Emerging Concepts in Periventricular White Matter Injury
advertisement

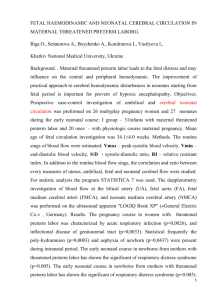
Emerging Concepts in Periventricular White Matter Injury Stephen A. Back, MD, PhD,* and Scott A. Rivkees, MD† Approximately 10% of newborns are born prematurely. Of these children, more than 10% will sustain neurological injuries leading to significant learning disabilities, cerebral palsy, or mental retardation, with very low birth weight infants having an even higher incidence of brain injury. Whereas intraventricular hemorrhage was the most common form of serious neurological injury a decade ago, periventricular white matter injury (PWMI) is now the most common cause of brain injury in preterm infants. The spectrum of chronic PWMI includes focal cystic necrotic lesions (periventricular leukomalacia; PVL) and diffuse myelination disturbances. Recent neuroimaging studies support that the incidence of PVL is declining, whereas diffuse cerebral white matter injury is emerging as the predominant lesion. Factors that predispose to PVL include prematurity, hypoxia, ischemia, and inflammation. It is believed that injury to oligodendrocyte (OL) progenitors contributes to the pathogenesis of myelination disturbances in PWMI by disrupting the maturation of myelin– myelin-forming oligodendrocytes. Other potential mechanisms of injury include activation of microglia and axonal damage. Chemical mediators that may contribute to white matter injury include reactive oxygen (ROS) and nitrogen species (RNS), glutamate, cytokines, and adenosine. As our understanding of the pathogenesis of PWMI improves, it is anticipated that new strategies for directly preventing brain injury in premature infants will evolve. Semin Perinatol 28:405-414 © 2004 Elsevier Inc. All rights reserved. T he care of premature infants has improved markedly over the past few decades, resulting in striking improvements in the survival of very low birth weight (VLBW) infants (⬍1.5 kg). However, improved survival of premature infants has been accompanied by increasing recognition of longterm neurological deficits. At least 10% of preterm survivors will develop the spastic motor deficits of cerebral palsy and up to 50% will be identified with learning disabilities.1-6 Several forms of brain injury are observed in premature infants that include intraventricular hemorrhage (IVH), intraparenchymal hemorrhage, and PWMI. Whereas medical interventions have resulted in a pronounced decrease in the incidence of IVH,7,8 the incidence of PWMI is not decreasing.8,9 Thus PWMI is now the major neurological problem that affects VLBW infants. *Department of Pediatrics, Oregon Health Science University, Portland, OR. †Yale Child Health Research Center, Yale University, New Haven, CT. Address reprint requests to: Scott A. Rivkees, MD, Director, Yale Child Health Research Center, Yale Pediatrics, P.O. Box 208081, 464 Congress Avenue, New Haven, CT 06520. E-mail: Scott.Rivkees@yale.edu 0146-0005/04/$-see front matter © 2004 Elsevier Inc. All rights reserved. doi:10.1053/j.semperi.2004.10.010 Pathological Features of Periventricular White Matter Injury PWMI includes a spectrum of cerebral injury that ranges from focal injury to extensive cerebral white matter lesions (diffuse PWMI).8,10 PVL is characterized by focal cystic–necrotic lesions that commonly occur in the subventricular zone (SVZ) adjacent to the lateral ventricle and involve injury to all cellular elements.10 Such lesions may be accompanied by reduction in white matter volume, secondary cyst formation or ventricular enlargement. Multiple neuropathology studies indicate that diffuse PWMI is characterized by extensive regions in deep cerebral white matter that contain numerous reactive astrocytes (ie, “diffuse gliosis”) and fail to normally myelinate. Diffuse PWMI may be accompanied by PVL or occur as an isolated lesion.11-15 Although diffuse gliosis is believed to arise in response to extensive white matter damage, the injured cell types that provoke this gliosis remain unresolved but are hypothesized to be oligodendrocyte progenitors,10 because such lesions occur in a similar distribution to regions of myelination disturbance. Recent neuroimaging studies support that the incidence of cystic necrotic 405 406 lesions (PVL) is declining, whereas diffuse cerebral white matter injury is emerging as the predominant lesion.16-18 In these recent series, cystic PVL lesions accounted for less than 5% of cases. The ability to recognize neonatal white matter injury has been greatly facilitated by the use of diffusionweighted imaging (DWI).16 Using DWI, abnormal white matter signals are observed in up to 68% of former preterm infants when studied at term equivalency. Abnormalities detected with DWI are believed to reflect reduced myelin axonal myelination, but neuropathological confirmation is still lacking. Risk Factors for PWMI Several factors are associated with the development of PWMI, the most prominent of which is prematurity. Other risk factors include apnea with hypoxia, bradycardia, intrauterine growth retardation and preeclampsia. The major pathogenetic mechanisms proposed for PVL are maternal–fetal infection19,20 and impaired cerebrovascular autoregulation that results in cerebral ischemia.21,22 Either mechanism may be operative during fetal development or in the neonate, and are not mutually exclusive. Fetal exposure to endotoxins or cytotoxic cytokines occurs in the setting of chorioamnionitis, and in experimental models these agents can trigger white matter injury through vasoactive mechanisms that result in cerebral ischemia.23,24 Although inflammatory-mediated mechanisms related to maternal fetal infection in near-term and term infant are strongly correlated with risk for later cerebral palsy, recent studies have failed to identify a similar relationship in premature infants by examination of either intrauterine exposure to infection or inflammatory cytokines in neonatal blood.25,26 A complex interplay of factors related to cerebrovascular immaturity appear to predispose preterm human periventricular white matter to injury from ischemia. Vascular end zones exist in the cerebral white matter that are supplied by long or short penetrating arteries that arise from the pial arteries.27,28 Volpe has proposed that the occurrence of severe or persistent ischemia in vascular end zones of long penetrating arteries that supply the periventricular white matter may account for the focal cystic-necrotic lesions of PVL.8 The occurrence of less severe or briefer episodes of ischemia in the territory of more superficially situated end zones of short penetrating arteries may account for the more extensive myelination disturbances commonly associated with diffuse PWMI.8 Ample evidence supports that the propensity for the premature neonate to exhibit a pressure-passive circulation is related to disturbances of cerebral autoregulation.29-31 Basal cerebral blood flow in healthy preterm neonates is markedly lower than in term infants or adults.32-35 Basal flow to cerebral white matter was estimated to be less than 20% of gray matter.36 Direct experimental evidence that human periventricular white matter is selectively susceptible to ischemia is, however, lacking. Recently, Tsuji and coworkers provided indirect evidence with near infrared spectroscopy that impaired cerebrovascular autoregulation was highly correlated with the development of PVL and germinal matrix-intraven- S.A. Back and S.A. Rivkees tricular hemorrhage.37 With the advent of more sensitive modalities to identify the at-risk preterm neonate, it is clear that an understanding