Learning from Success and Failure
advertisement

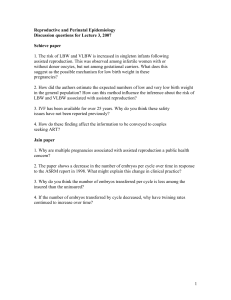
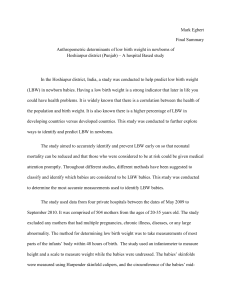
02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 185 Learning from Success and Failure in Psychosocial Intervention: An Evaluation of Low Birth Weight Prevention Trials QIAN LU, MICHAEL C. LU, & CHRISTINE DUNKEL SCHETTER University of California, Los Angeles, USA is a doctoral student in training in Social and Health Psychology at UCLA. She received her MD degree from Shandong Medical University. Her research focuses on the evaluation of health interventions, and health interventions for ethnic minorities. QIAN LU M I C H A E L L U is an Assistant Professor in Obstetrics and Gynecology and in the School of Public Health at UCLA. Dr Lu received his MD degree from the University of California, San Francisco, and MPH and MS degrees from the University of California, Berkeley. His current work is on ethnic disparities in maternal and child outcomes. C H R I S T I N E D U N K E L S C H E T T E R is a Professor of Psychology and Director of Health Psychology at UCLA where she has been on the faculty since 1983. She received her PhD from Northwestern University and was a postdoctoral fellow at the University of California, Berkeley. Her research concerns stress processes in pregnancy, social support, coping and health outcomes. COMPETING INTERESTS: ADDRESS. None declared. Correspondence should be directed to: P R O F. C H R I S D U N K E L S C H E T T E R , Department of Psychology, University of California Los Angeles, 405 Hilgard Ave, Los Angeles, CA 90095–1772, USA. [email: dunkel@psych.ucla.edu] Journal of Health Psychology Copyright © 2005 SAGE Publications London, Thousand Oaks and New Delhi, www.sagepublications.com Vol 10(2) 185–195 DOI: 10.1177/1359105305049763 Abstract The object of the study was to evaluate the research designs of social support interventions for prevention of low birth weight (LBW). A literature search of published articles identified 12 randomized controlled trials of social support to prevent LBW birth. These were evaluated using specific methodological criteria for effective intervention research. Only one study showed a significant reduction in LBW. However, none of the studies met all of the proposed criteria for rigorous intervention research. It is premature to conclude that social support interventions are ineffective in preventing LBW. Specific recommendations for future intervention research design are outlined. Keywords intervention, low birth weight (LBW), pregnancy risk, psychosocial, social support 185 02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 186 JOURNAL OF HEALTH PSYCHOLOGY 10(2) L OW B I RT H weight (LBW) is a leading cause of infant mortality and morbidities in the USA (Mathews, Menacker, & MacDorman, 2003). Limited success in reducing LBW through medical interventions (Lu, Tache, Alexander, Kotelchuck, & Halfon, 2003), coupled with accumulating evidence that links psychosocial factors to pregnancy outcomes (Paarlberg, Vingerhoets, Passchier, Dekker, & van Geijn, 1995) have led to interest in preventing LBW by implementation of psychosocial interventions. However, most programs that offer social support during pregnancy have not been particularly effective in preventing LBW (Hodnett & Fredericks, 2003; Stevens-Simon & Orleans, 1999). The primary aim of this article is to evaluate the design of these intervention studies. We contend that because most studies: (1) have not been theory-driven; (2) have not had effective risk screening; (3) have not matched interventions to risks; and (4) have not tested process variables, it may be premature to conclude that psychosocial interventions are ineffective in preventing LBW. In this article we propose a new model of psychosocial intervention research for the prevention of LBW. Methods We conducted a literature search for original research, systematic reviews, meta-analyses and commentaries that were published in the English language from 1960 to 2004 in computerized databases, specifically, Pubmed, PsycInfo and the Cochrane Library. Keywords used to conduct the search included ‘low birth weight’, ‘preterm’, ‘randomized trials’, ‘prenatal care’, ‘social support’ ‘psychosocial intervention’ ‘psychological intervention’ and/or ‘prevention’. Additionally, the reference lists of all qualifying articles and several recent reviews (e.g. Hodnett Screen population at risk for LBW & Fredericks, 2003; Stevens-Simon & Orleans, 1999) were examined for additional studies not identified through the database search. Our search generated 2279 articles. All abstracts were reviewed, and