Minimally Invasive Surgery in the Neonate: Review of Current Evidence
advertisement

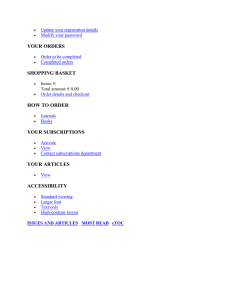
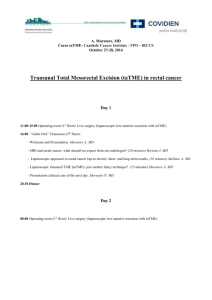
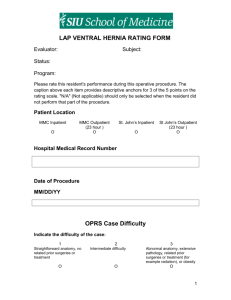
Minimally Invasive Surgery in the Neonate: Review of Current Evidence Keith E. Georgeson and Daniel J. Robertson Minimally invasive surgery has been one of the most important surgical advances in the last 15 years. The development of smaller instruments has allowed pediatric surgeons to apply this rapidly evolving technology to neonates. Congenital neonatal deformities including tracheoesophageal fistula, patent ductus arteriosus, duodenal atresia and anorectal malformations are now being managed with minimally invasive surgery. This article summarizes the status of these techniques in neonates. © 2004 Elsevier Inc. All rights reserved. he first reports of laparoscopic cholecystectomy in adults in the mid- 1980s stimulated the advance of minimally invasive general surgery (MIS), one of the most important and dramatic surgical developments of the last century. Minimally invasive techniques allow the surgeon to complete major intracavitary operations without the postoperative morbidity and pain associated with larger incisions. In the past few years, there has been an acceleration in the advancing technology and clinical sophistication of endoscopic surgery. As a result, the scope and complexity of operations that are performed via minimally invasive approaches has widened substantially. The development of MIS in the pediatric population has progressed more slowly than in adults. The most obvious problem for the development of pediatric endoscopic surgery has been instrument size and function. Instruments manufactured for adults are too large for most pediatric patients, especially neonates. Additionally, medical practitioners have often underestimated the degree of postoperative pain in neonatal and pediatric patients who are unable to articulate their specific distress. The length of incisions for open operations in neonates appear to be short, but are relatively as long as corresponding incisions in adults. It has taken the pediatric surgical community longer to ac- T From the Division of Pediatric Surgery, Children’s Hospital of Alabama, University of Alabama, Birmingham, AL. Address reprint requests to Daniel J. Robertson, MD, 1600 7th Ave S, Suite 300, Birmingham, AL 35233. © 2004 Elsevier Inc. All rights reserved. 0146-0005/04/2803-0007$30.00/0 doi:10.1053/j.semperi.2004.03.008 212 cept decreased incision size as a benefit of MIS in neonates.1 In addition, laparoscopic cholecystectomy is a relatively uncommon operation in children. No similar single procedure has propelled the advance of minimally invasive techniques in pediatric patients. With the development of smaller instruments and an understanding of both the safety and benefits of these techniques, there has been a virtual revolution in pediatric surgery over the last 5 to 10 years. Complicated neonatal problems including tracheoesophageal fistula, duodenal atresia, and pull-through for Hirschsprung’s disease can now be treated with MIS techniques. This article outlines some of the neonatal applications for endoscopic surgery and summarizes the scant but growing evidence supporting the use of minimally invasive techniques in neonates.2 Thoracoscopy Thoracoscopy provides several potential advantages over thoracotomy for resection or repair of intrathoracic neonatal abnormalities. Scoliosis develops in up to 30% of neonates after thoracotomy.3 In addition, thoracoscopy appears to be associated with decreased pain and better pulmonary mechanics postoperatively and improved cosmesis when compared to thoracotomy. For thoracoscopy to be successfully employed, single-lung ventilation via mainstem intubation is ideal for improved visualization. Insufflation with CO2 into the pleural space can also help create a larger intrathoracic working space. Neonates that have marginal pulmonary status and Seminars in Perinatology, Vol 28, No 3 (June), 2004: pp 212-220 Minimally Invasive Surgery in the Neonate poorly tolerate single-lung ventilation or an elevation in CO2 via pleural absorption may not be good candidates for these techniques. Overall, however, thoracoscopy is well tolerated in neonates and appears to offer both early and late benefits. Patent Ductus Arteriosus Ligation As neonatal care has continued to improve, more low-birth weight neonates with patent ductus arteriosus (PDA) are being cared for in the NICU setting. Multi-institutional trials have demonstrated that diuretics and indomethacin are often effective in inducing closure of the PDA, leaving surgical ligation of the PDA for failure of these medical therapies. Recent studies have