateral No Where: ROS: Fever Chills Weakness Night Pain Numbness Paresthesias Weight Loss Amount_________ PMHx: Prior malignancy: Yes No Meds: Hx of back problems: Yes No Allergies: Chronic medical conditions: Immunizations Current: Yes No Soc Hx: Occupation and/or Activities: Smoking status: Current Past Never IV Drug Use: Yes No PE: General Appearance: Gait: Normal Skin: Redness Yes No Location: Warmth Yes No Location: Ulcers Yes No Location: Distal Hair pattern: Normal Decreased Right Vascular: Neuro: ROM: Antalgic Unable to bear weight Femoral Pulse: Nl Dorsalis Pedis Pulse: Nl Post Tibialis Pulse: Nl Capillary Refill: Normal Left Absent Absent Absent Slow Nl Nl Nl Normal Absent Absent Absent Slow Painful Painful Painful Painful Nl Nl Nl Nl Painful Painful Painful Painful Straight Leg Raise: Knee Jerk Reflex (L4): Toe Raise (L5): Ankle Jerk (S1): 2-point discrimination: Internal Rotation: Nl External Rotation: Nl Flexion: Nl Extension: Nl Active Eval: SI Joint (FABER): Impingement (McCarthy): Soft Tissue: (Palpation) Palpable Lymph Nodes: Lateral Hip (tender): Hernia: Testicular Exam: Nl Painful Nl Painful Nl Painful Nl Painful Yes No Yes No Yes No Nl Abnormal Yes No Yes No Yes No Nl Abnormal TREAT APPROPRIATELY Trochanteric Bursitis ................... 726.5 Osteoarthritis ............................ 715.95 ITB Syndrome ............................ 728.89 SI Joint Pain ............................... 719.45 Sprain/Strain ............................... 843.x Low Back Pain ............................. 724.2 TREAT WITH CLOSE FOLLOW-UP Soft Tissue CALL CONSULTATNT THAT DAY Can’t walk AVN Fracture CONSULT OR REFER OA, failed conservative treatment Suspected fracture Diagnosis unknown Plan: Xray / Imaging Laboratory Eval NSAIDs Acetaminophen Other PRICE Protocol Physical Therapy Disposition: Treatment initiated: Follow-up __________ weeks Treatment / Work up Initiated: Follow-up ≤ 1 week __________ days Immediate call to Dr. Consultation initiated with Dr. Referral to Dr.