all articles that could not be conclusively excluded based on the abstract were retrieved to determine eligibility. The following criteria were used to select interventions to be included in this review: (1) the intervention must be a randomized controlled trial (RCT); (2) the intervention must be aimed at preventing LBW; and (3) the intervention must be mainly psychosocial in nature. We excluded interventions that were primarily medical (e.g. screening and treatment of asymptomatic bacteriuria) or nutritional in nature. We also exclude smoking cessation interventions even if they included psychosocial components. Based on these criteria, 12 randomized controlled trials were included in our review. These 12 studies were evaluated using a new model for LBW prevention intervention research. The traditional model of psychosocial intervention consists of three steps: screen the population at risk for LBW; provide psychosocial support to at-risk populations; and then compare LBW rates between intervention and control groups (Fig. 1). This traditional model has several pitfalls. First, the intervention is often not theory-driven. Without a predictive model linking intervention to outcome, it is sometimes difficult to know why, for whom and under what circumstances the program works or does not work (Drotar, 2002). Second, risk screening is based on risk factors for LBW, no matter whether or not they are modifiable by psychosocial interventions. Third, because some subjects are selected based on medical risks rather than psychological risks for LBW, psychosocial interventions may prove inappropriate and ineffective. Lastly, the Provide psychosocial support Figure 1. Traditional model of psychosocial intervention for LBW prevention. 186 Assess outcomes (LBW) 02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 187 LU ET AL.: LEARNING FROM SUCCESS AND FAILURE traditional model often fails to measure process variables. The term process variables, as used here, refers to variables mediating the effects of interventions (Aiken, 1999), and is used interchangeably with the terms ‘mediators’ in this article. Testing process variables allow the investigators to better understand the processes by which the intervention produces its effect, or the reasons for the absence of any effects. To address these pitfalls, we propose a new model of psychosocial intervention research for LBW prevention. Elaborating on a model developed by Aiken (1999), and West and Aiken (1997), our model consists of five stages. The first stage is to construct a predictive model that is empirically supported. The second stage is to screen population based on risk factors that are modifiable by psychosocial intervention. The third stage is to match interventions to risks. Psychosocial support should be provided to women and families at increased psychosocial risk, but not necessarily increased medical risk, for LBW. The fourth stage is to test process variables. Excellent examples of testing process variables exist in the literature for mammography screening (Aiken, West, Woodward, Reno, & Reynolds, 1994) and other issues such as AIDS prevention (Fisher, Fisher, Misovich, Kimble, & Malloy, 1996) but this approach has yet to be applied to LBW prevention. Statistical testing of mediators is beyond the scope of this article and can be read in Aiken et al. (1994) and Baron and Kenny (1986). The final stage is to assess outcomes (see Fig. 2). Thus the new model improves on the traditional model by: (1) calling for a priori development of a predictive model; (2) limiting risk screening to modifiable psychosocial risk factors; (3) matching psychosocial interventions Develop a predictive model Screen population based on modifiable psychosocial risk factors to psychosocial risks for LBW; and (4) testing process variables. Based on this new model, we established seven criteria for evaluating the design of psychosocial intervention research for LBW prevention: 1. Did the study describe a predictive model? 2. Did the study evaluate the effectiveness of risk screening? 3. Was the risk screening effective in identifying women at risk for LBW? 4. Did the study target risk factors modifiable by psychosocial interventions? 5. Did the study test process variables? 6. Did the intervention modify the process variables? 