reemphasized the effectiveness and the safety of surgical ligation, particularly in very low birth weight babies, who are prone to necrotizing enterocolitis and recurrence of the PDA after indomethacin therapy.4 From the time that Dr. Robert Gross first successfully ligated a PDA in 1938 until 1991, the standard operative approach to this lesion was via a posterolateral thoracotomy. In the early 1990s, both Burke5 in Boston and Laborde6 in Paris independently developed thoracoscopic techniques for interrupting the PDA. Since that time, these techniques have been used in multiple centers and in progressively smaller newborns. Burke7 in a recent experience reports on 34 neonates with an average weight of 930 g, who underwent VATS PDA ligation with no operative mortality, a 12% conversion rate to open, elimination of ductal flow in all patients documented by echocardiogram, and a 6% rate of trace ductal flow documented during subsequent follow-up echocardiography. Recurrent laryngeal nerve injury was seen in 2.9% of patients. These figures are consistent with other published literature on thoracoscopic PDA ligation and are comparable to rates of recurrence and recurrent nerve injury for open techniques. Tracheoesophageal Fistula Successful ligation and repair of tracheoesophageal fistula via a thoracoscopic approach has been accomplished in the last several years and illustrates the potential that can be achieved with minimally invasive surgery in neonates. The 213 first entirely thoracoscopic repair was reported by Lobe et al8 in 1999 and described repair of pure atresia in an 8-month-old patient. Rothenberg has subsequently reported on a series of 8 neonates with esophageal atresia and distal fistula9; Bax et al from the Netherlands also has reported a series of 8 patients.10 Several neonatal centers have successfully performed more than 20 esophageal atresia repairs.11 The procedure is completed using 3 endoscopic ports ranging in size from 3 to 5 mm in diameter. Low flow CO2 insufflation into the right hemithorax (or left if the patient has a right-sided aortic arch) is used to retract the lung. In addition to the benefits of avoiding thoracotomy, the surgeons who report on this technique cite improved exposure and visualization as well as dissection under magnification as potential advantages (Fig 1). In addition, CO2 insufflation may cause less pulmonary compromise during the operation when compared to standard mechanical retraction. Suturing the anastomosis in a small space is technically demanding. The incidence of leakage and stricture may be increased during the learning curve for this technique, but appear to be equivalent after experience is gained. Pulmonary Resection Thoracoscopic wedge resection of lung lesions has been used widely in both adults and children, but thoracoscopic lobectomy is relatively new. Neonatal lung diseases most amenable to VATS techniques include cystic congenital adenomatoid malformation (CCAM) and pulmonary sequestration. These congenital lesions are commonly diagnosed on prenatal ultrasound; they may enlarge and cause mediastinal compression and fetal hydrops; they may remain stable or they may regress in size.12 Even when these lesions regress and cannot be detected by subsequent ultrasound, they are usually apparent on postnatal CT scan of the chest.13 Sequestration and CCAMs require resection due to the risk of recurrent pulmonary infection and progressive enlargement of the pulmonary cysts leading to ventilatory compromise (Fig 2). Several reports document VATS pulmonary lobectomy in neonates and infants. Gluer et al reported on the resection of an extralobar pulmonary sequestration in a 22 day old.14 Al- 214 Georgeson and Robertson Figure 1. Thoracoscopic repair of esophageal atresia. Note the clip on the divided tracheoesophageal fistula. banese et al15 recently reported on 14 patients with prenatal diagnoses of lung lesions who underwent thoracoscopic resection between the ages of 4 and 35 months with an average operating time of 110 minutes, a postoperative hospital stay of 3 days with no serious complications and no conversions. Figure 2. Thoracoscopic resection of an intralobar pulmonary sequestration with a clear view of the extraanatomic feeding vessels prior to ligation. Diaphragmatic Hernia/Eventration Neonates can be afflicted with diaphragmatic eventration and phrenic nerve paralysis as either a result of a difficult delivery or as an iatrogenic problem after neonatal cardiac surgery. The goal of diaphragmatic plication in these patients Minimally Invasive Surgery in the Neonate is to improve respiratory mechanics to allow for bilateral lung expansion, which is critically important in neonates due to their cylindrical chest, recumbent position and small