Journal of Perinatology (2006) 26, 180–184
r 2006 Nature Publishing Group All rights reserved. 0743-8346/06 $30
www.nature.com/jp
ORIGINAL ARTICLE
Mild hypothermia via selective head cooling as neuroprotective
therapy in term neonates with perinatal asphyxia: an experience
from a single neonatal intensive care unit
Z-L Lin1, H-M Yu2, J Lin3, S-Q Chen1, Z-Q Liang1 and Z-Y Zhang1
1
Department of Neonatology, Yuying Children’s Hospital of Wenzhou Medical College, Wenzhou, China; 2Department of Pediatrics,
Zhejiang University School of Medical, Hangzhou, China and 3Department of Pediatrics, Mount Sinai School of Medicine, New York,
USA
Objective: The objective of this study was to determine the efficacy of mild
hypothermia via selective head cooling as a neuroprotective therapy in term
infants with perinatal asphyxia.
Study design: Full-term newborns who had 5 min Apgar scores <6, first
arterial blood gas pH<7.10 or BD>15 mEq/l, and with the clinical signs
of encephalopathy were enrolled within 6 h after birth. Patients were
randomized to receive mild hypothermia treatment via selective head
cooling for a total of 72 h or receive routine treatment as a control. Brain
hypoxic-ischemic injury was quantified based on the head computed
tomographic scan (CT scan) at postnatal age 5–7 days and a Neonatal
Behavioral Neurological Assessment (NBNA) score at 7–10 days of life.
Results: A total of 58 patients (30 hypothermia, 28 control) completed
the study. Hypothermia was well tolerated in this study and attenuated the
hypoxic-ischemic brain injury due to perinatal asphyxia. Head CT scan
demonstrated moderate to severe hypoxic-ischemic changes in only 4/30
cases from the hypothermic group. In contrast, 18/28 cases in the control
group showed moderate to severe hypoxic-ischemic changes (w2 ¼ 15.97,
P<0.01). Brain hypothermia also significantly improved the NBNA score
(32±2 in the hypothermic group vs 28±3 in the control group, P<0.01).
Conclusions: Our results suggest that selective head cooling may be used
as a neuroprotective therapy in term neonates with perinatal asphyxia. A
long-term follow-up study is needed to further validate the results of this
study.
Journal of Perinatology (2006) 26, 180–184. doi:10.1038/sj.jp.7211412;
published online 12 January 2006
Keywords: perinatal, asphyxia; hypoxic-ischemic encephalopathy;
newborn, infant; induced, hypothermia
Correspondence: Dr Z-L Lin, Department of Neonatology, Yuying Children’s Hospital of
Wenzhou Medical College, Wenzhou 325027, China.
E-mail: linzhenlang@hotmail.com
Received 14 June 2005; revised 19 September 2005; accepted 22 September 2005; published
online 12 January 2006
Introduction
Hypoxic-ischemic encephalopathy (HIE) due to perinatal asphyxia
remains one of the major causes of neonatal death and later
neurodevelopmental disability. There are limited therapeutic
interventions available to rescue brain function during or
immediately after perinatal asphyxia. The prognosis for an infant
diagnosed with HIE has not changed during the past two decades.
It is estimated that 25–30% of HIE survivors will have long-term
neurodevelopmental disabilities that include cerebral palsy, seizure
disorder and mental retardation.1 The magnitude of HIE due to
perinatal asphyxia is much worse in developing countries such as
China.2
Over the past two decades, our understanding of the
mechanisms of neonatal HIE has increased dramatically from
experiments both in vitro and in vivo. It is well accepted that
depletion of cellular stores of high-energy phosphates, principally
ATP and phosphocreatine, initiates the cascade of events leading to
neuronal death after hypoxic ischemia.3,4 On the basis of extensive
animal studies, there is increasing evidence suggesting that mild or
moderate brain hypothermia is an effective intervention to
ameliorate the neuronal injury due to hypoxic ischemia.5–7 A few
small clinical trials have demonstrated the safety of head cooling
when used in neonates with HIE.8,9 The purpose of this study was
to use this simple method to treat full-term infants with perinatal
asphyxia and examine its measurable efficacy compared to a
control group that received routine treatment.
