Pain 118 (2005) 185–193
www.elsevier.com/locate/pain
Heart rate mediation of sex differences in pain tolerance in children
Qian Lua, Lonnie K. Zeltzera, Jennie C.I. Tsaoa, Su C. Kima, Norman Turka, Bruce D. Naliboffb,*
a
Pediatric Pain Program, Department of Pediatrics, David Geffen School of Medicine at UCLA, and Veterans Administration Greater Los Angeles Healthcare
System, Bldg. 115, Rm. 223 11301 Wilshire Boulevard, Los Angeles, CA 90073, USA
b
UCLA Center for Neurovisceral Sciences and Women’s Health, Department of Psychiatry and Biobehavioral Sciences, David Geffen School of Medicine at
UCLA, and Veterans Administration Greater Los Angeles Healthcare System, Bldg. 115, Rm. 223 11301 Wilshire Boulevard, Los Angeles, CA 90073, USA
Received 19 February 2005; received in revised form 16 June 2005; accepted 8 August 2005
Abstract
Despite evidence supporting the existence of important sex-related differences in pain, the mechanisms underpinning such differences are
not well understood. The aim of this study is to examine the relationship between sex and pubertal differences in autonomic arousal and pain
tolerance to laboratory pain stimuli in healthy children. We tested the following specific hypotheses: (1) females would have greater autonomic
arousal and less pain tolerance than males, and (2) this sex difference in pain tolerance would be mediated by autonomic arousal. Participants
were 244 healthy children (50.8% female, mean age 12.73G2.98 years, range 8–18 years). Separate 4-trial blocks of cutaneous pressure and
thermal pain stimuli were presented in counterbalanced order. Heart rate (HR) was recorded during 2–3 min periods preceding each block and a
1-min period between trials. Results indicated lower tolerance in females for cutaneous pressure, but not thermal pain, compared to males. In
addition, pre-trial HR was greater for females than males. Mediation analyses suggested that sex differences in pressure pain tolerance were
accounted for by sex differences in pre-trial HR. There were also significant effects for puberty, but these did not vary by sex. Overall, early
pubertal children had greater pre-trial HR and less pain tolerance than those in late puberty for both cutaneous pressure and thermal pain across
sex. These results suggest that autonomic arousal may be a mediator of sex-related differences in pain responses in children.
q 2005 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
Keywords: Sex differences; Laboratory pain; Pain tolerance; Heart rate; Puberty; Children and adolescents
1. Introduction
Considerable research indicates that females are more
likely than males to experience clinical pains (Unruh, 1996);
females also demonstrate enhanced responses to experimental pain (Riley et al., 1998). A potential mediator of sex
differences in pain responses is level of anxiety or arousal.
Affective processes, generally, and autonomic arousal,
specifically, have important links to pain perception and
modulation (Price, 2002). It is recognized that the major
ascending and descending pain networks in the brain include
limbic system structures such as the amygdala, anterior
cingulate cortex, and hypothalamus. Cortico-limbic interactions are thought to have a significant role in determining
the focus and threshold for nociceptive information (Craig,
* Corresponding author. Tel.: C1 310 268 3242; fax: C1 310 794 2864.
E-mail address: naliboff@ucla.edu (B.D. Naliboff).
2003). Consistent with this neurophysiological model is the
observation that affective processes, particularly anxiety, are
associated with clinical pain symptoms (Schmidt et al., 2002)
and experimental pain responses (Tsao et al., 2004).
Autonomic nervous system (ANS) arousal, indexed by
increased heart rate (HR), has been hypothesized to be
associated with increased pain sensitivity (Jassen, 2002).
Support for arousal in setting the overall tone of the pain
perception system include findings that ANS arousal, i.e.
resting HR before painful stimulation, influences perceived
pain intensity and behavioral response (Dowling, 1983).
Porro et al. (2003) reported that HR during anticipation of
pain is associated with increased activity in somatosensory
cortex, thalamus, and anterior cingulate cortex, and
decreased activity in medial prefrontal cortex. Thus, ANS
arousal during pain anticipation may activate regions
involved in ‘priming’ pain sensitivity and may indicate
processes related to group and individual differences in pain
response. A meta-analysis (Stoney et al., 1987) and a review
0304-3959/$20.00 q 2005 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
doi:10.1016/j.pain.2005.08.008
186
Q. Lu et al. / Pain 118 (2005) 185–193
(Piira et al., 2002) suggested that females exhibit enhanced
cardiac responsivity (i.e. HR) to laboratory stressors, which
may be related to greater anticipatory anxiety. Thus, sexbased differences in arousal in anticipation of painful
stimulation may be an important mediator of laboratory
pain responses.
Despite evidence of sex-related differences in basal HR
in adults, few studies have examined such differences in
children. Two studies (Allen and Matthews, 1997; Steiner
et al., 2002) suggested that adolescent girls (aged 14–18
years) have higher HR than boys in anticipation of stressinducing tasks. Stage of pubertal development has received
scant attention despite the hypothesis that pubertal status
may be an important marker for the emergence of female
predominance in clinical pain syndromes (LeResche, 1999).
There is little direct data examining the interacting
influences of sex and puberty in moderating ANS activity
in anticipation of or during stress tasks.
The current study tested the relationship between
autonomic arousal (indexed by HR during pre-trial periods)
and children’s pain tolerance to two different laboratory
pain tasks, taking into account child sex, age, and pubertal
status, as well as the sex by puberty interaction. These
specific hypotheses were tested: (1) females will have
greater pre-trial HR and lower pain tolerance than males; (2)
this sex difference in pain tolerance will be mediated by pretrial HR; and (3) late pubertal children will have lower pretrial HR and higher tolerance compared with children in
early puberty.