of the vascular basis of preterm white matter injury is needed and will require the application of new technologies in appropriate animal models (see below) to measure blood flow to defined regions of vulnerable white matter. The Developing Brain is at High Risk for Oxidant-Mediated Damage Oxidative stress resulting from the generation of injurious reactive species or oxidants is a well-established sequela of ischemia–reperfusion.38 Several models of perinatal asphyxia in the term fetus have demonstrated increased free radical generation in the developing cerebrum. Electron spin resonance studies found that free radical generation is most pronounced during the initial period of reperfusion.39,40 Elevations in lipid peroxidation products, protein carbonyls, and biomarkers of reactive nitrogen species were detected 8 minutes after the onset of reperfusion in a near term fetal rabbit model of placental insufficiency. Administration of antioxidants to the mother after the onset of this insult resulted in decreased brain injury implicating the important role of reactive species in brain injury from hypoxia–ischemia.41,42 The fetal brain is especially prone to lipid peroxidation-mediated injury, because of the abundance of membrane lipids.43,44 The aldehydes formed from lipid hydroperoxides are most specifically detected in glia by measurement of F2-isoprostanes.45 Increased lipid peroxidation has been observed in lipid extracts from the entire brain of normal premature guinea pigs that peaks at around 60% term gestation. Following hypoxia, increased lipid peroxidation was observed in brains obtained at around 80% term gestation.46 In the preterm human fetus, elevated lipid peroxidation products have been detected in periventricular white matter.15,47 In the preterm human fetus, antioxidant defenses appear to be underdeveloped compared with the term fetus.48 In guinea pig brain, most of the antioxidant enzyme systems increase and attain adult levels in the last 30% of the gestation period.49 The developing brain may be more vulnerable to oxidative damage due to a lag in the expression of the potentially protective enzymes superoxide dismutases-1 and -2, catalase, and glutathione peroxidase in the white matter of the human fetus.50 There is thus little direct information from experimental models about the extent of free radical generation in the preterm fetus in response to ischemia–reperfusion and cerebral white matter has not been specifically studied. Human Oligodendrocyte Development and Damage in PVL OLs develop according to a well-established lineage, defined by stage-specific antibodies specific for sequentially ex- Periventricular white matter injury Figure 1 The four stages of oligodendrocyte development. The antigens expressed at each stages are listed in the bottom panel. pressed OL cell-surface and myelin-specific epitopes.51,52 The successive OL stages are distinguished by a progressively more complex morphology (Fig. 1). The OL progenitor is identified by the A2B5 monoclonal antibody in vitro or by NG2, in vivo. The preOL is a simple multipolar, mitotically active late OL progenitor identified with the O4 but not the O1 monoclonal antibodies. The immature OL is a postmitotic complex multipolar cell identified by the O1 antibody that binds to galactocerebroside. The mature OL is identified by myelin-associated markers that include myelin basic protein. It is, thus, feasible to precisely define the timing and features of OL lineage progression both in vitro and in vivo. Since the major period of vulnerability for PWMI (23-32 weeks gestation) occurs before the onset of myelination, Volpe first proposed that the myelination disturbances of PWMI might arise from targeted death of OL progenitors that are the source of mature OLs.48 This hypothesis proposes that the predilection for PWMI is related to a developmentallyregulated susceptibility of more immature stages of the OL lineage to oxidative stress, a well-established sequela of both hypoxia–ischemia53 and maternal-fetal infection.20 In support of this hypothesis we found that the developmental window of highest risk for PWMI (ie, about 23-32 weeks postconceptional age) corresponds to a period in white matter development before the onset of myelination.51 This period coincides with the presence of one major population of preOLs in cerebral white matter and identifies the preOL as a target for injury in PWMI. The decline in risk for PWMI coincides with the onset of a wave of differentiation of preOLs to immature OLs that initiate myelination of periventricular white matter.52 Several lines of evidence in support of a role for targeted preOL death in the pathogenesis of PWMI derive from in vitro and in vivo experimental models. Maturation-Dependent Vulnerability of the Oligodendrocyte Lineage to Oxidative Stress OL progenitors display maturation-dependent vulnerability to oxidative stress in vitro and hypoxia–ischemia in vivo.54-59 407 The notion that OL progenitors display enhanced susceptibility to oxidative stress was initially supported by in vitro studies that compared the susceptibility of successive stages in the OL lineage to intrinsic and extrinsic sources of oxidative stress. We initially demonstrated that preOLs are markedly more susceptible than mature OLs to intrinsic and extrinsic sources of oxidative stress.54 We defined an oxidative stress pathway in which intracellular depletion of glutathione triggered a downstream rise in reactive oxygen species (ROS) that lead to preOL death. Interestingly, the E2-isoprostanes, a lipid peroxidation product, are particularly toxic to OL progenitors, but not mature OLs, which suggests that specific compounds generated endogenously from oxidative stress might be a potential mechanism for OL degeneration in PWMI.60 Several recent in vitro studies found that caspasemediated death of OL progenitors occurs and after oxidative stress in vitro.58,61,62 If targeted death of the preOL is related to the pathogenesis of PVL, then preOLs should demonstrate enhanced susceptibility to hypoxia–ischemia, a common sequela of critical illness in the premature neonate. In a perinatal rodent model of hypoxia–ischemia, we found that preOLs are highly susceptible to hypoxia–ischemia, whereas earlier and later OL stages are markedly more resistant. The enhanced susceptibility of preOLs was a stage-specific property that was independent of the postnatal age of the animal or the location of these cells in the forebrain. Hence, targeted death of preOLs could contribute to the pathogenesis of PWMI across a broad range of gestational ages and in multiple susceptible regions. We and others have found that caspase-mediated mechanisms of apoptosis at least partially contribute to preOL death from hypoxia–ischemia.56,63-65 In summary, multiple experimental studies support a developmental explanation for the predilection for PWMI to occur during prematurity that is related to the presence of a susceptible population of preOLs in the periventricular white matter. Microglia Induced Cell Injury The observation that activated microglia are present in the brains of infants with PVL, raises the possibility that this inflammatory cell type may contribute to preterm brain injury.14,66,67 Microglia are macrophage-derived cells involved in the response of the brain to inflammatory and metabolic insults.68-71 Microglia are present in the fetal brain by midgestation, and are expressed in developing white matter.72,73 Microglia are small, ramified cells with branching processes and dynamically respond to changes in the microenvironment.68-71 Microglia have