Patients and methods
This study was approved by the Ethics Committee of Yuying
Children’s Hospital of Wenzhou Medical College. After written
consent from parents, newborn infants admitted to the Yuying
Children’s Hospital of Wenzhou Medical College from July 1, 2000
to June 30, 2003 were enrolled into the study when the following
criteria were fulfilled: (1) gestational age X37 weeks; (2) Apgar
scores <6 at 5 min with first postnatal arterial blood gas pH<7.10
Selective head cooling in newborn infants with asphyxia
Z-L Lin et al
181
or BD>15 mEq/l; and (3) the clinical signs of postpartum
encephalopathy (decreased muscle tone, lethargy, coma, or
seizures) starting within 6 h after birth. Consecutively admitted
patients who met the inclusion criteria were randomized to the
hypothermic group or the control group based on whether it was
on an odd or even day of admission. Infants with major congenital
anomalies and prolonged hypoxemia due to severe persistent fetal
circulation were excluded from the study.
Once a patient was enrolled, the complete obstetric history was
obtained, and the degree of HIE was determined with Sarnat’s
clinical staging system by our attending neonatologists.10 In the
hypothermic group, selective head cooling was initiated as soon as
the patient was admitted and enrolled. The selective head cooling
was achieved by applying a cooling cap device (SDL-V) with
circulating cold water at 101C (10±11C) (Tianyuan Scientific
Development Inc. Changchun, China). The patients were kept
under a radiant warmer with the targeted temperature set at 34–
351C for a total of 72 h. A shield was used to block the cooling cap
from the radiant heat during head cooling. An indwelling rectal
temperature (TR) probe was used to monitor the temperature
constantly and used as the target temperature. Nasopharyngeal
temperature (TNP) was also monitored during head cooling.
Infants were then spontaneously rewarmed in room temperature to
a normal temperature after the completion of 72 h of head cooling.
The radiant warmer was added for rewarming if a patient’s TR
remained less than 36.01C after 12 h from the completion of head
cooling. The serum electrolytes were monitored daily and routine
liver enzymes checked on day 3. The vital signs including TNP and
TR were monitored continuously and recorded bihourly in our
NICU during the study period. The control group received the same
neonatal intensive care and monitoring except head cooling. Their
TR was measured with a regular thermometer not by constant
rectal probe. All patients in both groups were treated with a loading
dose of 20 mg/kg of phenobarbital (regardless of having clinical
seizures or not) as soon as they were enrolled and then 5 mg/kg
per day for a minimum of 72 h as part of our NICU routine
treatment protocol for HIE patients. An additional 5–10 mg/kg of
phenobarbital was administered if clinical seizures continued and
the phenobarbital levels were subtherapeutic. Furthermore, all
patients were kept on maintenance intravenous fluids (10%
dextrose water with or without sodium and potassium) and NPO
for at least 72 h. Dopamine at 5 mg/kg/min was also routinely used
in both groups to maintain a normal blood pressure or for renal
blood perfusion during the 72-h study period.
A cranial head computed tomographic (CT) scan (GE 2000)
was obtained on all enrolled infants at 5–7 postnatal days. All CT
scans were reviewed by a neuroradiologist without the knowledge of
group assignment. The extent and location of hypodensity areas
were used to quantify the brain injury into three grades as
previously described by Fitzhardinge et al.11: (1) Mild: scattered,
minor areas of hypodensity usually localized in the periventricular
area with some extension into the frontal or parieto-occipital areas
of the cortex; (2) Moderate: widespread involvement extending
from white matter well into the gray matter giving a mottled
appearance; and (3) Severe: homogeneous decreased brain tissue
density throughout most of the supratentorial compartment with
only the basal ganglia and cerebellum presenting as normal
density and the lateral ventricles small and compressed. The
presence of intraparenchymal or intraventricular hemorrhage was
graded as severe.
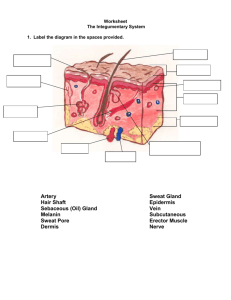
A well-described 20-item Neonatal Behavioral Neurological
Assessment (NBNA) score was also used in the study. The NBNA
score system, which was modified from the Brazelton Neonatal
Behavioral Assessment Scale (BNBAS),12 has been well described
before in detail and used as an assessment tool for neurological
impairment in HIE patients.13,14 NBNA contains five clusters:
behavior (six items); passive tone (four items); active tone (four
items); primary reflexes (three items); and general assessment
(three items). Each item of NBNA can be scored as 0, 1 or 2, and
has a maximum score of 40 for normal full-term infants.13 The
scoring was done in all patients at 7–10 days of life by two
specially trained individual investigators. If the scores were different
between the two investigators, the mean value of the two scores was
used. All statistical analysis was performed by using the SPSS 8.0
software and data presented as mean and s.d. when appropriate.