2. Methods
2.1. Participants
A sample size of 240 children was chosen to give adequate
power (O0.85) to test for moderate effect size differences (dZ0.4)
for comparisons across puberty, sex, and the puberty by sex
interaction, with the assumption of no interactions with task type.
In total, 244 healthy children (124 female; 50.8%) with a mean age
of 12.73 years (SD, 2.98 years, range, 8–18 years) served as
participants. The ages of male (mean, 12.44 years, SD, 2.89 years)
and female (mean, 13.01 years, SD, 3.05 years) participants were
closely matched. The current sample included 109 children in the
early stages of puberty (54 female, 55 male) and 125 in the late
stages of puberty (63 female, 62 male). Mean age of the early
pubertal sample was 10.5 years and mean age of the sample in late
puberty was 14.6 years. Mean grade in school of early pubertal
cohort was 5th grade, and for the late pubertal group was 9th grade.
The ethnic composition of the sample was 40.2% Caucasian,
13.9% African–American, 9.8% Asian–American, 23.8% Hispanic, and 12.3% other. Parent socioeconomic status (Hollingshead,
1975) was: unskilled workers 3.7%, semi-skilled workers 4.1%,
clerical/sales 11.9%, technical 41.8%, professional 34.8%.
Participants were recruited from a major urban area through
mass mailing, posted advertisements, and classroom presentations.
The mailings and advertisements were widely targeted across sites
with varying ethnicities and income levels since one of the goals of
subject recruitment was to enhance the enrollment of children from
low-income and minority neighborhoods. Initial eligibility was
confirmed by telephone: 489 individuals were screened for
eligibility by telephone; 17 children (3.5% of those screened)
were excluded due to on-going acute or chronic illness, or use of
medications that would affect study outcomes. Of the 472 (96.5%)
invited to participate, 228 (48%) declined participation mainly
because of parental lack of interest (54%) or time (21%). Of the 244
study participants, four did not complete the protocol in its entirety
because one felt uncomfortable being attached to the physiological
sensors, while the others refused to do the lab pain tasks due to lack
of time or interest. The University of California, Los Angeles
(UCLA) Institutional Review Board (IRB), as well as the IRBs for
recruitment sites approved all recruitment and study procedures.
IRB approved consent and assent forms were completed by parents
and children, respectively. Participants received a $30 video store
gift certificate and a t-shirt for their participation.
2.2. Overview of procedure
Laboratory sessions were conducted between 8 a.m. and 8 p.m.
by two experimenters. At the start of the session, participants
completed demographic and psychosocial questionnaires, administered by an experimenter in a quiet room adjacent to the laboratory.
The experimenters included five females and two males. Two
experimenters together conducted the laboratory sessions. Of the
244 sessions, 198 were run with two females, 39 with a male and
female experimenter, 1 with two males, and 7 that did not have the
sex of the experimenter recorded. Post-hoc analyses did not reveal a
participant–experimenter interaction in tolerance times when
comparing female–female experimenter pairs with female–male
experimenter pairs after controlling for child age.
After completing questionnaires, participants were escorted
individually to the laboratory where they were seated in a chair and
electrocardiogram (ECG) leads were attached for continuous
cardiovascular measures. After ECG placement, there was a 15min laboratory habituation period. Thus, the time from lead
placement to the first baseline epoch used in the analysis was at
least 15 min. Participants were then instructed about and exposed
to the thermal and pressure pain laboratory pain tasks (see below
for detailed descriptions).
The purpose of the larger study from which the current data
were drawn was to examine the effects of sex, puberty,
psychological vulnerability, and their interactions on pain
responsivity. The larger study examined multiple tasks, including
cutaneous heat and pressure, and a cold pressor task. The pressure
and heat pain tasks each included four trials; within each task, all
four trials had identical ceilings (see below for detailed
description). The cold pressor task consisted of 2 trials: one trial
with a 1 min informed ceiling and one trial with a 3 min
uninformed ceiling. Since the current analysis was focused on
the relationship between HR and tolerance across multiple trials,
we only included in this analysis the pressure and heat tasks, each
with a similar four trial design. Results for the cold pressor have
been presented elsewhere (Tsao et al., 2004).
Four-trial blocks of cutaneous pressure and thermal pain stimuli
were presented separately in counterbalanced order across
participants. A 2- to 3-min resting baseline period preceded the
first trial of each block and a 1-min resting period preceded each of
the other three trials. For each task we used two sites to avoid local
Q. Lu et al. / Pain 118 (2005) 185–193
sensitization or habituation, and we used two intensities to allow
for greater variation in pain response.
Following the pain tasks, self-report puberty staging diagrams
(pictures of Tanner pubertal stages, described below) were
administered. The current study examined factors associated with
pain tolerance rather than intensity in order to focus on more
objective and behavioral measures. Results related to sex effects on
ratings of pain intensity have been published elsewhere (Tsao
et al., 2004).
2.3. Laboratory pain tasks
2.3.1. Pressure task
The Ugo Basile Analgesy-Meter 37215 was used to administer
focal pressure through a Lucite point approximately 1.5 mm in
diameter to the second dorsal phalanx of the middle finger and
index finger of each hand. Four trials, two at each of two levels of
pressure (322.5 and 465 g), were run with an uninformed ceiling of
3 min. Between each trial there was a 1-min rest interval. A
comparable device has been used in healthy and clinical pediatric
samples (aged 5–17 years) without adverse effects (Gil et al., 1997;
Walco et al., 1990).