7. Did the study evaluate the relationship of process variables to outcome (LBW)? Results Table 1 summarizes the characteristics of the 12 studies included in our review. All studies offered social support as a single intervention or the centerpiece of a multi-component prenatal care intervention with a major goal of preventing LBW. Five studies also aimed to prevent preterm delivery (PTD), one of the twin contributors to LBW (the other being intrauterine growth restriction (IUGR) or fetuses that are small-for-gestational-age (SGA), defined as fetal or birth weight below the 10th percentile for a given gestation) (Kitzman et al., 1997; Klerman et al., 2000; Moore et al., 1998; Olds, Henderson, Tatelbaum, & Chamberlin, 1986; Villar et al., 1992). Four studies had other aims such as preventing child maltreatment (McLaughlin et al., 1992) or improving developmental outcomes or pregnancy outcomes other Match interventions to risks Test process variables Assess outcomes (LBW) Figure 2. New model of psychosocial intervention for LBW prevention. 187 C A L L L B W P T D O T H M E D P S Y S E S B E H + + + + + + + + + + + + + + + + – + + + + + + + + + + _ + + + + + + Content of support Outcome (% LBW) A P P I N F E M O E D U Intervention group (%) Control group (%) p value + + + + + + + + + + 12.5 10.9 15 9.1 8.7 10.5 10 14.0 19 19 11.2 14 14 22.4 9.4 7.5 9 11.6 22 20.5 NS NS NS p = 0.005 NS NS NS NS NS NS + 8.8 5.8 8.6 2.6 + + + H O M E + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + I N S + + + + NS NS Notes: Goal of intervention: LBW = low birth weight (defined as weight <2500g), PTD = preterm delivery, OTH = others goals Study population: W = White, AA = African American, LA = Latina American Risk screening based on categories of risk factors: MED = medical, PSY = psychological, SES = socioeconomic status, BEH = behavioral; ‘–’ signifies risk as exclusion criteria, ‘+’ signifies risk as inclusion criteria Format of social support: CALL = telephone call, HOME = home visit; APP = additional appointment Content of social support: INF = informational support (information about available community services, signs of medical complications of pregnancy); EMO = emotional/relational social support (provide emotional support directly or encourage emotional support from existing social network); INS = instrumental social support (help directly with housing, shopping, other domestic work); EDU = health education Outcome defined as percent LBW: NS = non-significant Page 188 Spencer et al. (1989) Olds et al. (1986) Format of support 3:40 pm Ethnicity AA 77% AA 92% AA AA LA AA AA & W W 95% W 45% W & 53% AA Non-Asian W Risk screening 21/1/05 Author Klerman et al. (2000) Moore et al. (1998) Kitzman et al. (1997) Norbeck et al. (1996) Villar et al. (1992) Graham et al. (1992) McLaughlin et al. (1992) Rothberg & Lits (1991) Oakley et al. (1990) Heins et al. (1990) Goal 02 Qian Lu (bc/d) Population JOURNAL OF HEALTH PSYCHOLOGY 10(2) 188 Table 1. Characteristics of randomized controlled trials of psychosocial interventions for the prevention of LBW 02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 189 LU ET AL.: LEARNING FROM SUCCESS AND FAILURE than LBW and PTD (Kitzman et al., 1997; Klerman et al., 2000; Olds, Henderson, Tatelbaum, & Chamberlain, 1986). Most of the studies recruited low-income women or African-American women who were at high risk of LBW. Among the twelve studies, three prevention programs recruited solely African-American women (Graham, Frank, Zyzanski, Kitson, & Reeb, 1992; Klerman et al., 2000; Norbeck, Dejoseph, & Smith, 1996), and two studies recruited primarily African Americans (Kitzman et al., 1997; Moore et al., 1998). Two studies had about half African Americans and half Whites (Heins, Webster, McCarthy, & Melvin, 1990; McLaughlin et al., 1992), and three studies had primarily or solely Whites (Oakley, Rajan, & Grant, 1990; Olds et al., 1986; Rothberg & Lits, 1991). One study was conducted with primarily Whites in Manchester, England (Spencer, Thomas, & Morris, 1989), and another study was conducted with Latina Americans (Villar et al., 1992) (Table 1). All of the 12 studies screened participants based on risk factors, except the Olds et al. (1986) study in which any women who asked to participate were allowed to enroll in the study. Risk factors in the studies can be classified into four categories: medical, psychological, socioeconomic and behavioral (Table 1). The intervention groups in these studies were provided with various formats of social support, such as telephone calls (Moore et al., 1998), home visitations from nurses or social workers (Graham et al., 1992; Kitzman et al., 1997; McLaughlin et al., 1992; Olds et al., 1986; Spencer et al., 1989; Villar et al., 1992), additional face-to-face appointment in clinics (Heins et al., 1990; Klerman et al., 2000; Rothberg & Lits, 1991) or a combination of telephone calls and home visits (Norbeck et al., 1996; Oakley et al., 1990). The contents of social