Analysis of variance (ANOVA), Student’s t-test and w2 were used to
compare the difference between two groups, and P<0.05 was
considered to be statistically significant.
Results
There were a total of 62 patients enrolled into the study during the
study period, among them 32 in the hypothermic group and 30 in
the control group. There were only nine cases (four from
hypothermic group and five from control group) who were
intubated upon admission for ventilatory support. There were four
deaths (two in each group) after enrollment into the study due to
multiorgan failure secondary to severe asphyxia and parental wish
to withdraw therapy. Therefore, a total of 58 patients completed the
study. The demographic data and characteristics of the two groups
are presented in Table 1. There are no significant differences
between the two groups for all the factors listed.
All enrolled patients were born in other community hospitals or
clinics and were immediately transferred to the Yuying Children’s
Hospital if the patient had an Apgar score <6 at 5 min. Most of the
enrollments were within 4 h after birth. Both groups were relatively
hypothermic at admission due to the lack of a neonatal transport
incubator for transporting patients. Once enrolled into the
hypothermic group, it took an average of 55±20 min to cool the
temperature down to the target level. After 72 h of head cooling, it
took an average of 300±50 min to rewarm the patients to a
normal temperature.
Journal of Perinatology
Selective head cooling in newborn infants with asphyxia
Z-L Lin et al
182
Table 1 The demographic data and initial clinical characteristics of the
study population
Hypothermia (n ¼ 30)
Control (n ¼ 28)
Gender (M/F)
Gestational age (weeks)
Birth weight (kg)
Maternal age (years)
Enrollment time (h)
Apgar score (5 min)
HIE grade I/II/III
18/12
38.7±1.3
3.31±0.47
27±5
3.6±1.3
3±1
7/16/7
17/11
39.1±1.6
3.43±0.52
24±3
3.8±1.2
3±1
7/15/6
First arterial blood gas
pH
BD (mEq/l)
7.05±0.12
15.9±4.6
7.07±0.11
15.6±4.8
Admission temperature
TNP (1C)
TR (1C)
35.8±0.4
35.6±0.5
35.8±0.4
35.7±0.4
Table 3 The number of cases with different degree of HIE changes on
head CT scan in hypothermia treatment or control patients at 5–7 days
of age
Group
n
Normal to mild
Moderate to severe
Hypothermia
Control
30
28
26
10
4
18
w2 ¼ 15.97, P<0.01.
Table 2 Changes in temperatures, heart rate and mean arterial blood
pressure starting from enrollment in both hypothermia treatment and
control group infants
Group
Time (h)
0
12
24
48
72
Hypothermia (n ¼ 30)
HR (beats/min) 138±15 110±8*
108±6*
106±7*
107±8*
MAP (mmHg)
47±5
48±4
49±7
50±8
48±7
TNP (1C)
35.8±0.4 34.2±0.4* 34.1±0.5* 34.7±0.3* 34.4±0.5*
TR (1C)
35.6±0.5 35.0± 0.6* 34.9±0.6* 34.8±0.5* 34.5±0.5*
Control (n ¼ 28)
HR (beats/min) 140±10 136±12
MAP (mmHg)
49±8
48±7
TNP (1C)
35.8±0.4 36.9±0.4
TR (1C)
35.7±0.4 36.8± 0.6
132±10
48±8
37.1±0.5
36.9±0.6
138±11
51±7
37.0±0.3
37.1±0.5
135±13
47±6
36.8±0.5
37.1±0.3
*P<0.05 compared to control group.
The changes of temperature, heart rate and mean blood
pressure during the 72 h trial period are presented in
Table 2. As expected, the heart rates in the hypothermic group
were significantly lower than the control group. However, the
mean blood pressures were maintained by the routine use of
dopamine. The hypothermia was well tolerated by all the
patients in the hypothermic group. There was no difference
between the two groups for electrolytes, liver enzymes, blood
urea nitrogen (BUN) and creatinine levels during the 72-h period
(data not shown).