2.3.2. Thermal task
The Ugo Basile 7360 Unit was used to administer a total of four
trials of two infrared intensities (15, 20) of radiant heat 2 in.
proximal to the wrist and 3 in. distal to the elbow on both volar
forearms with an uninformed ceiling of 20 s. Thermal pain
tolerance was electronically measured with an accuracy of 0.1 s.
A similar task has been used in a sample aged 6–17 years without
adverse effects (Meier et al., 2001).
For both tasks, there was a 1-min rest interval between each
trial. The presentation order (setting, site of exposure) was
counterbalanced across participants. Before the start of each trial,
subjects were informed that they would experience moderate
sensation that might eventually be perceived as pain. Participants
were instructed to continue with the task for as long as they could
and to withdraw from the apparatus if it became too uncomfortable
or painful. All tasks were extensively piloted on volunteers in the
targeted age range to ensure safety and acceptability and to
determine the lowest level of stimulation that would allow
sufficient variation in responding.
2.4. Laboratory pain measures
2.4.1. Pain tolerance
Pain tolerance was defined as time in seconds elapsed from the
onset of the pain stimulus to participants’ withdrawal from the
stimulus.
2.4.2. Anticipatory anxiety
Ratings of anticipatory anxiety were obtained immediately prior
to each trial. Participants used a vertical sliding VAS, anchored with
0 at the bottom indicating the least amount and 10 at the top
indicating the greatest amount, in response to the instruction to rate
‘how nervous, afraid, or worried’ they were about the upcoming
task. The scale also had color cues, graded from white at the bottom
to dark red at the top, as well as a neutral face at the bottom and a face
showing a negative expression at the top.
187
2.5. Heart rate recording and analysis
ECG was recorded from electrodes attached to the jugular notch
and over lower ribs using an isolated bioamplifier (BMA-931, And
ISO-Z; CWE, Inc, Ardmore, PA). The signal was sampled at 400
Hz using Windaq software (Dataq, Akron, OH). The ECG signals
were bandpass filtered (10–80 Hz) and processed through adjusting
peak detection algorithm time R-waves using specially written
software (RedTech, Calabasas, CA). All epochs were also visually
checked for quality control. Periods with excessive noise, usually
due to movement, were eliminated from the analysis. HR was
recorded for the 2-min period preceding the first trial of each pain
task and for the 1-min periods preceding the other three trials of
each task. Individual interbeat intervals were averaged to derive
means for each period. Therefore, the HR measure in this analysis
is not an immediate pre-task value (e.g. single beat) but a more
stable baseline level of arousal before the task.
2.6. Pubertal status
Pubertal stage was assessed with a self-report instrument (Morris
and Udry, 1980) consisting of schematic drawings, including
appropriate written descriptions of five stages of secondary sexual
characteristics on two separate dimensions (female breasts and
pubic hair, and male genitalia and pubic hair) based on Tanner’s
Sexual Maturity Scale (Tanner, 1962; 1975). Such self-assessment
ratings of pubertal status by children and adolescents correlate well
with ratings based on physical examination by physicians (Dorn et
al., 1990; Dukes et al., 1980; Frankowski et al., 1987; Morris and
Udry, 1980; Schlossberger et al., 1992). Each participant was given
sex-appropriate schematic drawings and asked to rate her or himself
on each of the two dimensions by selecting the drawing closest to his
or her stage of development. A single individual score, ranging from
I—pre-pubertal to V—adult level of development, was computed
by averaging the two ratings (Angold et al., 1998; 1999). In this
report, we use a dichotomized variable to indicate pubertal status.
Since Tanner scores range from 1 to 5, with 1, pre-puberty and 5,
adult sexual development, we used Tanner R3 to represent ‘late
puberty’ and lower scores to indicate early puberty.
2.7. Data analysis
Mixed models (SPSS for Windows, 2003), known variously as
multilevel modeling (Singer and Willett, 2003) or Hierarchical
Linear Modeling (Bryk and Raudenbush, 1992), was used to study
the influence of sex and puberty on pain tolerance and HR across
the four trials of the heat and pressure pain tasks. The mixed
models are generally more flexible in terms of its data requirements
because the repeated observations are viewed as nested within the
person rather than as the same fixed set for all persons as in
standard ANOVA models. Therefore, mixed models can incorporate both intra-individual and inter-individual change and handle
missing data better than ANOVA or Repeated Measures in General
Linear Model. In this study, our hypotheses regarding the effects of
sex and puberty on pain tolerance and HR were analyzed by a twolevel model using Mixed Models:
Level 1: Yij Z b0i C Rij
Level 2: b0i Z g00 C g01 !Sexi C g02 !Pubertyi C g03 !Sexi
!Pubertyi C U0i
188
Q. Lu et al. / Pain 118 (2005) 185–193
Combining the two equations into one by substituting the level
2 equation into the level 1 equation, we have the equation below,
with the random effects identified by placing them in square
brackets.
Yij Z g00 C g01 !Sexi C g02 !Pubertyi C g03 !Sexi !Pubertyi
C ½U0i C Rij The term U0i is a random effect at level 2 (individuals level),
representing random variation in the average pain tolerance across
all individuals in the population. The term Rij is a random effect at
level 1 (repeated trials), representing random variation in the pain
tolerance across all trials for individuals i in the population. This
model, therefore, tested as predictors of pain tolerance for
individual i at the jth trial, the average intercept for the population,
sex of individual i, puberty status of individual i, the interaction of
sex and puberty of individual i, the unique effect of individual i (i.e.
U0j, random intercept) and random error associated with each
individual i at the jth trial (Rij).