support provision included informational support to help to recognize signs and symptoms of pregnancy complications and provide information about the utilization of local services; emotional support to enhance the existing social network and reduce stress (Norbeck et al., 1996); instrumental support to directly support domestic tasks (Spencer et al., 1989); health education including nutrition education and smoking cessation; and a combination of two or three of these intervention components (Graham et al., 1992; Heins et al., 1990; Klerman et al., 2000; McLaughlin et al., 1992; Moore et al., 1998; Oakley et al., 1990; Olds et al., 1986; Rothberg & Lits, 1991; Spencer et al., 1989; Villar et al., 1992). The control groups in these studies received standard or usual care, except for two prevention programs that offered free transportation to the control group (Kitzman et al., 1997; Olds et al., 1986). Only one (Norbeck et al., 1996) of the twelve studies showed a significant reduction in LBW rates (Table 1). Table 2 summarizes our evaluation of the intervention designs. Five of the twelve trials (Graham et al., 1992; Heins et al., 1990; Klerman et al., 2000; Moore et al., 1998. Norbeck et al., 1996) developed a predictive model, or at least had a simple predictive hypothesis (column 2). Only two studies (Graham et al., 1992; Klerman et al., 2000) evaluated the effectiveness of their risk screening, none of which actually were effective (column 3). We evaluated the effectiveness of risk screening for the remaining nine studies by observing the LBW rates in the control groups. If the risk screening was effective, then the LBW rate in the control groups (with no intervention) should be substantially higher than that in the general population. That is, we would expect LBW rates in the control groups of greater than 7 percent in studies with predominantly White population and 14 percent in studies with predominantly African-American study population (Mathews, Menacker, & MacDorman, 2003). For the two studies (Heins et al., 1990; McLaughlin et al., 1992) with about even population admixture of African Americans and Whites, the LBW rate in the control group should be substantially higher than 10.5 percent if risk screening was effective. For the study by Spencer et al. (1989), we would expect the LBW rate in the control group of greater than 10.2 percent, the LBW rate in the general population in Manchester at the time of the study. Similarly, for the study by Villar et al. (1992) with Latina Americans, the LBW rate of 9.4 percent in the control group was substantially lower than the expected rate of 15 percent. As Table 2 illustrates, only four of the twelve studies (Heins et al., 1990; Norbeck et al., 1996; Oakley et al., 1990; Rothberg & Lits, 1991) met the criteria for effective risk screening (column 4). In other words, the women studied in eight of twelve studies did not appear to be at high risk for LBW. 189 Y Y N Y N Y N N N Y N N Y N N N N Y N N N N N N N N N Y N N N Y Y Y N N Y N N Y N Y N Y N N N N Notes: Y = Yes, N = No, NS = Non-significant, NK = Not known 8. Did the study evaluate the relationship of process variables to LBW? Y N N N N N N N N N N N Y NK NK NK N NK NK NK NK NK NK Y N NK NK NK NK NK NK NK NK NK NK N Page 190 Klerman Moore Kitzman Norbeck Villar Graham McLaughlin Rothberg Oakley Heins Spencer Olds 6. Did the study test process variables? 7. Did the intervention change process variables? 3:40 pm 5. Did the study target risk factors modifiable by psychosocial interventions? 21/1/05 4. Was the risk screening effective in identifying women at risk for LBW? 02 Qian Lu (bc/d) 1. First author 2. Did the study describe a predictive model? 3. Did the study evaluate the effectiveness of risk screening? JOURNAL OF HEALTH PSYCHOLOGY 10(2) 190 Table 2. Evaluation of the study designs of psychosocial interventions for the prevention of LBW 02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 191 LU ET AL.: LEARNING FROM SUCCESS AND FAILURE Of the twelve trials, only four (Graham et al., 1992; Klerman et al., 2000; Norbeck et al., 1996; Rothberg & Lits, 1991) screened for psychosocial risk factors for LBW that are modifiable by psychosocial interventions; consequently only these four are able to match psychosocial interventions to psychosocial risks (column 5). Only one (Klerman et al., 2000) tested process variables (column 6). Two others (Olds et al., 1986; Villar et al., 1992) assessed process variables in their study designs, but did not include these process variables in the data analyses (column 6). Of the three studies that have information about process variables, two (Klerman