membrane receptors for several neurotransmitters,74,75 including purinergic receptors74 that are stimulated by ATP and adenosine. Microglia are also responsive to excitatory neurotransmitters including glutamate71 In response to altered levels of neurotransmitters and/or cytokines, microglia are activated.68,71,76,77 Reactive microglia are nonramified cells that secrete a variety of cytokines that exert toxic effects on neurons and oligodendrocytes.68,71,76,77 These factors include tumor necrosis factor-␣ (TNF-␣), IL-1, interferon-gamma (INF-␥) and superoxide 408 radicals.68,71,76,77 Microglial factors that may project against cell injury including the cytokines TGF-1, IL-4, bFGF and NGF.68,71,76,77 Nitric oxide production by activated microglia generates reactive nitrogen species that are toxic to both preOLs and mature OLs in vitro.78-82 In vitro studies also support the notion that microglial are required to promote the toxicity of inflammatory mediators. Vartanian showed that activation of the microglial Toll-like receptor TLR4 is required for endotoxin to promote the acute degeneration of oligodendrocyte progenitors in vitro.83 Perinatal Neuronal Injury Despite the particular predilection of the preterm infant to white matter pathology, increasing evidence suggests that neuro-axonal gray matter injury may contribute to the longterm deficits that accompany PWMI in survivors of premature birth. Volumetric MRI studies of infants with PWMI found reductions in gray matter volumes in several brain regions that prominently included the cerebral cortex.84 There have been, however, no neuropathological studies to directly account for the mechanisms underlying the reductions in gray matter volume. Although the cerebral cortex is typically spared in PWMI, extensive neuronal necrosis, thalamic infarcts and pontosubicular necrosis can be observed together with PWMI.10 A number of recent experimental findings are consistent with maturation-dependent susceptibility of developing gray matter to hypoxia–ischemia. We recently reported that after hypoxia–ischemia, preterm fetal rabbits sustained injury to the basal ganglia and anterior thalamus, which are major components of subcortical motor pathways. At birth, hypertonic motor deficits that resemble early cerebral palsy were observed in the preterm survivors. These regions are particularly susceptible to hypoxic–ischemic injury in both preterm and term infants.85,86 Likewise, the thalamus and basal ganglia are particularly susceptible to hypoxia–ischemic injury in preterm and near-term fetal sheep subjected to global cerebral hypoperfusion87 (Back and Hohimer, unpublished observations). It, thus, appears that susceptibility of the developing gray matter to injury also will be maturation-dependent and involve preferential injury to particular neuronal populations. Within the cerebral cortex, fetal rabbits showed a predilection of apparent subplate neurons to injury consistent with recent observations that hypoxia–ischemia preferentially targets these neurons in the perinatal rat.88 In chronic sublethal hypoxia, reduction in gray matter volume is observed in several brain regions including the cerebral cortex, thalamus, and striatum.89 Recent data show that chronic sublethal hypoxia is associated with reduced neuronal number (see chapter by Schwartz and colleagues). In neonatal rats reared in 10% oxygen, H-NMR spectroscopy reveals lower levels of brain N-acetyl aspartate levels, which suggests reductions in neuronal number (R. Rao, personal communication). Levels of glutamate, GABA, and phosphocreatine are also lower than in control animals. Glutamate: glutamine ratios are higher in hypoxia, which indicates reduced neurotransmitter recycling. S.A. Back and S.A. Rivkees Several mediators of neuronal loss in the developing brain have been identified that include excitatory neurotransmitters, free radicals, and iron.90,91 Evidence recently generated from our laboratory suggests that the neuromodulator adenosine may contribute to injury in developing neurons by altering intracellular calcium levels.92 Although not well characterized in PWMI, it is likely that brain injury may be associated with altered levels of neurotrophic agents and other factors that influence axon growth and synaptogenesis. Potential Chemical Mediators of Preterm Brain Injury PWMI causation is complex and will likely involve the action of different neurochemicals and cytokines. In addition to reactive oxygen and nitrogen species, other factors considered to play a role in PWMI include excitatory amino acids, iron deposition, and inflammatory cytokines.93 Activated microglia release a number of cytokines that are toxic to OLs. The microglial products TNF-␣ and interferon-␥ (INF-␥) are directly toxic to preOLs and mature OLs94-97 and in combination their toxicity is synergistic.98 Recently, INF-␥ immunopositive cells were localized in necrotic foci in premature infants with white matter injury.99 Free iron contributes to the generation of toxic ROS and is directly toxic to oligodendrocytes. IVH increases the risk of PWMI and elevated levels of iron can be observed in the spinal fluid of such infants. Multiple studies indicate that OLs play a central role in CNS iron metabolism and, thus, may be at risk for ironmediated oxygen radical toxicity. Within the adult rodent and human CNS, including the white matter, ferric iron, ferritin, and transferrin localize primarily to OLs, as well as to some restricted populations of neurons, microglia and astrocytes.100-103 Myelin deficient rats, in which OLs fail to mature, show significant reductions in the distribution of iron, transferrin, and the transferrin receptor in the CNS.104-106 Degeneration of preOLs subjected to oxidative stress107 was prevented by pretreatment with the iron chelator desferrioxamine. A photochemically induced rise in ROS was also blocked in OLs by desferrioxamine.108 In embryonic cortical neurons, a broader role for iron chelators was proposed based on the finding that the protection rendered by such compounds against oxidative stress-induced apoptosis involves the activation of a collection of hypoxia-responsive genes.109 Increased release of glutamate and glutamate action has been implicated in rodent studies of preterm white matter injury.110-112 It has been suggested that white matter injury is associated with elevations of extracellular glutamate, possibly due to axonal injury.8 In addition, with altered brain energy supply, glutamate uptake is reduced. Glutamate-induced injury to preOLs is mediated by ionotropic glutamate receptors (iGluRs) of the -amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA)/kainate type.55,113-117 Recent data show that preOLs also express metabotropic glutamate receptors (mGluRs).112 However, activation of group 1 mGluRs attenuates OL excitotoxicity by controlling downstream oxidative Periventricular white matter injury stress after iGluR overactivation.112 Nonreceptor-mediated mechanisms also can lead to glutamate-induced OL death.54,107,118 Excessive extracellular glutamate causes glutathione depletion in preOLs with consequent free radical generation.54 This effect is related to activation of a glutamate– cystine exchange transporter, which results in glutamate uptake and cystine efflux.119-121 In turn, intracellular cystine depletion leads to reduced glutathione synthesis, leading to depletion of free radical scavengers. Experimental Models of PWMI Several experimental models have been developed to provide insight into injury of the developing brain and include studies in rodents, rabbits, sheep and nonhuman