Mixed models analysis was performed by using the mixed
models subprogram in SPSS 12.0.0 (SPSS for Windows, 2003). In
all of the models reported, test of random intercept (U0j) was
significant; suggesting individuals varied on initial level of all of
the outcomes.
Mediation analysis was used to examine the hypothesis that
pre-trial HR mediated sex differences in pain tolerance. When the
relationship between the independent and the dependent variable is
partially or totally accounted for by the hypothesized mediating
variable, this variable may be considered a mediator (Baron and
Kenny, 1986). When both the mediator and the outcome variables
are measured repeatedly over time (as in this case in which HR and
pain tolerance are measured over multiple trials), the outcome and
mediator can be viewed as concurrent parallel processes (Cheong
et al., 2001). Using mixed modeling in SPSS 12.0.0, the following
model was tested,
Pain toleranceij Z g00 C g01 !Sexi C g02 !Pubertyi C g03
!Sexi !Pubertyi C HRij C U0i C Rij
This model, therefore, tested as predictors of pain tolerance for
individual i at the jth trial, the average intercept for the population, sex
of individual i, puberty status of individual i, the interaction of sex and
puberty of individual i, pre-trial HR for individual i before the jth trial,
the unique effect of individual i (i.e. U0i, random intercept) and
random error associated with each individual i at the jth trial (Rij).
3. Results
3.1. Descriptive statistics
Table 1 provides descriptive statistics for pain tolerance
and HR during the four pre-trial periods (before pain trials)
and pre-task anxiety before the pain trials. On average, 13
(5%) participants reached ceiling during the pressure pain
trials, and 47 (19.2%) participants reached ceiling during the
heat pain trials. Even though more males than females
reached ceiling during the pressure pain trials (8 vs. 5) and
the heat pain trials (26 vs. 21), these differences were not
significant. Due to ceiling effects, transforming pressure
pain tolerance and heat pain tolerance would not have been
appropriate to normalize the distribution. Given the ceiling
effects and non-normal distribution of pressure and heat
pain tolerance, two sets of analyses were performed with
and without the cases reaching ceiling. Results did not differ
between the two sets of analyses. Therefore, the results with
the total sample were reported, since larger sample size
reduces the problem of non-normal distribution.
Table 1
Descriptive statistics of pain tolerance, HR and anxiety across four pressure and heat pain trials
Trial
1
2
3
4
Average
Pressure pain trials
Heat pain trials
Tolerance
(seconds)
Pre-trial HR
(beat/min)
Pre-trial anxiety
Tolerance
(seconds)
Pre-trial HR
(beat/min)
Pre-trial anxiety
Mean
SD
N
Mean
SD
N
Mean
SD
N
Mean
SD
N
37.26
53.04
239
50.25
57.98
239
37.07
50.57
239
36.50
51.82
239
78.45
10.61
222
75.51
10.12
177
76.60
10.10
177
77.12
10.35
177
2.96
2.56
237
3.35
2.88
234
3.14
2.76
234
3.10
2.81
234
14.34
6.08
239
8.89
5.60
240
10.64
6.54
238
9.23
5.56
239
78.44
11.11
227
75.62
10.88
183
76.54
10.21
182
76.66
10.53
182
3.91
2.83
239
3.71
2.95
238
3.88
3.18
239
3.61
3.04
239
Mean
SD
Range (min–max)
N
40.27
53.65
1–180
239
77.01
10.35
48.36–109.17
188
3.14
2.75
0–9.76
235
10.77
6.33
0–20
239
76.91
10.75
48.94–109.45
194
3.78
3.00
0–9.76
239
HR, heart rate.
Q. Lu et al. / Pain 118 (2005) 185–193
3.2. Pressure task
3.2.1. Main effects of sex and puberty on pressure
pain tolerance
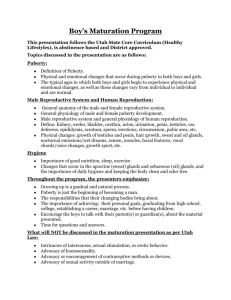
As shown in Table 2 (model 2.2) and Fig. 1, mixed model
analysis revealed that males had greater pressure tolerance
than females (F (1,229)Z4.78, PZ0.03), and late puberty
children had greater pressure tolerance than those in early
puberty (F (1,229)Z31.56, P!0.001). The results hold
after controlling for age, indicating that pubertal influences
on pressure tolerance were above and beyond age. Although
the interaction of sex and puberty was not a statistically
significant predictor of pressure tolerance (F (1,229)Z2.49,
PZ0.116), there was a trend for males to have a larger
increase in pressure tolerance from early puberty to late
puberty than females (Fig. 1). Table 2 indicates the results
of the mixed model analyses, with marginal means for males
and females, and for early and late puberty children.
3.2.2. Main effect of sex and puberty on pre-trial
HR during pressure trials
As shown in Table 2 (model 2.1) and Fig. 1, mixed model
analysis revealed that females had higher HR than did males
(F (1,214)Z8.55, PZ0.004); similarly, early pubertal
children had higher HR than those in late puberty (F
(1,214)Z21.582, P!0.001). Since age was a significant
predictor of HR (F (1,212)Z7.02, P!0.01), we statistically
controlled for age and found that puberty no longer had a
significant main effect on HR (F (1,211)Z2.34, PO0.05).
189
This finding suggests that puberty did not predict HR above
and beyond age. The interaction of sex and puberty was
not a significant predictor of HR for the pressure task
(F (1,214)Z0.018, PO0.05).