et al., 2000; Olds et al., 1986) showed that the intervention was effective in changing process variables (column 7), though in neither study were these variables evaluated in terms of their relationship with outcome (LBW) (column 8). Discussion Of the 12 studies we reviewed, only one showed a significant reduction in LBW rates. However, before concluding that psychosocial interventions are ineffective in preventing LBW, it is important to evaluate the designs of these studies. Based on the work by Aiken (1999), Drotar (2002), Stevens-Simon and Orleans (1999) and West and Aiken (1997), we proposed a new model for evaluating LBW-psychosocial intervention research. None of the 12 studies met all of the criteria for effective research design. We found several pitfalls common to the design of these studies. Most interventions were not theory-driven The majority of the studies did not have a predictive model (or even a simple predictive hypothesis) that was grounded in social support theory and supported by empirical data. A predictive model specifies how the psychosocial intervention is supposed to work. Without it, it is sometimes difficult to know why, for whom and under what circumstances the program works or does not work (Drotar, 2002). Of the seven studies that did not specify a predictive model, only one (Rothberg & Lits, 1991) conducted risk screening using psychosocial risk factors and matched intervention to psychosocial risks, and none of these seven tested psychosocial mediators (process variables) of intervention effects. An effective intervention design begins with a predictive model linking intervention to outcome. The sole successful intervention trial (Norbeck et al., 1996) had a clear theoretical and empirical basis. It was hypothesized that in a population of pregnant African-American women with inadequate social support, a culturally competent social support intervention would decrease the rate of LBW. The empirical basis for the hypothesis came from an earlier study (Norbeck & Anderson, 1989), which showed that social support from the pregnant woman’s mother and male partner, but not from female friends or relatives, was directly predictive of pregnancy outcomes. Thus, inadequate support from mother and male partner was used as the basis for identifying high-risk status. In order to design an effective social support intervention, the researchers used focus groups to learn about the life situations of low-income AfricanAmerican pregnant women and the characteristics of the social support they needed during pregnancy. They found that the essential support from the woman’s mother or male partner was emotional support. Based on focus groups’ results, Norbeck et al. (1996) designed an intervention to provide emotional support. Thus, a predictive model that was grounded in social support theory and supported by empirical evidence helped guide the design of an effective intervention program. Most interventions did not have effective risk screening Risk screening is a critical first step in an intervention trial. By identifying populations at risk for LBW, interventions can be more effectively targeted to ‘high-risk’ populations. Our review suggests that most intervention trials have not had effective risk screening. Although all twelve studies conducted risk assessment, only two (Graham et al., 1992; Klerman et al., 2000) evaluated the effectiveness of risk screening, namely, whether the people who were identified at risk were in fact at risk. In one trial (Graham et al., 1992), for example, a screening questionnaire containing medical and psychosocial questions was used at the beginning of the study to differentiate between participants hypothesized to be at high or low 191 02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 192 JOURNAL OF HEALTH PSYCHOLOGY 10(2) risk of having a LBW infant. Risk factors included low family function as assessed by the Family APGAR Scale (Smilkstein, 1978), the Modified Index of Family Relationships (Hudson, 1982), stressful life events and additional risk factors such as smoking, low maternal weight–height ratio, age 27 or older and history of a previous preterm delivery. Results indicated that untreated subjects judged by the questionnaire to be at high risk by the screening instrument actually had a lower LBW rate (9%) than those judged to be at low risk (11%). Thus, the risk screening employed by this study was not effective in identifying women at risk for LBW births. In another study (Olds et al., 1986) the LBW rate was so low in the control group (2.6%) that it was nearly impossible to show any effect of the intervention even though the