primates. Models used to induce injury include ischemia–reperfusion, injection of endotoxin, administration of excitoxic agents, and rearing in chronic sublethal hypoxia. These models are complementary and it is not clear that any one model is fully representative of human PWMI.122,123 Rodents have been widely used for studies of neonatal brain injury. In mice and rats, the first two postnatal weeks are roughly similar to the last trimester of human gestation.124 To develop a model of perinatal H-I in the rat relevant to the high-risk period for PWMI in humans, we recently defined the timing of oligodendrocyte lineage progression in rats and mice. We identified a period in early rodent cerebral development when the distribution of OL lineage stages coincides with that of human during the high-risk period for PWMI.125 Each species was found to display a distribution of OL stages at postnatal day 2 (P2) that was similar to that seen in premature human cerebral white matter. At P2, the cerebral white matter of rodents, like premature infants,51 contains predominantly preOLs. These studies also predicted that if the vulnerable period for white matter injury in the rodent is centered around P2, then it should decline thereafter, coincident with the onset of oligodendrocyte differentiation and myelination between P7 and P14.126 We, confirmed that white matter injury in the rat is maximal at P2 and declines markedly by P7 when oligodendrocyte maturation occurs.56 It should be emphasized that this model and the widely used Rice-Vannucci P7 rodent model of focal hypoxia–ischemia127 do not closely reproduce the pathological features of PWMI in humans. These hypoxia–ischemia models generate extensive cortical and subcortical neuronal necrosis and apoptosis. The particular value of these models resides, in part, in the considerable experimental access they provide to questions related to cellular and molecular mechanisms of injury to immature cell types in the developing cerebrum. Excitotoxic agents also have been studied in perinatal rodents to mimic the effects of severe neonatal hypoxic–ischemic brain injury. Injection of AMPA or ibotenate in neonatal rodents induces focal white matter lesions that resemble cystic necrotic PVL.128-132 Whereas acute hypoxia–ischemia models commonly trigger cortico-neuronal necrosis together with white matter injury, rearing newborn rats or mice in chronic sublethal hypoxia (CSH; 9-10% oxygen) appears to result in diffuse PWMI 409 without focal necrosis.89 CSH results in features similar to those observed in PWMI, including ventriculomegaly, reduced white and gray matter volumes, and reduced myelination.89,133 Studies suggest that CSH is associated with arrested oligodendrocyte lineage progression, reduced myelination, and abnormal axon spouting.134,135 A distinct shortcoming of perinatal rodent models is that they do not reproduce the many distinct physiological features unique to the premature human infant. For this reason, a number of investigators are actively studying the pathological features of true fetal models. These studies have principally evaluated fetal rabbits, sheep and nonhuman primates. Preterm rabbit fetuses subjected to sustained global hypoxia– ischemia survive and display significant impairment of motor activity related to hypertonic motor deficits.136 Histopathological studies identified a distinct pattern of acute injury to subcortical motor pathways that involved the basal ganglia and thalamus.136 These findings suggest that the rabbit may provide a unique model for studying cerebral palsy. The instrumented immature (0.65 gestation) fetal sheep appears to be the optimal in utero animal model of relatively specific white matter damage.20 The 0.65 gestation fetal sheep is similar to human between 24 to 28 weeks in terms of the completion of neurogenesis, the onset of cerebral sulcation, and the detection of the cortical component of the auditory and somatosensory evoked potentials.137-139 We found that OL lineage maturation in 0.65 gestation ovine cerebral white matter is developmentally similar to the 23 to 28 week human fetus.140 Over the last 20 years there has been extensive in utero study of late-gestation fetal ovine cerebral blood flow and metabolic rate of oxygen consumption under normal and pathological conditions. Important studies focused on normal values and the vasodilatory role of hypoxia141,142 and hypercarbia.143 The immature fetus appears to be extremely vulnerable to hypotension and subsequent hypoxia– ischemia. The immature fetus also has even less autoregulatory capacity than the term fetus.144,145 The immature sheep fetus has a much lower cerebral blood flow (CBF) than the late gestation fetus.146-148 Most significantly anatomically undefined cerebral white matter of the immature fetus had only about 50% of the CBF of the cerebral cortex. These studies, however, provided no information regarding blood flow specifically to periventricular white matter. The predilection for periventricular white matter damage appears to be greater in the preterm fetal sheep. Reddy and coworkers reported an ovine model of white matter injury generated by severe brain hypoperfusion imposed by chronic bilateral ligation of the occipito-vertebral anastomosis and a 30-minute reversible occlusion of the carotid arteries.87 In the near term (0.9 gestation) fetus, this insult caused primarily selective neuronal loss in the upper layers of the cortex while in the immature fetus (0.65 gestation) the damage was primarily to subcortical white matter.149 Chronic placental insufficiency in the near term fetal sheep resulted in moderate hypoxemia, cerebral cortical gliosis and myelination disturbances of subcortical but not periventricular white matter.150 Severe hemorrhagic hypotension in the 0.6 gestation sheep caused periventricular white matter lesions in most (5/6) an- S.A. Back and S.A. Rivkees 410 imals.151 We are currently defining a model of graded global cerebral hypoperfusion. With increasing duration of ischemia, we generated graded selective cerebral white matter injury that replicates the major histopathological features of the spectrum of acute PWMI.140 Lipopolysaccharide (LPS) exposure in preterm and near term animals has been used to generate white matter injury in immature dogs, cats, and fetal sheep, and has been used to provide insights into inflammatory mechanisms of injury to the developing brain. LPS and umbilical cord occlusion both produce white matter injury with quite similar distribution in sheep about two-thirds through gestation.152 The morphological appearance is associated with pronounced infiltration of inflammatory cells into the brain and focal collections of microglia/macrophage. Of great interest is the potential use of nonhuman primates in the study of PWMI. As detailed in the chapter by Dr. Inder and coworkers in this issue, the preterm baboon infant cared for in a manner similar to human premature infants manifest many features of PWMI. Also of great interest is the rhesus macaque model of infection-induced preterm labor that closely mimics many of the key features of chorioamnionitis in the preterm infant.153,154 This model holds considerable promise to clarify the role of maternal-fetal infection in the pathogenesis of PWMI. The Role of Adenosine in White Matter Injury In the mature brain, adenosine plays an important neuroprotective role.155 However, evidence generated from in vitro and in vivo studies suggests that adenosine may play a critical role in the pathogenesis of hypoxia-related brain injury, and possibly PWMI. Adenosine is a nucleoside that is