Journal of Perinatology
Figure 1 Neonatal Behavioral Neurological Assessment (NBNA) scores
in hypothermia treatment and control group. Mild hypothermia via
selective head cooling significantly improves the NBNA score in term
infants with perinatal asphyxia at 7–10 days of life.
Hypothermia treatment significantly attenuated the acute
hypoxic-ischemic brain injury based on the head CT scan done at
5–7 days of life and NBNA score at 7–10 days of life. In the
hypothermia treatment group, there were four out of 30 total cases
with moderate to severe hypoxic-ischemic changes seen on head
CT scan. In contrast, 18 of 28 cases in control group demonstrated
moderate to severe hypoxic-ischemic changes (P<0.01, Table 3).
As seen in the Figure 1, brain hypothermia treatment also
significantly improved the NBNA score performed at 7–10 days
of life (32±2 vs 28±3, P<0.01).
Discussion
There is a long history of using hypothermia for trauma patients to
prevent further tissue injury. In the care of neonates, some
clinicians used hypothermia to treat asphyxiated neonates as early
as in 1950s.5,15 After extensive experiments in animal models,
several pilot or small clinical trials using hypothermia for
neuroprotection in asphyxiated full-term infants have been
performed.8,9,16–19 From those pilot human studies it appears that
mild hypothermia is safe when used in term infants with perinatal
Selective head cooling in newborn infants with asphyxia
Z-L Lin et al
183
asphyxia as long as close monitoring can be implemented in the
NICU setting.
With our particular setting and patient population, we are able
to demonstrate in this randomized intent-to-treat clinical trial that
mild hypothermia for 72 h via selective head cooling started within
6 h of perinatal asphyxia can significantly attenuate the brain
injury based on the head CT scan and NBNA score changes at
about 1 week of life. Areas in brain tissue with decreased density are
a common finding in term infants with HIE, the degree of which
has been correlated with subsequent neurodevelopmental defect.11
Further studies using diffusion-weighted magnetic resonance
imaging and quantitative magnetic resonance spectroscopy may be
needed,20,21 but these modalities are not readily available to a
developing country such as ours. The NBNA scoring system, which
was modified from the BNBAS by Bao et al.13,14 in China, has been
used to predict neurodevelopmental outcome. A similar scoring
system has also been used by other investigators in other parts of
the world for predicting neurodevelopmental outcome in HIE
patients.22 We understand the limitation of these clinical tools for
evaluating the acute neurological outcome of patients. A long-term
neurological outcome follow-up study of our enrolled patients will
significantly enhance the value of this study.
There are several other limitations to our study. This is an
intent-to-treat clinical trial carried out in a single children’s
medical center and the number of patient enrolled was relative
small. The study assignment was not blinded to investigators. The
randomization method based on the odd or even day, which was
specifically designed to fit our staff scheduling, was not considered
to be a strict randomization. Further, all enrolled patients were
born in other hospitals or clinics and the acute perinatal care was
inadequate in most of those community hospitals. Almost all of the
babies enrolled in this study were born vaginally (only two babies
in hypothermia group and one baby in control group were born by
cesarian section). During the study period, most of the local
perinatal care providers had not been adequately trained in the
neonatal resuscitation program, and most of the asphyxiated babies
might not have been properly resuscitated at delivery room. Some
severe HIE cases probably died soon after birth in local community
hospitals before they had a chance to be admitted to the only level
three NICU in the region. Therefore, only a few severe HIE cases
were enrolled in this study and patient population might be
different from those seen in other developed countries where a
multicenter trial of using head cooling for HIE was conducted
recently.23 However, the beneficial effects of using selective head
cooling in our particular patient population are consistent with the
report of the international multicenter trial. In that report,
hypothermia was only effective in patients with moderate HIE based
on the results of initial amplitude-integrated
electroencephalography.23
In our study, therapeutic dose of phenobarbital was routinely
used in every enrolled patient. Thoresen et al.24 has shown that
hypothermia alone without sedation was not effective in protecting
the brain tissues of newborn piglets after a severe global hypoxicischemic insult. We speculate that the use of phenobarbital may
help to reduce cerebral metabolism and oxygen consumption25 and
facilitate the hypothermia process, which might enhance the
neuroprotection of head cooling for infants with perinatal asphyxia.