social support manipulation seemed effective in that study. Most studies screened for medical, socioeconomic and behavioral risk factors for LBW, many of which were not modifiable by psychosocial interventions. Only four studies (Graham et al., 1992; Klerman et al., 2000; Norbeck et al., 1996; Rothberg & Lits, 1991) screened for psychosocial risk factors; of these, only two (Norbeck et al., 1996; Rothberg & Lits, 1991) used screening instruments that were predictive of LBW. One study (Graham et al., 1992) used stressful life events as a screening instrument. Several studies have shown that stressful life events do not reliably predict LBW (Hoffman & Hatch, 1996; Lobel, Dunkel-Schetter, & Scrimshaw, 1992). In the only successful intervention trial, Norbeck et al. (1996) targeted African-American women at risk for LBW due to inadequate social support. Instead of comprehensive risk screening for medical, socioeconomic and behavioral risk factors, they used the Norbeck Social Support Questionnaire (NSSQ) to assess the adequacy of social support. If the social support from either the women’s mother or husband/partner was inadequate, women were identified as high risk and they were asked to participate in the study. A sample of African-American women who were low in social support was identified. In this study, the control group had a LBW rate of 22.4 percent, indicating that screening women at risk for LBW was effectively achieved. The intervention group had a LBW rate of 9.1 percent, 192 suggesting that the social support intervention for pregnant women with inadequate social support can be effective in preventing LBW. Most interventions have not matched interventions to risks Women with medical risk factors for LBW require medical interventions; those with psychosocial risk factors require psychosocial interventions. Many women with known medical risk factors have adequate social support and do not need psychosocial interventions. In eight out of twelve studies, participants were selected based on medical, socioeconomic and behavioral risk factors, but not psychological risk factors. Perhaps it is not surprising that offering social support to these women was not effective in reducing LBW rates. In fact, social support may not always be welcomed by participants. Developments in social support theory clearly distinguish two constructs of social support: received or provided social support (also called enacted social support), and perceived social support (whether enacted or not) (Herbert & DunkelSchetter, 1992; Lakey & Lutz, 1996). Just because the social support is received does not mean it is accepted. In one study (Spencer et al., 1989), over half the women randomly assigned to a family social worker group refused to participate in the study. It is also increasingly recognized that social support is not always helpful (Herbert & Dunkel-Schetter, 1992). Providing social support inappropriately can have an intrusive effect (Karfmacher, Kitzman, & Olds, 1998), or negative effects of other kinds (Dunkel-Schetter, Blasband, Feinstein, & Herbert, 1992). For example, one study found that reliance on peer networks for social support was associated with higher distress (Reibstein, 1981). In another study involving family members in home visits and helping them become more bonded to the pregnancy (Graham et al., 1992), few family members actually participated in the study. These problems have led researchers to rethink for whom, for what and how should social support be provided. In the only effective intervention trial, Norbeck et al. (1996) designed an intervention to provide emotional support based on focus group results. The intervention consisted of four standardized face-to-face individual sessions 02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 193 LU ET AL.: LEARNING FROM SUCCESS AND FAILURE that followed written protocols. The pregnant women were instructed to focus on three problem areas and three successful areas in their lives. Participants were guided to find meaning in their pregnancy, to increase self-esteem and improve relationships. This type of emotional support was found to be effective in reducing LBW rates among African-American women at risk for low emotional support. The trial was successful in part because the intervention matched the risks. Most interventions did not test process variables Among the 12 studies reviewed here, only one tested process variables (Klerman et al., 2000). Two other studies included measurement of process variables in the study design, but did not include them in the analyses (Olds et al., 1986; Villar et al., 1992). Without testing process