3.2.3. Pre-trial HR mediates sex influences on pressure
pain tolerance
The mediation analyses were conducted in two steps. To
meet criteria as a mediator, pre-trial HR had to be associated
with both sex and pain tolerance. As discussed above, HR
differed by sex. Mixed model analysis also indicated that
HR was negatively related to pressure tolerance (rZ-0.25,
P!0.001). This corresponds to a d-value of 0.5 or a
medium effect size (Cohen, 1988). In the second step, to test
HR as a mediator, we entered sex, puberty, their interaction,
and HR into a regression equation to predict pressure
tolerance. We predicted that sex would not be a significant
predictor once HR entered the equation. As shown in
Table 2 (model 2.3), mixed model analysis indicated that
HR still predicted pressure tolerance (F (1,363)Z10.17,
PZ0.002), and sex was no longer a significant predictor (F
(1,220)Z0.76, PZ0.384). Therefore, HR was considered to
mediate the sex difference in pressure tolerance. Anticipatory anxiety was also assessed as a possible mediator of sex
differences in pressure tolerance. Although anxiety had
negative correlations with pain tolerance (r range, K0.14 to
K0.25 for the various trials), it did not differ between boys
and girls and was not correlated with pre-trial HR, so a
formal mediation analysis was not performed.
Table 2
Mixed model analysis on pressure tolerance and heart rate
Dependant variables
Independent variables
Marginal mean (SE)
Model 2.1
Sex
Heart rate
Puberty
Male, 75.76 (0.95)
Female, 79.76 (0.98)
Early, 80.93 (0.99)
Late, 74.59 (0.94)
Early puberty male, 78.84 (1.38)
Late puberty male, 72.68 (1.32)
Early puberty female, 83.02 (1.41)
Late puberty female, 76.49 (1.35)
Male, 45.26 (3.97)
Female, 32.98 (3.96)
Early, 23.36 (4.09)
Late, 54.88 (3.84)
Early puberty male, 25.08 (5.76)
Late puberty male, 65.44 (5.47)
Early puberty female, 21.65 (5.81)
Late puberty female, 44.32 (5.38)
Male, 42.03 (4.15)a
Female, 36.81 (4.27)a
Early, 24.37 (4.41)a
Late, 54.46 (4.09)a
Early puberty male, 21.83 (6.02)a
Late puberty male, 60.98 (5.82)a
Early puberty female, 25.67 (6.30)a
Late puberty female, 46.69 (5.78)a
Sex!Puberty
Model 2.2
Sex
Pressure tolerance
Puberty
Sex!Puberty
Model 2.3
Sex
Pressure tolerance
Puberty
Sex!Puberty
Heart rate
a
Marginal mean when heart rate at 77 beat/min.
F
DF
P
8.55
1,214
0.004
21.58
1,214
!0.001
0.02
1,214
0.895
4.79
1,229
0.03
31.56
1,229
!0.001
2.49
1,229
0.12
0.76
1,220
0.38
24.21
1,222
!0.001
2.35
1,219
0.13
10.17
1,363
0.002
190
Q. Lu et al. / Pain 118 (2005) 185–193
Pressure Tolerance by Gender and Puberty
B 16
Male
Female
Heat Tolerance (seconds)
Pressure Tolerance (seconds)
A 80
Heat Tolerance by Gender and Puberty
60
40
20
14
Male
Female
12
10
8
6
4
2
0
0
Early
Late
Early
Puberty
Pre-Trial Heart Rate During Heat Task
Pre-Trial Heart Rate During Pressure Task
C 85
Male
Female
D 85
75
70
65
60
55
Male
Female
80
Heart Rate (beat/min)
Heart Rate (beat/min)
80
Late
Puberty
75
70
65
60
55
50
50
Early
Late
Early
Puberty
Late
Puberty
Fig. 1. Sex and pubertal differences in pressure tolerance, heat tolerance, and heart rate (values are meanGSE).
3.3. Thermal pain task
3.3.1. Main effects of sex and puberty on thermal pain
tolerance
As shown in Table 3 (model 3.2) and Fig. 1, mixed model
analysis revealed that late pubertal children had greater
thermal tolerance than did those in early puberty (F
(1,230)Z55.88, P!0.001). However, unlike the findings
for the pressure task, the thermal task analysis did not reveal
a sex difference in tolerance (F (1,230)Z1.58, PZ0.21).
Additionally, the interaction of sex and puberty was
not significantly predictive of thermal pain tolerance
(F (1,230)Z2.49, PZ0.61). After controlling for age (age
was a significant predictor, F (1231)Z38.43, P!0.001),
puberty was no longer found to have a significant main
effect on tolerance (F (1,228)Z1.73, PO0.05).
3.3.2. Main effects of sex and puberty on pre-trial
HR during thermal pain tasks
As shown in Table 3 (model 3.1) and Fig. 1, mixed model
analysis revealed that females had higher pre-trial HR than
did males (F (1,219)Z8.43, PZ0.04), and early pubertal
children had higher pre-trial HR than did late puberty
children (F (1,219)Z21.66, P!0.001). After controlling
for age (age was a significant predictor, F (1, 218)Z13.10,
P!0.001), puberty no longer remained significant (F
(1,218)Z0.711, PO0.05). The interaction of sex and
puberty was also found not to be a significant predictor of
HR during thermal pain tasks (F (1,219)Z0.015, PO0.05).
Since no sex differences were found for heat tolerance,
mediation analysis was not conducted.