present in all cells and is a component of nucleic acids and energy carrying molecules.156 Adenosine levels can rapidly climb more than 100-fold with ischemia and increased tissue activity, providing a barometer of tissue activity and oxygenation.156 Specific cell surface receptors transduce adenosine action including A1 adenosine receptors (A1ARs) that are activated when modest elevations in adenosine levels occur and are distributed throughout the brain.157-159 The other cloned adenosine receptor subtypes include A2a, A2b, and A3 adenosine receptors (ARs).160 A1ARs are found throughout the brain and are enriched in cerebral white matter tracts. The A1ARs are expressed in brain during periods of neuronal birth, migration, and axon sprouting.161 A1ARs are expressed by neurons, microglia and oligodendrocytes.162,163 When P3 to P14 rats are treated with A1AR agonists, reductions in cerebral white matter are observed together with ventriculomegaly, and reduced myelination.164 Quantitative electron microscopy reveals reductions in total axon volume. Importantly, neonatal rats treated with A1AR agonists sustain alterations in cerebral anatomy that are strikingly similar to those observed in rats reared in chronic sublethal hypoxia.164 We also examined the brains of genetically-engineered mice that are deficient in the enzyme adenosine deaminase. These mice have circulating levels of adenosine that are 100-fold higher than control animals.165,166 In support of the notion that increased levels of endogenous adenosine induced brain injury, we observed ventriculomegaly and reduced myelination in ADA-deficient mice. Moreover, we found that deletion of A1ARs prevents hypoxia-induced ventriculomegaly and myelin loss.133 When mice expressing A1ARs are reared in 10% oxygen, reduced myelination and ventriculomegaly is seen, along with elevated brain adenosine levels. Yet, hypoxia-induced ventriculomegaly and myelination disturbances are not observed in A1AR-knockout mice. Further supporting the notion that adenosine mediated hypoxia-induced brain injury; in preliminary studies we observed that adenosine antagonist therapy, can also prevent hypoxia-induced delayed myelination and brain injury.135 Caffeine, which is a nonselective adenosine antagonist, has also been shown to reduce hypoxic–ischemic injury in neonatal mice.167 Summary PWMI continues to be the major form of brain injury in very low birth weight infants and underlies the chronic spastic motor deficits of cerebral palsy and cognitive and learning disabilities. The spectrum of PWMI ranges from the cystic necrotic lesions of PVL to myelination disturbances that coincide with regions of diffuse gliosis. Factors that predispose to PWMI include prematurity, hypoxia, ischemia, and inflammation that contribute to degeneration of the progenitors to myelin-forming oligodendrocytes. Mediators contributing to cell injury included reactive oxygen, glutamate, cytokines, and adenosine. As our understanding of PWMI pathogenesis improves, it is anticipated that new strategies for directly preventing brain injury in premature infants will evolve. References 1. Chaudhari S, Otiv M, Chitale A, et al: Pune low birth weight study– cognitive abilities and educational performance at twelve years. Indian Pediatr 41:121-128, 2004 2. Hack M, Taylor HG: Perinatal brain injury in preterm infants and later neurobehavioral function. J Am Med Assoc 284:1973-1974, 2000 3. Taylor HG, Minich NM, Klein N, et al: Longitudinal outcomes of very low birth weight: neuropsychological findings. J Int Neuropsychol Soc 10:149-163, 2004 4. Walther FJ, den Ouden AL, Verloove-Vanhorick SP: Looking back in time: Outcome of a national cohort of very preterm infants born in The Netherlands in 1983. Early Hum Dev 59:175-191, 2000 5. Wood NS, Marlow N, Costeloe K, et al: Neurologic and developmental disability after extremely preterm birth. EPICure Study Group. N Engl J Med 343:378-384, 2000 6. Yu VY: Developmental outcome of extremely preterm infants. Am J Perinatol 17:57-61, 2000 7. Fowlie P, Davis P: Prophylactic indomethacin for preterm infants: A systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed 88:F464-F466, 2003 8. Volpe JJ: Neurobiology of periventricular leukomalacia in the premature infant. Pediatr Res 50:553-562, 2001 9. Rezaie P, Dean A: Periventricular leukomalacia, inflammation and white matter lesions within the developing nervous system. Neuropathology 22:106-132, 2002 10. Kinney HC, Back SA: Human oligodendroglial development: Rela- Periventricular white matter injury 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. tionship to periventricular leukomalacia. Semin Pediatr Neurol 5:180-189, 1998 Banker B, Larroche J: Periventricular leukomalacia of infancy. A form of neonatal anoxic encephalopathy. Arch Neurol 7:386-410, 1962 DeReuck J, Chattha A, Richardson E: Pathogenesis and evolution of periventricular leukomalacia in infancy. Arch Neurol 27:229-236, 1972 Rorke LB: Pathology of Perinatal Brain Injury. New York, NY, Raven Press, 1982, pp 45-63 Leviton A, Gilles F: Acquired perinatal leukoencephalopathy. Ann Neurol 16:1-10, 1984 Haynes RL, Folkerth RD, Keefe RJ, et al: Nitrosative and oxidative injury to premyelinating oligodendrocytes in periventricular leukomalacia. J Neuropathol Exp Neurol 62:441-450, 2003 Counsell S, Allsop J, Harrison M, et al: Diffusion-weighted imaging of the brain in preterm infants with focal and diffuse white matter abnormality. Pediatrics 112:176-180, 2003 Inder TE, Andersen NJ, Spencer C, et al: White matter injury in the premature infant: A comparison between serial cranial ultrasound and MRI at term. AJNR Am J Neuroradiol 24:805-809, 2003 Miller SP, Cozzio CC, Goldstein RB, et al: Comparing the diagnosis of white matter injury in premature newborns with serial MR imaging and transfontanel ultrasonagraphy findings. AJNR Am J Neuroradiol 24:1661-1669, 2003 Dammann O, Levition A: Infection remote from the brain, neonatal white matter damage, and cerebral palsy in the preterm infant. Semin Pediatr Neurol 5:190-201, 1998 Hagberg H, Peebles D, Mallard C: Models of white matter injury: Comparison of infectious, hypoxic–ischemic, and excitotoxic insults. Ment Retard Dev Disabil Res Rev 8:30-38, 2002 Greisen G, Borch K: White matter injury in the preterm neonate: The role of perfusion. Dev Neurosci 23:209-212, 2001 Volpe JJ: Perinatal brain injury: From pathogenesis to neuroprotection. Ment Retard Dev Disabil Res Rev 7:56-64, 2001 Young RSK, Hernandez MJ, Yagel SK: Selective reduction of blood flow to white matter during hypotension in neonatal dogs: A possible mechanism of periventricular leukomalacia. Ann Neurol 12:445-448, 1982 Ando M, Takashima S, Mito T: Endotoxin, cerebral blood flow, amino acids and brain damage in young rabbits. Brain Dev 10:365-370, 1988 Nelson KB, Grether J, Dambrosia J, et al: Neonatal cytokines and cerebral palsy in very preterm infants. Pediatr Res 53:600-607, 2003 Grether J, Nelson KB, Walsh E, et al: Intrauterine exposure to infection and risk of cerebral palsy in very preterm infants. Arch Pediatr Adolesc Med 157:26-32, 2003 Takashima S, Tanaka K: Development of cerebrovascular architecture and its relationship to periventricular leukomalacia. Arch Neurol 35: 11-16, 1978 Nakamura Y, Okudera T, Hashimoto T: Vascular architecture in white matter of neonates: Its relationship to periventricular leukomalacia. J Neuropathol Exp Neurol 53:582-589, 1994 Pyrds O, Griesen G, Lou H: Heterogeneity of cerebral vasoreactivity in preterm infants supported by mechanical ventilation. J Pediatr 115: 638-645, 1989 Pyrds O: Control of cerebral circulation in the