variables, it is difficult to determine which components of the intervention worked and which failed (Stevens-Simon & Orleans, 1999). The only pitfall in the design of the one successful intervention study (Norbeck et al., 1996) was that process variables were not measured. Thus it is not known whether the reduction in LBW rate resulted from increased emotional support as the predictive model hypothesized, or other unmeasured processes. Furthermore, as Stevens-Simon and Orleans (1999) observed, when programs fail, it is often unclear whether the failure is because a flawed theory was implemented or because a good theory was poorly implemented. The only intervention that tested process variables (Klerman et al., 2000) failed to decrease LBW. However, because the study tested process variables, it still provided valuable information about why the intervention failed. In this study, 629 women were randomized to receive usual or augmented prenatal care. Augmented care included educationally oriented peer groups, additional appointments, extended time with clinicians and other supports. Participants in the augmented care group showed more positive perceptions of their prenatal care and greater knowledge about their risk factors. However, there was no difference in LBW rates between the two groups. Thus, the results did not support the theory that perceived helpfulness or increased knowledge (at least as manipulated) decreased the rate of LBW. Future psychosocial interventions should include measurement of process variables in the study design. Conclusion Our review suggests that it may be premature to conclude that psychosocial interventions are ineffective in preventing LBW. Most intervention trials are flawed in their study design. Thus before we can answer whether these interventions worked or not, we need to address how to conduct high quality intervention studies. Future intervention research should aim to: (1) construct a predictive model a priori to guide the intervention design; (2) develop an effective risk screening based on modifiable psychosocial risk factors, and tailor the psychosocial intervention to reduce these risk factors; and (3) test process as well as outcome variables. References Aiken, L. S. (1999). Understanding how intervention works: Combining research design and mediational analysis. Presidential Address to Division 5, Evaluation, Measurement, and Statistics, of the American Psychological Association, Boston, MA. Aiken, L. S., West, S. G., Woodward, C. K., Reno, R. R., & Reynolds, K. D. (1994). Increasing screening mammography in asymptomatic women: Evaluation of a second-generation, theory-based program. Health Psychology, 13(6), 526–538. Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. Drotar, D. (2002). Enhancing reviews of psychological treatments with pediatric populations: Thoughts on next steps. Journal of Pediatric Psychology, 27(2), 167–176. Dunkel-Schetter, C., Blasband, D., Feinstein, L. G., & Herbert, T. B. (1992). Elements of supportive interactions: When are attempts to help effective? In S. Spacapan & S. Oskamp (Eds.), Helping and being helped in the real world (pp. 83–114). Newbury Park, CA: Sage Publications. Fisher, J. D., Fisher, W. A., Misovich, S. J., Kimble. D. L., & Malloy, T. E. (1996). Changing AIDS risk behavior: Effects of an intervention emphasizing AIDS risk reduction information, motivation, and behavioral skills in a college student population. Health Psychology, 15(2), 114–123. 193 02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 194 JOURNAL OF HEALTH PSYCHOLOGY 10(2) Graham, A. V., Frank, S. H., Zyzanski, S. J., Kitson, G. C., & Reeb, K. G. (1992). A clinical trial to reduce the rate of low birth weight in an inner-city black population. Family Medicine, 24(6), 439–446. Heins, H. C., Webster, N. N., McCarthy, B. J., & Melvin, C. E. (1990). A randomized trial of nursemidwifery prenatal care to reduce low birth weight. Obstetrics and Gynecology, 75, 341–345. Herbert, T. L., & Dunkel-Schetter, C. (1992). Negative social reactions to victims: An overview of responses and their determinants. In L. Montada, S. H. Filipp, & M. J. Lerner (Eds.), Life crises and experiences of loss in adulthood (pp. 497–518). Hillsdale, NJ: Lawrence Erlbaum. Hodnett, E. S., & Fredericks, S. (2003). Support during pregnancy for women at increased risk of low birthweight babies. Cochrane Database Syst. Rev., No. 3, CD000198. Hoffman, S., & Hatch, M. C. (1996). Stress, social support and pregnancy outcome: A reassessment based on recent research. Pediatric Perinatal Epidemiology, 10, 380–405. Hudson, W. (1982). The clinical measurement package: A field