airways.16 Thoracoscopy is ideally suited for eventration, because it allows for successful plication of the diaphragm without a large abdominal wall incision, which can decrease pulmonary compliance in the early postoperative period. Several studies in adults document marked improvement of PFTs postoperatively17,18; no similar studies to date have been performed in children. From a technical standpoint, either interrupted or running sutures or endoscopic staplers have been used for plication. The authors prefer interrupted sutures. Congenital diaphragmatic hernia in the neonate is one of the most challenging problems faced by the pediatric surgeon. Mortality rates for this condition are under dispute but range from 20% to 60%. While there are a number of reports in the literature that describe repair of both Morgagni hernias and Bochdalek hernias in children and adults, MIS in neonates with life threatening Bochdalek hernias is controversial. Repair of asymptomatic CDH may be performed laparoscopically or thoracoscopically.19 Endoscopic placement of diaphragmatic patches has also been successfully performed in our hospital. Laparoscopy In order to perform laparoscopy, pneumoperitoneum using insufflation with CO2needs to be established for adequate visualization. Neonates are particularly sensitive to absorption of CO2 and can develop respiratory acidosis, which is almost always correctable by increasing the neonate’s minute ventilation. Increased intraabdominal pressure can also compromise venous return causing hypotension, and intraabdominal pressures greater than 10 mm Hg are sometimes poorly tolerated by the neonate.20 Several unique problems are encountered when performing laparoscopy in the neonate. In pediatric patients, the largest trocar is usually inserted through the umbilicus for cosmesis and to exploit an existing small umbilical hernia. Many neonates have retained umbilical stumps, and access in this age group is generally made through an umbilical fold below the umbilicus. The abdominal wall of neonates is relatively 215 thin. Techniques have been developed to secure trocars to the abdominal wall to keep them from slipping in and out when instruments are placed through them. In general, incisions and trocars between 2 and 4 mm are used in neonates. The volume of gas required for pneumoperitoneum in neonates is small and current insufflators, designed primarily for adults, deliver large volumes of gas fairly rapidly. Flow on these insufflators must be kept low, and a small intentional leak from a laparoscopy trocar is often helpful in controlling pressure overshoot. Duodenal Atresia Congenital duodenal obstruction is usually treated with duodenoduodenostomy using open methods with excellent long-term results. Only recently has MIS been applied to this condition. Unlike many neonatal bowel obstructions, which present technical problems for the laparoscopic surgeon due to the dilated bowel making visualization difficult, duodenal atresia is favorable for treatment via laparoscopy. The distal bowel is decompressed (due to the duodenal obstruction) allowing for space to identify the nature of the lesion and the performance of a successful repair. Recent reports describe successful treatment for both atresias and webs.21-23 Operating time is not significantly different between open and laparoscopic techniques. Return to feeding may be more rapid after laparoscopic duodenoduodenostomy than after its open counterpart, although patient numbers are too small to make definitive conclusions. Infusing saline through a spinal needle inserted through the abdominal wall and into the proximal jejunal lumen is used to assess the lumenal continuity through the entire small bowel. Malrotation Malrotation of the intestine can be a life-threatening surgical emergency due to the risk of midgut volvulus with subsequent infarction of the small intestine. This problem occurs most commonly in neonates, although children and adolescents have also presented with acute volvulus as the initial presentation of malrotation. Surgical treatment of malrotation was first described by Ladd in 1932 and includes detorsion of the associated volvulus, placement of the proximal 216 Georgeson and Robertson small intestine in the right side of the abdomen, placement of the colon in the left side of the abdomen, and broadening of the base of the mesentery by incising the anterior peritoneum of the mesentery. Incidental appendectomy is usually recommended due to the abnormal position of the appendix in these neonates. The spectrum of nonrotation to malrotation of the intestine varies substantially and the more narrow the base of the mesentery, the more unstable the midgut. Stability of the gut is best assessed by surgical exploration. Laparoscopy