4. Discussion
We hypothesized sex differences in pain tolerance and
autonomic arousal in anticipation of pain, and that autonomic
arousal, as indexed by HR, would mediate sex differences in
pain tolerance. Our results confirm sex differences in pain
tolerance but only for cutaneous pressure and not for thermal
pain. We also found higher HR for females compared to
males during pre-trial periods. Notably, mediation analysis
Q. Lu et al. / Pain 118 (2005) 185–193
191
Table 3
Mixed model analysis on heat tolerance and heart rate
Dependant variables
Independent variables
Marginal mean (SE)
Model 3.1
Sex
Heart rate
Puberty
Male, 75.72 (0.98)
Female, 79.76 (0.99)
Early, 80.99 (1.01)
Late, 74.50 (0.96)
Early puberty male, 78.88 (1.42)
Late puberty male, 72.56 (1.32)
Early puberty female, 83.09 (1.45)
Late puberty female, 76.44 (1.37)
Male, 11.08 (0.43)
Female, 10.32 (0.43)
Early, 8.43 (0.44)
Late, 12.97 (0.41)
Early puberty male, 8.96(0.62)
Late puberty male, 13.19 (0.59)
Early puberty female, 7.90 (0.63)
Late puberty female, 12.74 (0.58)
Male, 11.64 (.45)a
Female, 10.98 (0.46)
Early, 9.35 (0.48)
Late, 13.27(.43)
Early puberty male, 10.00 (0.66)a
Late puberty male, 13.29 (0.62)a
Early puberty female, 8.71 (0.68)a
Late puberty female, 13.24 (0.61)a
Sex!Puberty
Model 3.2
Sex
Heat tolerance
Puberty
Sex!Puberty
Model 3.3
Sex
Heat tolerance
Puberty
Sex!Puberty
Heart rate
a
F
DF
P
8.43
1,219
0.004
21.66
1,219
!0.001
0.015
1,219
0.903
1.58
1,230
0.21
55.88
1,230
!0.001
0.26
1,230
0.61
1.07
1,203
0.30
35.51
1,204
!0.001
0.95
1,202
0.33
5.46
1,300
0.02
Marginal mean when heart rate at 77 beat/min.
suggested that sex differences in pressure tolerance were
mediated by differences in HR. Pubertal status had
significant effects on HR and pain tolerance but these effects
did not interact with sex. Overall, early pubertal children had
higher HR and lower pain tolerance than late pubertal
children. Despite the difficulty in separating puberty and age
effects given their high correlation (rZ0.7), results indicated
that the relationship between puberty and HR could be
accounted for by age, whereas, differences in pressure
tolerance may be puberty-specific.
4.1. Sex, puberty and task differences in pain responses
Increased pain sensitivity for females compared to males
has been reported for some experimental pain models but
not all (Fillingim and Maixner, 1995). A meta-analysis
(Riley et al., 1998) revealed that effect sizes ranged from
moderate to large depending on the stimulus. Values for
pressure and electrical stimulation were the largest. Thermal
pain effects were smaller (mean effect size, 0.41) and more
variable (effect size SD, 0.47) than for pressure pain. Our
data are consistent with this overall pattern in that we found
decreased tolerance in females compared to males for the
pressure and not for the heat task. Because the heat task was
much shorter in duration than the pressure task (0–180 vs.
1–20 s), the restricted range of values for the heat task might
have led to an attenuation of sex-dependent effects.
Developmental differences in pain tolerance also
appeared to be partially task-dependent. Overall, pain
tolerance increased as age increased—findings that may
relate to developmental differences in children’s cognitive
abilities and sense of time. Older children may be better
able than younger children to understand that experimental
pain is temporary, and thus, less threatening. Older
children may also have a wider array of coping responses
to assist them in tolerating the tasks longer than younger
children (Piira et al., 2002). As noted above, pubertal
status and age were closely correlated; however, there was
also significant variance in pubertal status within age
bands, especially during early adolescence. After controlling for age, a pubertal effect on pain tolerance was found
for the pressure, but not the thermal task. Beyond age
alone, puberty denotes physiological changes in gonadal
hormones, such as testosterone, estrogen, and progesterone, as well as changes in cognitive abilities. Thus, the
longer duration pressure task may elicit more developmental physiological and cognitive differences beyond
those associated with age alone.
Although not statistically significant, late pubertal males
appeared to have greater pressure tolerance than late
pubertal females (65G5.47 vs. 44G5.38 s), but early
pubertal males and females were similar (see Fig. 1). With
advancing puberty in males, there are increasing levels of
testosterone and muscle bulk, which may influence
tolerance during longer exposures. Social and cognitive
factors may also play a greater role during longer tasks.
Prior work has shown a similar sex by puberty interaction
with increased tolerance to cold pressor in older boys
192
Q. Lu et al. / Pain 118 (2005) 185–193
compared to older girls. The authors hypothesized that this
was due to a more ‘tough’ or stoical view of self in older
boys (Piira et al., 2002).
In the current study, younger children (10.5G1.6 years)
had higher HR in anticipation of pain than older children
(14.5G2.4 years) across sex, and there were no specific
effects of puberty on HR beyond age. The results are
consistent with previous studies showing that younger
children have a higher level of resting HR than older
children (Alkon et al., 2002; Matthews et al., 2002). Given
that pubertal effects on tolerance remained significant after
controlling for HR, the data also support somewhat
independent mechanisms for the influences of sex and
development on pain tolerance. Sex effects may depend
partially on autonomic arousal as suggested by the
mediation analysis, while age/puberty related differences
may result from other cognitive or physiological factors.