high-risk neonate. Ann Neurol 30:321-329, 1991 Menke J, Michel E, Hildebrand S: Cross-spectral analysis of cerebral autoregulation dynamics in high risk preterm infants during the perinatal period. Pediatr Res 42:690-699, 1997 Griesen G: Cerebral blood flow in preterm infants during the first week of life. Acta Paediatr Scand 75:43-51, 1986 Skov L, Pyrds O, Griesen G, et al: Estimation of cerebral venous oxygen saturation in newborn infants by near infrared spectroscopy. Pediatr Res 32:52-55, 1992 Yoxall C, Weindling A: Measurment of cerebral oxygen consumption in the human neonate by near infrared spectroscopy: Cerebral oxygen consumption increases with advancing gestational age. Pediatr Res 44:283-290, 1998 Buchvald F, Keshe K, Griesen G: Measurement of cerebral oxyhaemo- 411 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. globin saturation and jugular blood flow in term healthy newborn infants by near-infrared spectroscopy and jugular venous occlusion. Biol Neonate 75:97-103, 1999 Borch K, Greisen G: Blood flow distribution in the normal human preterm brain. Pediatr Res 43:28-33, 1998 Tsuji M, Saul J, du Plessis A, et al: Cerebral intravascular oxygenation correlates with mean arterial pressure in critically ill premature infants. Pediatrics 106:625-632, 2000 Traystman RJ, Kirsch JR, Koehler RC: Oxygen radical mechanisms of brain injury following ischemia and reperfusion. Am J Physiol 71: 1185-1195, 1991 Capani F, Loidl C, Aguirre F, et al: Changes in reactive oxygen species (ROS) production in rat brain during global perinatal asphyxia: An ESR study. Brain Res 914:204-207, 2001 Bagenholm R, Nilsson U, Gotborg C, et al: Free radicals are formed in the brain of the fetal sheep during reperfusion after cerebral ischemia. Pediatr Res 43:271-275, 1998 Tan S, Zhou F, Nielsen VG, et al: Sustained hypoxia–ischemia results in reactive nitrogen and oxygen species production and injury in the premature fetal rabbit brain. J Neuropathol Exp Neurol 57:544-553, 1998 Tan S, Zhou F, Nielsen VG, et al: Increased injury following intermittent fetal hypoxia-reoxygenation is associated with increased free radical production in fetal rabbit brain. J Neuropathol Exp Neurol 58: 972-981, 1999 Janero DR: Malondialdehyde and thiobarbituric acid-reactivity as diagnostic indices of lipid peroxidation and peroxidative tissue injury. Free Radic Biol Med 9:515-540, 1990 Hasegawa K, Yoshioka H, Sawada T, et al: Lipid peroxidation in neonatal mouse brain subjected to two different types of hypoxia. Brain Dev 13:101-103, 1991 Montine K, Quinn J, Zhang J, et al: Isoprostanes and related products of lipid peroxidation. Chem Phy Lipids 128:117-124, 2004 Mishra OP, Delivoria-Papadopoulos M: Lipid peroxidation in developing fetal guinea pig brain during normoxia and hypoxia. Brain Res Dev Brain Res 45:129-135, 1989 Back SA, Luo NL, Montine TJ, et al: Human oligodendrocyte progenitors are vulnerable in periventricular leukomalacia. Ann Neurol 52: S112, 2002 Back SA, Volpe JJ: Cellular and molecular pathogenesis of periventricular white matter injury. Ment Retard Dev Disabil Res Rev 3:96107, 1997 Mishra OP, Delivoria-Papadopoulos M: Anti-oxidant enzymes in fetal guinea pig brain during development and the effect of maternal hypoxia. Brain Res 470:173-179, 1988 Folkerth R, Haynes R, Borenstein NS, et al: Developmental lag in superoxide dismutases relative to other antioxidant enzymes in premyelinated human telencephalic white matter. J Neuropathol Exp Neurol 63:990-999, 2004 Back SA, Luo NL, Borenstein NS, et al: Late oligodendrocyte progenitors coincide with the developmental window of vulnerability for human perinatal white matter injury. J Neurosci 21:1302-1312, 2001 Back SA, Luo NL, Borenstein NS, et al: Arrested oligodendrocyte lineage progression during human cerebral white matter development: dissociation between the timing of progenitor differentiation and myelinogenesis. J Neuropathol Exp Neurol. 61:197-211, 2002 Chan PH: Reactive oxygen radicals in signalling and damage in the ischemic brain. J Cereb Blood Flow Metab 21:2-14, 2001 Back SA, Gan X-D, Li Y, et al: Maturation-dependent vulnerability of oligodendrocytes to oxidative stress-induced death caused by glutathione depletion. J Neurosci. 18:6241-6253, 1998 Fern R, Moller T: Rapid ischemic cell death in immature oligodendrocytes: A fatal glutamate release feedback loop. J Neurosci 20:34-42, 2000 Back SA, Han BH, Luo NL, et al: Selective vulnerability of late oligodendrocyte progenitors to hypoxia–ischemia. J Neurosci 22:455-463, 2002 Lin S, Rhodes P, Lei M, et al: ␣-Phenyl-n-tert-butyl-nitrone attenuates S.A. Back and S.A. Rivkees 412 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. hypoxic–ischemic white matter injury in the neonatal rat brain. Brain Res 1007:132-141, 2004 Fragoso G, Martinez-Bermudez A, Lui H-N, et al: Developmental differences in H2O2-induced oligodendrocyte cell death: Role of glutathione, mitogen-activated protein kinases and caspase 3. J Neurochem 90:392-404, 2004 Baud O, Greene A, Li J, et al: Glutathione peroxidase-catalase cooperativity is required for resistance to hydrogen peroxide by mature rat oligodendrocytes. J Neurosci 24:1531-1540, 2004 Brault S, Martinez-Bermudez A, Roberts II J, et al: Cytotoxicity of the E2-Isoprostane 152T-IsoP on oligodendrocyte progenitors. Free Radic Biol Med 37:358-366, 2004 Mronga T, Stahnke T, Goldbaum O, et al: Mitochondrial pathway is involved in hydrogen-peroxide-induced apoptotic cell death of oligodendrocytes. Glia 46:446-455, 2004 Druzhyna N, Hollensworth S, Kelley M, et al: Targeting human 8-oxoguanine glycosylase to mitochondria of oligodendroyctes protects against menadione-induced oxidative stress. Glia 42:370-378, 2003 Ness JK, Romanko MJ, Rothstein RP, et al: Perinatal hypoxia–ischemia induces apoptotic and excitotoxic death of periventricular white matter oligodendrocyte progenitors. Dev Neurosci 23:203-208, 2001 Castillo-Melendez M, Chow J, Walker D: Lipid peroxidation, caspase-3 immunoreactivity, and pyknosis in late-gestation fetal sheep brain after umbilical cord occlusion. Pediatr Res 55:864-871, 2004 Cao Y, Gunn A, Bennet L, et al: Insulin-like growth factor (IGF)-1 suppresses oligodendrocyte caspase-3 activation and increases glial proliferation after ischemia in near-term fetal sheep. J Cereb Blood Flow Metab 23:739-747, 2003 Rorke LB: Perinatal brain damage, in Adams JH, Duchen LW (eds): Greenfield’s Neuropathology. London, Edward Arnold, 1992, pp 639-709 Kinney HC, Armstrong DD: Perinatal neuropathology, in Graham D, Lantos P (eds): Greenfield’s Neuropathology. London, Arnold, 2002, pp 519-606 Nakanishi H: Microglial functions and proteases. Mol Neurobiol 27: 163-176, 2003 Gebicke-Haerter PJ: Microglia in neurodegeneration: Molecular aspects. Microsc Res Tech 54:47-58, 2001 Streit WJ: The role of microglia in brain injury. Neurotoxicology 17: 671-678, 1996 Hansson E, Ronnback L: Glial neuronal signaling in the central nervous system. FASEB J 17:341-348, 2003 Rezaie P, Male D: Colonisation of the developing human brain and spinal cord by microglia: A review. Microsc Res Tech 45:359-382, 1999 Male D, Rezaie P: Colonisation of the human central nervous system by microglia: The roles of chemokines and vascular adhesion molecules. Prog Brain Res 132:81-93, 2001 Ciccarelli R, Di Iorio P, D’Alimonte I, et al: Cultured astrocyte proliferation induced by extracellular guanosine involves endogenous adenosine and is raised by the co-presence of microglia. Glia 29:202211, 2000 Kreutzberg GW: Microglia: A sensor for pathological events in the CNS. Trends Neurosci 19:312-318, 1996 Inoue K: Microglial activation by purines and pyrimidines. Glia 40: 156-163, 2002 Nakajima K, Kohsaka S: Microglia: Activation and their significance in the central nervous system. J Biochem (Tokyo) 130:169-175, 2001 Merrill JE, Ignarro LJ, Sherman MP, et al: Microglial cell cytotoxicity of oligodendrocytes is mediated through nitric oxide. J Immunol 151: 2132-2141, 1993 Merrill JE, Murphy SP, Mitrovic B, et al: Inducible nitric oxide synthase and nitric oxide production by oligodendrocytes. J Neurosci Res 48:372-384, 1997 Mitrovic B, Ignarro LJ, Vinters HV, et al: Nitric oxide induces necrotic but not apoptotic cell death in oligodendrocytes. Neuroscience 65: 531-539, 1995 Boullerne AI, Nedelkoska L, Benjamins JA: Synergism of nitric oxide 82. 