Although it remains controversial whether using high-dose
phenobarbital alone is neuroprotective in asphyxiated infants,4,26
prophylactic use of a conventional dose of phenobarbital for a few
days in asphyxiated infants remains a common practice in China.
On the other hand, routine use of dopamine for asphyxiated term
infants is not a common practice. Based on our experience with
asphyxiated infants, as well as reported hemodynamic and renal
perfusion changes in other studies,8,9,27 we decided to use dopamine
at 5 mg/kg/min for all enrolled patients to prevent hypothermiarelated adverse hemodynamic changes, and as an attempt to
improve renal blood flow.
Impaired cardiac, liver and renal functions are common
clinical presentations in asphyxiated patients.28 As expected, on
average our enrolled patients in both group had elevated BUN,
creatinine and liver enzymes compared to the normal values,
however, there were no statistical difference for any of those
parameters between our hypothermic treatment group and control
group. Further, there were no obvious abnormal bleeding
symptoms recognized in any of those 58 patients, although clotting
factors were not routinely measured in all patients. Mild
hypothermia was therefore well tolerated by our enrolled patients
and no adverse effect related to hypothermia was recorded in our
study, which is consistent with other reported clinical trials.8,17,23
In conclusion, our study adds data suggesting that mild
hypothermia via selective head cooling in term neonates with
perinatal asphyxia is relatively safe and can be used in a regular
NICU setting. Mild hypothermia does not aggravate cardiac, hepatic
and renal dysfunction if close monitoring can be implemented.
More importantly, our data suggest that the mild hypothermia via
selective head cooling has a potential to be used as neuroprotective
therapy in term neonates with perinatal asphyxia. A long-term
follow-up study is needed to further validate the results of this study.
Abbreviations
HIE, hypoxic-ischemic encephalopathy; TNP, nasopharyngeal
temperature; TR, rectal temperature; CT scan, computed
tomographic scan; NBNA, Neonatal Behavioral Neurological
Assessment
Acknowledgments
We wish to thank the entire staff members of the NICU of Yuying Children’s Hospital
of Wenzhou Medical College for helping to complete the study and Drs Sidhartha
Tan and Ian Holzman for the critical review and comments of the manuscript.
Journal of Perinatology
Selective head cooling in newborn infants with asphyxia
Z-L Lin et al
184
References
1 Vannucci RC, Perlman JM. Interventions for perinatal hypoxic-ischemic
encephalopathy. Pediatrics 1997; 100: 1004–1014.
2 Xu JL, Gao XX, Wang SX. Retrospective analysis of neonatal hypoxicischemic encephalopathy in last 10 years. Chin J Perinatal Med 2001; 4:
236–239 (Chinese).
3 Whitelaw A. Systemic review of therapy after hypoxic-ischemic brain injury
in the perinatal period. Semin Neonatol 2000; 5: 33–40.
4 Grow J, Barks JDE. Pathogenesis of hypoxic-ischemic cerebral injury in the
term infant: current concepts. Clin Perinatol 2002; 29: 585–602.
5 Miller JA, Miller FS, Westin B. Hypothermia in the treatment of asphyxia
neonatorum. Biol Neonate 1964; 6: 148–163.
6 Gunn AJ, Gunn TR, Haan HH, Williams CE, Gluckman PD. Dramatic
neuronal rescue with prolonged selective head cooling after ischemia in fetal
lambs. J Clin Invest 1997; 99: 248–256.
7 Thoresen M, Simmonds M, Satas S, Tooley J, Silver IA. Effective selective
head cooling during posthypoxic hypothermia in newborn piglets. Pediatr
Res 2001; 49: 594–599.
8 Gunn AJ, Gluckman PD, Gunn TR. Selective head cooling in newborn infants
after perinatal asphyxia: a safety study. Pediatrics 1998; 102: 885–892.
9 Akisu M, Huseyinov A, Yalaz M, Cetin H, Kultursay N. Selective head cooling
with hypothermia suppresses the generation of platelet-activating factor in
cerebrospinal fluid of newborn infants with perinatal asphyxia.
Prostaglandins Leukot Essent Fatty Acids 2003; 69: 45–50.