allows the surgeon to assess the exact character of the malrotation and to perform detorsion of the bowel and completion of Ladd’s procedure. Laparoscopic treatment of this problem was first published in 199524 and has subsequently been reported in roughly 50 patients ranging in age from several days to adulthood.25-29 One potential disadvantage to laparoscopic Ladd’s procedure is that postoperative adhesion formation may be less than in the open operation, leaving the bowel unstable. However, raw surfaces are left after a laparoscopic Ladd’s procedure, which usually form adhesions. There have been no published reports of midgut volvulus after laparoscopic Ladd’s procedure. Endorectal Pull-Through for Hirschsprung’s Swenson was the first to report a successful surgical correction for Hirschsprung’s disease in 1948. Since that time, several operations have been developed which differ in technical detail from Swenson’s procedure, but adhere to the basic principles he advocated. Successful repair of Hirschsprung’s disease includes resection of the distal aganglionic bowel with reanastomosis of the neorectum to the anus while sparing the anal sphincter and avoiding injury to the genitourinary tract. The operations described by Duhamel and Soave were developed to minimize anterior pelvic dissection to prevent problems with urinary continence and reproductive function. Classically, a diverting ostomy was initially performed followed by subsequent resection of the aganglionic segment. In 1980, So et al30 first reported successful primary pull-through without diverting ostomy. In most patients with Hirschsprung’s disease, primary pull-through can be performed in the neonatal period with results equivalent or superior to multi-stage procedures and with the benefit of avoiding the morbidity associated with an ostomy and secondary surgeries.31 Laparoscopy has been used to enhance the primary surgical management of this disease in several ways. Endoscopic seromuscular biopsies can be obtained from various levels in the colon which are then evaluated by frozen section to determine the level of the transition zone. The intraabdominal aganglionic colon is mobilized laparoscopically. After this mobilization, a transanal submucosal dissection is carried out to complete removal of the aganglionic colon. The transanal submucosal dissection is performed to spare nerves to both the bladder and reproductive organs and the nerves and muscular fibers of the anal sphincters. After the resection of the aganglionic segment, normally ganglionic colon is brought down just proximal to the dentate line and secured there (Fig 3). Finally, laparoscopy is also used to ensure that the pull-through segment has not been twisted on its mesentery after it is pulled through. Combined outcomes from 80 patients operated in 6 pediatric surgery centers over 5 years have been summarized by Georgeson et al.32 Of these 80 patients, only 1 required blood transfusion, blood loss averaged less than 10 mL, average operating time was 147 minutes, and time to ad lib feedings averaged 28 hours. The disease was confined to the rectosigmoid in 86% of these patients, although one patient had total colonic Hirschsprung’s disease. Almost 90% were less than 6 months of age and mean time to hospital discharge was 3.7 days after operation. Two cases were converted to open operations, 6 patients had early enterocolitis, 6 patients had chronic diarrhea, and 2 patients had anastomotic leaks. There were no anastomotic strictures, bowel obstructions, or wound complications. In summary, MIS techniques allow for treatment of Hirschsprung’s disease without laparotomy. By using laparoscopy prior to the transanal endorectal dissection, the transition zone can be gauged precisely. Long segment Hirschsprung’s disease can be recognized before the endorectal dissection so that colectomy can be based on permanent section analysis. Figure 3. (A) The aganglionic colon is mobilized laparoscopically. (B) The mucosa is cored out. (C) The aganglionic colon is removed through the anus. (D) Normally innervated colon is attached to the anus. 218 Georgeson and Robertson Anorectal Malformation Laparoscopic assisted anorectal pull-through (LAARP) for repair of high anorectal malformations has replaced the more invasive open approach in many newborn centers. While low anorectal malformations are best operated on via a perineal approach, laparoscopy allows good visualization of the deep pelvis for dissection and division of rectourethral, rectocystic or rectovaginal fistulae in high anorectal abnormalities. After using external electrostimulation to identify the proper location for the anus, the perineal dissection is initiated inside the anal sphincters. A trocar is passed inside the anal