83. 84. 85. 86. 87. 88. 89. 90. 91. 92. 93. 94. 95. 96. 97. 98. 99. 100. 101. 102. 103. 104. 105. and iron in killing the transformed murine oligodendrocyte cell line N20.1. J Neurochem 72:1050-1060, 1999 Rosenberg PA, Li Y, Ali S, et al: Intracellular redox state determines whether nitric oxide is toxic or protective to rat oligodendrocytes in culture. J Neurochem 73:476-484, 1999 Lehnardt S, Lachance C, Patrizi S, et al: The toll-like receptor TLR4 is necessary for lipopolysaccharide-induced oligodendrocyte injury in the CNS. J Neurosci 22:2478-2486, 2002 Inder T, Huppi P, Warfield S, et al: Periventricular white matter injury in the premature infant is followed by reduced cerebral cortical gray matter volume at term. Ann Neurol 46:755-760, 1999 Rutherford M, Pennock J, Dubowitz L: Cranial ultrasound and magnetic resonance imaging in hypoxic–ischaemic encephalopathy: A comparison with outcome. Dev Med Child Neurol 36:813-825, 1994 Okumura A, Hayakawa F, Kato T, et al: MRI findings in patients with spastic cerebral palsy. I. Correlation with gestational age at birth. Dev Med Child Neurol 39:363-368, 1997 Reddy K, Mallard C, Guan J, et al: Maturational change in the cortical response to hypoperfusion injury in the fetal sheep. Pediatr Res 43: 674-682, 1998 McQuillen PS, Sheldon RA, Shatz CJ, et al: Selective vulnerability of subplate neurons after early neonatal hypoxia–ischemia. J Neurosci 23:3308-3315, 2003 Ment LR, Schwartz M, Makuch RW, et al: Association of chronic sublethal hypoxia with ventriculomegaly in the developing rat brain. Brain Res Dev Brain Res 111:197-203, 1998 Vexler ZS, Ferriero DM: Molecular and biochemical mechanisms of perinatal brain injury. Semin Neonatol 6:99-108, 2001 Hamrick SE, Ferriero DM: The injury response in the term newborn brain: Can we neuroprotect? Curr Opin Neurol 16:147-154, 2003 Turner CP, Pulciani D, Rivkees SA: Reduction in intracellular calcium levels induces injury in developing neurons. Exp Neurol 178:21-32, 2002 Back SA: Approaches to the cellular and molecular pathogenesis of human perinatal white matter injury, in: Choi D, Dacey Jr R, Hsu CH, Powers W (eds): Cerebrovascular Disease: Momentum at the End of the Second Millenium (21st Princeton Conference). Armonk, NY, Futura Press, 2001, pp 131-160 Selmaj K, Raine CS: Tumor necrosis factor mediates myelin and oligodendrocyte damage in vitro. Ann Neurol 23:339-346, 1988 Vartanian T, Li Y, Zhao M, et al: Interferon-␥-induced oligodendrocyte cell death: Implications for the pathogenesis of multiple sclerosis. Mol Med 1:732-743, 1995 McLaurin J, D’Souza S, Stewart J, et al: Effect of tumor necrosis factor alpha and beta on human oligodendrocytes and neurons in culture. Int J Dev Neurosci 13:369-381, 1995 Merrill JE: Effects of interleukin-1 and tumor necrosis factor-␣ on astrocytes, microglia, oligodendrocytes, and glial precursors in vitro. Dev Neurosci 13:130-137, 1991 Agresti C, D’Urso D, Levi G: Reversible inhibitory effects of interferon-␥ and tumor necrosis factor-␣ on oligodendroglial lineage cell proliferation and differentiation in vitro. Eur J Neurosci 8:1106-1116, 1996 Folkerth R, Keefe R, Haynes R, et al: Interferon-gamma expression in periventricular leukomalacia in the human brain. Brain Pathol 14: 265-274, 2004 Hill JM, Switzer RC: The regional distribution and cellular localization of iron in the rat brain. Neuroscience 11:595-603, 1984 Dwork AJ, Schon EA, Herbert J: Nonidentical distribution of transferrin and ferric iron in human brain. Neuroscience 27:333-345, 1988 Gerber MR, Connor JR: Do oligodendrocytes mediate iron regulation in the human brain? Ann Neurol 26:95-98, 1989 Connor JR, Menzies SL: Relationship of iron to oligodendrocytes and myelination. Glia 17:83-93, 1996 Connor JR, Phillips TM, Lakshman MR, et al: Regional variations in the levels of transferrin in the CNS of normal and myelin-deficient rats. J Neurochem 49:1523-1529, 1987 Connor JR, Menzies SL: Altered distribution of iron in the central Periventricular white matter injury 106. 107. 108. 109. 110. 111. 112. 113. 114. 115. 116. 117. 118. 119. 120. 121. 122. 123. 124. 125. 126. 127. nervous system of myelin deficient rats. Neuroscience 34:265-271, 1990 Roskams AJ, Connor JR: Transferrin receptor expression in myelin deficient (md) rats. J Neurosci Res 31:421-427, 1992 Yonezawa M, Back SA, Gan X, et al: Cystine deprivation induces oligodendroglial death: Rescue by free radical scavengers and by a diffusible glial factor. J Neurochem 67:566-573, 1996 Thorburne SK, Juurlink BHJ: Low glutathione and high iron govern the susceptibility of oligodendroglial precursors to oxidative stress. J Neurochem 67:1014-1022, 1996 Zaman K, Ryu H, Hall D, et al: Protection from oxidative stressinduced apoptosis in cortical neuronal cultures by iron chelators is associated with enhanced DNA binding of hypoxia-inducible factor-1 and ATF-1/CREB and increased expression of glycolytic enxymes, p21 waf1/cip1, and erythropoietin. J Neurosci 19:9821-9830, 1999 Follet PL, Rosenberg PA, Volpe JJ, et al: NBQX attenuates excitotoxic injury to the developing white matter. J Neurosci 20:9235-9241, 2000 Liu H, Giasson B, Mushynski W, et al: AMPA receptor-mediated toxicity in oligodendrocyte progenitors involves free radical generation and activation of JNK, calpain and caspase 3. J Neurochem 82:398409, 2002 Deng W, Wang H, Rosenberg PA, et al: Role of metabotropic glutamate receptors in oligodendrocyte excitotoxicity and oxidative stress. Proc Natl Acad Sci U S A 101:7751-7756, 2004 Borges K, Ohlemeyer C, Trotter J, et al: AMPA/Kainate receptor activation in murine oligodendrocyte precursor cells leads to activation of a cation conductance, calcium influx and blockade of delayed rectifying K⫹ channels. Neuroscience 63:135-149, 1994 Yoshioka A, Hardy M, Younkin DP, et al: ␣-Amino-3-hydroxy-5methyl-4-isoxazolepropionate (AMPA) receptors mediate excitotoxicity in the oligodendroglial lineage. J Neurochem 64:2442-2448, 1995 McDonald JW, Althomsons S, Hyrc K, et al: Oligodendrocytes from forebrain are highly vulnerable to AMPA/kainate receptor-mediated excitotoxicity. Nat Med 4:291-297, 1998 Sanchez-Gomez M, Matute C: AMPA and kainate receptors each mediate excitotoxicity in oligodendroglial cultures. Neurobiol Dis 6:475485, 2000 Itoh T, Beesley J, Itoh A, et al: AMPA glutamate receptor-mediated calcium signaling is transiently enhanced during development of oligodendrocytes. J Neurochem 81:390-402, 2002 Oka A, Belliveau MJ, Rosenberg PA, et al: Vulnerability of oligodendroglia to glutamate: Pharmacology, mechanisms, and prevention. J Neurosci 13:1441-1453, 1993 Bannai S, Kitamura E: Transport interaction of L-cystine and L-glutamate in human diploid fibroblasts in culture. J Biol Chem. 255:23722376, 1980 Murphy T, Miyamoto M, Sastre A, et al: Glutamate toxicity in a neuronal cell line involves inhibition of cystine transport leading to oxidative stress. Neuron 2:1547-1558, 