4.2. Role of ANS in pain responses
It is increasingly recognized that central pain processing
is highly influenced by, if not an integral part of, limbic
circuitry (Craig, 2003; Price, 2002). Craig (2003) has
presented a model in which pain can be seen as a component
of interoception or homeostatic regulation, and pain
modulation would be highly interconnected with autonomic
function. A related model points to the key role of a set of
interconnected brain circuits referred to collectively as the
Emotional Motor System (EMS). The term EMS refers to a
specific set of parallel motor pathways governing somatic,
autonomic, antinociceptive and endocrine responses
(Holstege et al., 1996) when an organism’s homeostasis is
threatened, or perceived to be threatened. The EMS includes
subcortical structures such as the hypothalamus, amygdala
and periaqueductal gray. These receive peripheral input
from visceral and somatic afferents and cortical input from
subregions of cingulate and prefrontal cortices, and anterior
insula. The EMS in turn modulates activity in medullary
pontine nuclei (e.g. rostral ventral medulla, locus coeruleus,
raphe nuclei) involved in physiological and behavioral
responses. The output of this network reaches nuclei within
the brainstem with important roles in the regulation of pain
modulation, arousal and vigilance. Another very similar
model is that of the central autonomic networks proposed by
Thayer and Siegle (2002). These models predict that
differences in autonomic activity as indexed by peripheral
measures like HR are reflective of the overall state of the
EMS and that increased EMS activity may be associated
with altered attention (hypervigilance), inadequate pain
modulation, and decreased tolerance.
Only a small number of studies have actually compared
autonomic measures directly with pain responses. Chapman
et al. (2002) using an electrical stimulus found that
autonomic measures (primarily sympathetic measures like
skin conductance) could account for 44% of the variance in
pain report, and Dowling (1983) reported that pre-task HR
predicted cold pressor tolerance. Relevant to the current
findings, there is also recent evidence that men and women
(at least those with chronic visceral pain) show differential
central processing of a noxious visceral stimulus (Naliboff
et al., 2003). In this study using PET imaging, women
showed greater activation of limbic-related areas including
anterior cingulate cortex and amygdala, while men showed
greater activation in cognitive areas (lateral frontal cortex)
and central autonomic/pain modulation areas (insula and
brain stem in the region of periaqueductal gray). Chapman
(2002) in a study of electrical stimuli found that men who
experienced higher levels of arousal (based on skin
conductance, HR, and pupil diameter) gave more accurate
pain reports than those who had lower levels, but women
who had higher levels of arousal gave less accurate pain
reports than those with lower levels. Thus, there is some
evidence that ANS arousal is associated with altered pain
responses and that sex differences in pain may be in part
related to ANS differences. The current findings are
consistent with this general hypothesis and suggest for the
first time that sex-related differences in ANS responses in
anticipation of pain can account for sex-related differences
in pain tolerance.
4.3. Limitations
First, our mediation analyses should be interpreted with
caution until replicated. Since HR was not manipulated in
this study it is not possible to make definitive conclusions
regarding causation, however, the use of multiple trials and
the fact that pre-trial HR always preceded pain tolerance
support the conclusion of HR mediation of sex difference in
pain tolerance. The interpretation of HR as a marker of
general arousal is consistent with previous literature
although other possible moderators of HR (e.g. physical
conditioning) cannot be completely ruled out. Second, this
study focused on only one autonomic arousal marker, HR.
HR is a sensitive, but non-specific, measure determined by
many factors. It has both sympathetic and parasympathetic
influences, and therefore, future studies with more specific
indicators such as pre-ejection period, skin conductance, or
measures of HR variability are warranted. Third, we
assessed only pain tolerance, a measure of pain behavior,
rather than measures of pain magnitude. The influence of
psychosocial factors on pain tolerance might be larger than
that on pain magnitude judgments such as pain threshold.
Fourth, although this study was not designed to specifically
examine the interaction of experimenter and subject sex on
tolerance, it is plausible that this may have had some effect.
Our post-hoc analyses, however, did not reveal evidence of
such an interaction on tolerance.
4.4. Summary and conclusion
The present results show clear but generally independent
effects of age and sex on experimental pain tolerance in
Q. Lu et al. / Pain 118 (2005) 185–193
a large sample of healthy children. Type of pain stimulation
is important, as the sex differences were only observed
during pressure pain and not during thermal heat pain. In
addition, we have shown that the observed sex differences in
pressure tolerance were mediated by pre-trial HR,
suggesting an important role for autonomic arousal in
these responses.
Acknowledgements
This study was supported by R01 DE12754-01A1
(LKZ), the UCLA General Clinical Research Center Grant
MO1-RR-00865 (LKZ), R01 NR007768 (BDN) and R24
AT002681. The authors would like to thank Ms. Teresa
Olivas for assistance in preparing this manuscript.
References
Allen MT, Matthews KA. Hemodynamic responses to laboratory stressors
in children and adolescents: the influences of age, race, and gender.
Psychophysiology 1997;34(3):329–39.
Angold A, Costello EJ, Worthman CM. Puberty and depression: the roles of
age, pubertal status and pubertal timing. Psychol Med 1998;28:51–61.
Angold A, Costello EJ, Worthman CM. Pubertal changes in hormone levels
and depression in girls. Psychol Med 1999;29:1043–53.
Baron RM, Kenny DA. The moderator–mediator variable distinction in
social psychological research: conceptual, strategic, and statistical
considerations. J Pers Soc Psychol 1986;51:1173–82.
Bryk AS, Raudenbush SW. Hierarchical linear models. Newbury Park, CA:
Sage; 1992.
Cheong J, Mackinnon D, Khoo ST. A latent growth modeling approach to
mediation analysis. In: Collins LM, Sayer AG, editors. New methods
for the analysis of change, 2001. p. 390–2.
Chapman CR, Donaldson GW, Nakamura Y, Jacobson RC, Bradshaw DH,
Gavrin J. A psychophysiological causal model of pain report validity.
J Pain 2002;3:143–55.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed.
Hillsdale, NJ: Lawrence Earlbaum Associates; 1988.