manual. Homewood, IL: Dorsey Press. Karfmacher, J., Kitzman, H., & Olds, D. (1998). Intervention process as predictors of outcomes in a preventive home-visitation program. Journal of Community Psychology, 26, 49–64. Kitzman, H., Olds, D. L., Henderson, C. R., Jr, Hanks, C., Cole, R., Tatelbaum, R., McConnochie, K. M., Sidora, K., Luckey, D. W., Shaver, D., Engelhardt, K., James, D., & Barnard, K. (1997). Effect of prenatal and infancy home visitation by nurses on pregnancy outcomes, childhood injuries, and repeat childbearing: A randomized controlled trial. Journal of American Medical Association, 278, 644–652. Klerman, L. V., Ramey, S. L., Goldenberg, R. L., Marbury, S., Hou, J., & Cliver, S. P. (2000). A randomized trial of augmented prenatal care for multiple-risk, Medicaid-eligible African American women. American Journal of Public Health, 91, 105–111. Lakey, B., & Lutz, C. J. (1996). Social support and preventive and therapeutic interventions. In G. R. Pierce, B. R. Sarason, & I. G. Sarason (Eds.), Handbook of social support and the family (pp. 435–465). Plenum series on stress and coping. New York: Plenum Press. Lobel, M., Dunkel-Schetter, C., & Scrimshaw, S. C. (1992). Prenatal maternal stress and prematurity: A prospective study of socioeconomically disadvantaged women. Health Psychology, 11(1), 32–40. Lu, M. C., Tache, V., Alexander, G. R., Kotelchuck, M., & Halfon, N. (2003). Preventing low birth weight: Is prenatal care the answer? Journal of Maternal Fetal and Neonatal Medicine, 13(6), 362–380. 194 Mathews, T. J., Menacker, F., & MacDorman, M. F. (2003). Infant mortality statistics from the 2001 period linked birth/infant death data set. National Vital Statistics Report, 52(2), 1–28. McLaughlin, F. J., Altemeier, W. A., Christensen, M. J., Sherrod, K. B., Dietrick, M. S., & Stern, D. T. (1992). Randomized trial of comprehensive prenatal care for low-income women: Effect on infant birth weight. Pediatrics, 89(1), 128–132. Moore, M. L., Meis, P. J., Ernest, J. M., Wells, H. B., Zaccaro, D. J., & Terrell, T. (1998). A randomized trial of nurse intervention to reduce preterm and low birth weight births. Obstetrics and Gynecology, 91, 656–661. Norbeck, J. S., & Anderson, N. J. (1989). Psychosocial predictors of pregnancy outcomes in low-income black, Hispanic, and white women. Nursing Research, 38, 204. Norbeck, J. S., Dejoseph, J. F., & Smith, R. T. (1996). A randomized trial of an empirically-derived social support intervention to prevent low birth weight among African American women. Social Science and Medicine, 43, 947–954. Oakley, A., Rajan, L., & Grant, A. (1990). Social support and pregnancy outcome. British Journal of Obstetrics and Gynecology, 97, 155–162. Olds, D. L., Henderson, C. R., Tatelbaum, R., & Chamberlin, R. (1986). Improving the delivery of prenatal care and outcomes of pregnancy: A randomized trial of nurse home visitation. Pediatrics, 77, 16–28. Paarlberg, K. M., Vingerhoets, A. J., Passchier, J., Dekker, G. A., & van Geijn, H. P. (1995). Psychosocial factors and pregnancy outcome: A review with emphasis on methodological issues. Journal of Psychosomatic Research, 39(5), 563–595. Reibstein, J. (1981). Adjustment to the maternal role in mothers leaving careers: The impact of their interaction with role colleagues. Dissertation, University of Chicago. Rothberg, A. D., & Lits, B. (1991). Psychosocial support for maternal stress during pregnancy: Effect on birth weight. American Journal of Obstetrics and Gynecology, August, 403–407. Smilkstein, G. (1978). The family APGAR: A proposal for a family function test and its use by physicians. Journal of Family Practice, 6, 1231–1236. Spencer, B., Thomas, H., & Morris, J. (1989). A randomized controlled trial of the provision of a social support service during pregnancy: The South Manchester Family Worker Project. British Journal of Obstetrics and Gynecology, 96, 281–288. Stevens-Simon, C., & Orleans, M. (1999). Low-birth weight prevention programs: The enigma of failure. Birth, 26, 184–191. Villar, J., Farnot, U., Barros, F., Victora, C., Langer, 02 Qian Lu (bc/d) 21/1/05 3:40 pm Page 195 LU ET AL.: LEARNING FROM SUCCESS AND FAILURE A., & Belizan, J. (1992). A randomized trial of psychosocial support during high-risk pregnancies. New England Journal of Medicine, 327, 1266–1271. West, S. G., & Aiken, L. S. (1997). Toward understanding individual effects in multicoponent prevention programs: Design and analysis strategies. In K. J. Bryant, M. Windle, & S. G. West (Eds.), The science of prevention: Methodological advances from alcohol and substance abuse research (pp. 167–209). Washington, DC: American Psychological Association. 195