1989 Sato H, Tamba M, Ishii T, et al: Cloning and expression of a plasma membrane cystine/glutamate exchange transporter composed of two distinct proteins. J Biol Chem 274:11455-11458, 1999 Back SA: Recent advances in human perinatal white matter injury. Prog Brain Res 132:131-147, 2001 Rezaie P, Dean A: Periventricular leukomalacia, inflammation and white matter lesions within the developing nervous system. Neuropathology 22:106-132, 2002 Avishai-Eliner S, Brunson KL, Sandman CA, et al: Stressed-out, or in (utero)? Trends Neurosci 25:518-524, 2002 Craig A, Luo NL, Beardsley DJ, et al: Quantitative analysis of perinatal rodent oligodendrocyte lineage progression and its correlation with human. Exp Neurol 181:231-240, 2003 Craig A, Luo NL, Beardsley DJ, et al: Quantitative analysis of rodent oligodendrocyte lineage progression and its correlation with human. Exp Neurol 181:231-240, 2003 Vannucci RC, Connor JR, Mauger DT, et al: Rat model of perinatal hypoxic–ischemic brain damage. J Neurosci Res 55:158-163, 1999 413 128. Marret S, Mukendi R, Gadisseux J-F, et al: Effect of ibotenate on brain development: An excitotoxic mouse model of microgyria and posthypoxic-like lesions. J Neuropathol Exp Neurol 54:358-370, 1995 129. Husson I, Mesples B, Bac P, et al: Melatonergic neuroprotection of the murine periventricular white matter against neonatal excitotoxic challenge. Ann Neurol 51:82-92, 2002 130. Gressens P, Besse L, Robberecht P, et al: Neuroprotection of the developing brain by systemic administration of vasoactive intestinal polypeptide derivatives. J Pharmacol Exp Ther 288:1207-1213, 1999 131. Dommergues M-A, Patkai J, Renauld J-C, et al: Proinflammatory cytokines and interleukin-9 exacerbate excitotoxic lesions of the newborn murine neopallium. Ann Neurol 47:54-63, 2000 132. Follett PL, Rosenberg PA, Volpe JJ, et al: NBQX attenuates excitotoxic injury in developing white matter. J Neurosci 20:9235-9241, 2000 133. Turner CP, Seli M, Ment L, et al: A1 adenosine receptors mediate hypoxia-induced ventriculomegaly. Proc Natl Acad Sci U S A 100: 11718-11722, 2003 134. Weiss J, Takizawa B, McGee A, et al: Neonatal hypoxia suppresses oligodendrocyte Nogo-A and increases axonal sprouting in a rodent model for human prematurity. Exp Neurol 189:141-149, 2004 135. Back SA, Craig A, Luo NL, et al: Adenosine-1-receptor blockade by caffeine attenuates cerebral myelination disturbances induced by chronic hypoxia in the perinatal mouse. Ann Neurol 56:S89, 2004 136. Derrick M, Luo NL, Bregman JC, et al: Preterm fetal hypoxia causes hypertonia and motor deficits in the neonatal rabbit: A model for human cerebral palsy? J Neurosci 24:24-34, 2004 137. Barlow R: The foetal sheep: Morphogenesis of the nervous system and histochemical aspects of myelination. J Comp Neurol 135:249-262, 1969 138. Cook C, Williams C, Gluckman P: Brainstem auditory evoked potential in the fetal lamb, in utero. J Dev Physiol 9:429-440, 1987 139. Cook C, Gluckman P, Johnston B, et al: The development of the somatosensory evoked potential in the unanaesthetized fetal lamb. J Dev Physiol 9:441-456, 1987 140. Back SA, Luo NL, Beardsley DJ, et al: Selective white matter injury in a fetal sheep global ishemia model of periventricular leukomalacia (PVL). Soc Neurosci Abstr, 2002 141. Jones Jr MD, Sheldon RE, Peeters LL, et al: Regulation of cerebral blood flow in the ovine fetus. Am J Physiol 235:H162-H166, 1978 142. Jones Jr MD, Traystman RJ: Cerebral oxygenation of the fetus, newborn, and adult. Semin Perinatol 8:205-216, 1984 143. Helou SM, Hudak ML, Jones MD: Cerebral blood-flow response to hypercapnia in immature fetal sheep. Am J Physiol 261:H1366H1370, 1991 144. Harris AP, Helou S, Traystman RJ, et al: Efficacy of the Cushing response in maintaining cerebral blood flow in premature and nearterm fetal sheep. Pediatr Res 43:50-56, 1998 145. Helou S, Koehler RC, Gleason CA, et al: Cerebrovascular autoregulation during fetal development in sheep. Am J Physiol 266:H1069H1074, 1994 146. Gleason CA, Hamm C, Jones Jr MD: Cerebral blood flow, oxygenation, and carbohydrate metabolism in immature fetal sheep in utero. Am J Physiol 256:R1264-R1268, 1989 147. Szymonowicz W, Walker AM, Cussen L, et al: Developmental changes in regional cerebral blood flow in fetal and newborn lambs. Am J Physiol 254:H52-H58, 1988 148. Szymonowicz W, Walker A, Yu V, et al: Regional cerebral blood flow after hemorrhagic hypotension in the preterm, near-term, and newborn lamb. Pediatr Res 28:361-366, 1990 149. Raad RA, Tan WK, Bennet L, et al: Role of the cerebrovascular and metabolic responses in the delayed phases of injury after transient cerebral ischemia in fetal sheep. Stroke 30:2735-2741, 1999 150. Mallard E, Rees S, Stringer M, et al: Effects of chronic placental insufficiency on brain development in fetal sheep. Pediatr Res 43:262-270, 1998 151. Matsuda T, Okuyama K, Cho K, et al: Induction of antenatal periventricular leukomalacia by hemorrhagic hypotension in the chronically instrumented fetal sheep. Am J Obstet Gynecol 181:725-730, 1999 152. Hagberg H, Peebles D, Mallard C: Models of white matter injury: S.A. Back and S.A. Rivkees 414 153. 154. 155. 156. 157. 158. 159. Comparison of infectious, hypoxic–ischemic, and excitotoxic insults. Ment Retard Dev Disabil Res Rev 8:30-38, 2002 Gravett M, Witkin SS, Haluska GJ, et al: An experimental model for intraamniotic infection and preterm labor in rhesus monkeys. Am J Obstet Gynecol 171:1660-1667, 1994 Sadowsky D, Haluska G, Gravett M, et al: Indomethacin blocks interleukin 1-induced myometrial contractions in pregnant rhesus monkeys. Am J Obstet Gynecol 183:173-180, 2000 Fredholm BB: Adenosine and neuroprotection. Int Rev Neurobiol 40:259-280, 1997 Ijzerman A, van Rhee AM: Modulators of adenosine uptake, release, and inactivation, in Jacobson KA, Jarvis MF (eds): Purinergic Approaches in Experimental Therapeutics. New York, NY, Wiley-Liss, 1997, pp 129-148 Olah ME, Ren H, Stiles GL: Adenosine receptors: Protein and gene structure. Arch Int Pharmacodyn Ther 329:135-150, 1995 Libert F, Van Sande J, Lefort A, et al: Cloning and functional characterization of a human A1 adenosine receptor. Biochem Biophys Res Commun 187:919-926, 1992 Trivedi BK, Bridges AJ, Bruns RF: Structure-activity relationships of adneosine A1 and A2 receptors, in Williams M (ed): Adenosine and Adenosine Receptors. Clifton, NJ, Humana, 1990, pp 57-104 160. Fredholm BB, Abbracchio MP, Burnstock G, et al: Nomenclature and classification of purinoceptors. Pharmacol Rev 46:143-156, 1994 161. Rivkees SA: The ontogeny of cardiac and neural A1 adenosine receptor expression in rats. Brain Res Dev Brain Res 89:202-213, 1995 162. Othman T, Yan H, Rivkees SA: Oligodendrocytes express functional A1 adenosine receptors that stimulate cellular migration. Glia 44:166172, 2003 163. Stevens B, Fields RD: Response of Schwann cells to action potentials in development. Science 287:2267-2271, 2000 164. Turner CP, Yan H, Schwartz M, et al: A1 adenosine receptor activation induces ventriculomegaly and white matter loss. Neuroreport 13: 1199-1204, 2002 165. Blackburn MR, Datta SK, Kellems RE: Adenosine deaminase-deficient mice generated using a two-stage genetic engineering strategy exhibit a combined immunodeficiency. J Biol Chem 273:5093-5100, 1998 166. Blackburn MR, Wakamiya M, Caskey CT, et al: Tissue-specific rescue suggests that placental adenosine deaminase is important for fetal development in mice. J Biol Chem 270:23891-23894, 1995 167. Bona E, Aden U, Fredholm BB, et al: The effect of long term caffeine treatment on hypoxic–ischemic brain damage in the neonate. Pediatr Res 38:312-318, 1995