Craig ADB. Pain mechanisms: labeled lines versus convergence in central
processing. Annu Rev Neurosci 2003;26:1–30.
Dorn LD, Susman EJ, Nottelmann ED, Inoff-Germain ED, Ghrousos GP.
Perceptions of puberty: adolescent, parent and health care personnel.
Dev Psychopathol 1990;26:322–9.
Dowling J. Autonomic measures and behavioral indices of pain sensitivity.
Pain 1983;16:193–200.
Dukes PM, Litt IF, Gross RT. Adolescents’ self-assessment in sexual
maturation. Pediatrics 1980;66:918–20.
Fillingim RB, Maixner W. Gender differences in the responses to noxious
stimuli. Pain Forum 1995;4:209–21.
Frankowski B, Duke-Duncan P, Guillot A, McDougal D, Wasserman R,
Young P. Young adolescents’ self-assessment of sexual maturation. Am
J Dis Child 1987;141:385–6.
Gil KM, Edens JL, Wilson JJ, Raezer LB, Kinney TR, Schultz WH,
Daeschner C. Coping strategies and laboratory pain in children with
sickle cell disease. Ann Behav Med 1997;19:22–9.
Hollingshead AB. Four-factor index of social status. Yale University:
Department of Sociology, 1975.
Holstege G, Bandler R, Saper CB. The emotional motor system. Prog Brain
Res 1996;107:3–6.
193
Jassen SA. Negative affect and sensitization to pain. Scand J Psychol 2002;
43:131–9.
LeResche L. Gender considerations in the epidemiology of chronic pain. In:
Crombie IK, Croft PR, Linton SJ, LeResche L, Von Korff M, editors.
Epidemiology of pain. Seattle: IASP Press; 1999. p. 43–52.
Matthews KA, Salomon K, Kenyon K, Allen MT. Stability of children’s
and adolescents’ hemodynamic responses to psychological challenge: a
three-year longitudinal study of a multiethnic cohort of boys and girls.
Psychophysiology 2002;39:826–34.
Meier PM, Berde CB, DiCanzio J, Zurakowski D, Sethna NF. Quantitative
assessment of cutaneous thermal and vibration sensation and thermal
pain detection thresholds in healthy children and adolescents. Muscle
Nerve 2001;24:1339–45.
Morris NM, Udry JR. Validation of self-administered instrument to assess
stage of adolescent development. J Youth Adolesc 1980;9:271–80.
Naliboff BD, Berman S, Chang L, Derbyshire SWG, Suyenobu B,
Vogt BA, Mandelkern M, Mayer EA. Sex-related differences in IBS
patients: central processing of visceral stimuli. Gastroenterology 2003;
124:1738–47.
Piira T, Taplin JE, Goodenough B, von Baeyer CL. Cognitive-behavioural
predictors of children’s tolerance of laboratory-induced pain: implications for clinical assessment and future directions. Behav Res Ther
2002;40:571–84.
Porro CA, Cettolo V, Francescato MP, Baraldi P. Functional activity
mapping of the mesial hemispheric wall during anticipation of pain.
NeuroImage 2003;19:1738–47.
Price DD. Central neural mechanisms that interrelate sensory and affective
dimensions of pain. Mol Interv 2002;2:392–403.
Riley JL, Robinson ME, Wise EA, Myers CD, Fillingim RB. Sex
differences in the perception of noxious experimental stimuli: a metaanalysis. Pain 1998;74:181–7.
Schlossberger NM, Turner RA, Irwin CE. Validity of self-report of
pubertal maturation in early adolescents. J Adolesc Health 1992;13:
109–13.
Schmidt NB, Santiago HT, Trakowski JH, Kendren JM. Pain in patients
with panic disorder: relation to symptoms, cognitive characteristics and
treatment outcome. Pain Res Manag 2002;7:132–41.
Singer JD, Willett JB. Applied longitudinal data analysis: modeling change
and event occurrence. Oxford: University Press; 2003.
SPSS for Windows. Rel. 12.0.0. Chicago: SPSS Inc.; 2003.
Steiner H, Ryst E, Berkowitz J, Gschwendt M, Koopman C. Boys’ and
girls’ response to stress: affect and heart rate during a speech task.
J Adolesc Health 2002;306:14–21.
Stoney CM, Davis MC, Matthews KA. Sex differences in physiological
responses to stress and in coronary heart disease: a causal link?
Psychophysiology 1987;24:127–31.
Tanner JM. Growth at adolescence: with a general consideration of the
effects of hereditary and environmental factors upon growth and
maturation from birth to maturity. Oxford: Blackwell Scientific
Publications; 1962.
Tanner JM. Growth and endocrinology of the adolescent. In: Gardner LJ,
editor. Endocrine and diseases of childhood. 2nd ed. Philadelphia: W B
Saunders; 1975. p. 14–64.
Thayer JF, Siegle GJ. Neurovisceral integration in cardiac and emotional
regulation. IEEE Eng Med Biol Mag 2002;21(4):24–9.
Tsao JCI, Myers CD, Craske MG, Bursch B, Kim SC, Zeltzer LK. Role of
anticipatory anxiety and anxiety sensitivity in children’s and adolescents’
laboratory pain responses. J Pediatr Psychol 2004;29:379–88.
Unruh AM. Gender variations in clinical pain experience. Pain 1996;65:
123–67.
Walco GA, Dampier CD, Hartstein G, Djordjevic D, Miller L. The
relationship between recurrent clinical pain and pain threshold in
children. In: Krane EJ, editor. Advances in pain research therapy,
vol.15. New York: Raven Press; 1990. p. 333–40.