10 Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A
clinical and electroencephalographic study. Arch Neurol 1976; 33: 696–705.
11 Fitzhardinge PM, Flodmark O, Fitz CR, Ashby S. The prognostic value of
computed tomography as an adjunct to assessment of the term infant with
postasphyxial encephalopathy. J Pediatr 1981; 99: 777–781.
12 Als H, Tronick E, Lester BM, Brazelton TB. The brazelton neonatal
behavioral assessment scale (BNBAS). J Abnorm Child Psychol 1977; 5:
215–231.
13 Bao XL, Yu RJ, Li ZS, Zhang BL. Twenty-item behavioral neurological
assessment for normal newborns in 12 cities of China. Chin Med J 1991;
104: 742–746.
14 Bao XL, Yu RJ, Li ZS. 20-item neonatal behavioral neurological assessment
used in predicting prognosis of asphyxiated newborn. Chin Med J 1993; 106:
211–215.
15 Westin B, Miller J, Nyberg R, Wedenberg E. Neonatal asphyxia pallida treated
with hypothermia alone or with hypothermia and transfusion of oxygenated
blood. Surgery 1959; 45: 868–879.
Journal of Perinatology
16
17
18
19
20
21
22
23
24
25
26
27
28
Thoresen M, Whitlaw A. Cardiovascular changes during mild therapeutic
hypothermia and rewarming in infants with hypoxic-ischemic encephalopathy. Pediatrics 2000; 106: 92–99.
Battin MR, Dezoete JA, Gunn TR, Gluckman PD, Gunn AJ. Neurodevelopmental outcome of infants treated with head cooling and mild hypothermia
after perinatal asphyxia. Pediatrics 2001; 107: 480–484.
Shankaran S, Laptook A, Wright LL, Ehrenkranz RA, Donovan EF, Fanaroff
AA et al. Whole-body hypothermia for neonatal encephalopathy: animal
observations as a basis for a randomized, controlled pilot study in term
infants. Pediatrics 2002; 110: 377–385.
Battin MR, Penrice J, Gunn TR, Gunn AJ. Treatment of term infants with
head cooling and mild systemic hypothermia (35.0 and 34.51C) after
perinatal asphyxia. Pediatrics 2003; 111: 244–251.
Martin E, Buchli R, Ritter S, Regula S, Remo LH, Eugen B et al. Diagnostic
and prognostic value of cerebral 31P magnetic resonance spectroscopy in
neonates with perinatal asphyxia. Pediatr Res 1996; 40: 749–758.
Krishnamoorthy KS, Soman TB, Takeoka M, Schaefer PW. Diffusionweighted imaging in neonatal cerebral infarction: clinical utility and followup. J Child Neurol 2000; 15: 592–602.
Thompson CM, Puterman AS, Linley LL, Hann FM, van der Elst CW, Molteno
CD et al. The value of a scoring system for hypoxic ischemic encephalopathy
in predicting neurodevelopmental outcome. Acta Paediatr 1997; 86:
757–761.
Gluckman PD, Wyatt JS, Azzopardi D, Ballard R, Edwards A, Ferriero D et al.
Selective head cooling with mild systemic hypothermia to improve
neurodevelopmental outcome following neonatal encephalopathy: the
coolcap study. Lancet 2005; 365: 663–670.
Thoresen M, Satas S, Loberg EM, Whitelaw A, Acolet D, Lindgren C et al.
Twenty-four hours of mild hypothermia in unsedated newborn pigs starting
after a severe global hypoxic-ischemic insult is not neuroprotective. Pediatr
Res 2001; 50: 405–411.
Nilsson L. The influence of barbiturate anaesthesia upon the energy state
and upon acid–base parameters of the brain in arterial hypotension and in
asphyxia. Acta Neurol Scand 1971; 47: 233–253.
Hall RT, Hall FK, Daily DK. High-dose phenobarbital therapy in term
newborn infants with severe perinatal asphyxia: a randomized, prospective
study with three-year follow-up. J Pediatr 1998; 132: 345–348.
Guignard JP, Gillieron P. Effect of modest hypothermia on the immature
kidney. Acta Paediatr 1997; 86: 1040–1041.
Piazza AJ. Postasphyxial management of the newborn. Clin Perinatol 1999;
26: 749–765.