sphincter into the pelvis under laparoscopic surveillance (Fig 4). The rectal fistula is pulled down through the anal sphincters.33,34 LAARP affords excellent visualization of the pelvic anatomy in children with high anorectal anomalies and allows the operating surgeon to Figure 4. (A) The rectourethral fistula is divided laparoscopically and the pelvic floor muscles are viewed from above. (B) The external sphincter muscles are identified and a plane is developed inside the sphincters via the perineum. (C) An expandable trocar is passed from below through the sphincters using laparoscopic surveillance from above. (D) The fistulous end of the rectum is attached to the anal skin, which is tethered upward and held in position by hitch stitches. Minimally Invasive Surgery in the Neonate avoid division of the anal sphincter and pelvic floor musculature as is necessary in the posterior sagittal anorectoplasty, the usual procedure used to correct these anomalies.35 In addition, LAARP has been reported as a one-stage operation in the neonatal period, avoiding the need for a colostomy in selected patients.36 As the technique has been developed only recently, follow-up will be necessary to determine whether this minimally invasive approach ultimately improves the rate of fecal continence, which is only 25% to 30% in open approaches for high anorectal anomalies. Inguinal Hernia Repair of congenital indirect inguinal hernia is one of the most common operations performed by pediatric surgeons. The necessity of open exploration of the contralateral groin for bilateral hernia has been debated by pediatric surgeons for years. In the last decade, laparoscopic exploration of the contralateral groin for hernia, either via the existing hernia sac or via the umbilicus, has become standard practice in most centers. More recently, laparoscopic repair of inguinal hernia has been reported, allowing for exploration of both sides and repair of existing hernias all via a minimally invasive approach. Ligating the hernia sac in this manner spares the extensive dissection required to separate the spermatic cord structures from the often adherent hernia sac, and may decrease the incidence of infertility, particularly in cases of bilateral hernia. The techniques are too new to allow for long-term data regarding fertility and recurrence. Summary Minimally invasive surgery has been one of the major surgical advances in the last several decades. New technology has allowed the application of these advances to the neonate. While early data collected to this point has been based on relatively small numbers of patients, the techniques are promising.37 Potential advantages of these techniques are the development of less adhesions and scar tissue, less postoperative pain, less disruption of anatomy and function and better cosmesis. Continued technical advances in the manufacture of the smaller equip- 219 ment will allow continued advances in endoscopic neonatal surgery. References 1. Georgeson KE, Owings E: Advances in minimally invasive surgery in children. Am J Surg 180:362-364, 2000 2. Georgeson KE: Minimally invasive surgery in neonates. Semin Neonatol 8:243-248, 2003 3. Jaureguizar E, Vasquez J, Mrucia J, et al: Morbid musculoskeletal sequelae of thoracotomy for tracheoesophageal fistula. J Ped Surg 20:511-514, 1985 4. Little DC, Pratt TC, Blalock SE, et al: Patent ductus arteriosus in micropreemies and full-term infants: The relative merits of surgical ligation versus indomethacin treatment. J Ped Surg 38:492-496, 2003 5. Burke RP, Michielon G, Wernosvsky G: Video-assisted cardioscopy in congenital heart operations. Ann Thorac Surg 110:1681-1684, 1995 6. Laborde F, Noirhomme P, Karam J, et al: A new videoassisted thoracoscopic surgical technique for interruption of patent ductus arteriosus in infants and children. J Thorac Cardiovasc Surg 105:278-280, 1993 7. Burke RP, Jacobs J, Cheng W, et al: Video-assisted thoracoscopic surgery for patent ductus arteriosus in low birth weight neonates and infants. Pediatrics 104:227230, 1999 8. Lobe TE, Rothenberg SS, Waldschmidt J, et al: Thoracoscopic repair or esophageal atresia in an infant: A surgical first. Ped Endosurg Innovative Tech 3:141-148, 1999 9. Rothenberg SS: Thoracoscopic repair of tracheoesophageal fistula in newborns. J Ped Surg 37:869-872, 2002 10. Bax NM, van der Zee DC: Feasibility of thoracoscopic repair of esophageal atresia with distal fistula. J Ped Surg 37:192-196, 2002 11. Personal Communication, Bax NM, October 2003 12. Adzick NS, Harrison MR, Crombleholme TM, et al: Fetal lung lesions: Management and outcome. Am J Obstet Gynecol 179:884-889, 1998 13. Winters WD, Effmann EL, Nghiem HV, et al: Disappearing fetal lung masses: Importance of postnatal imaging studies. Ped Radiol 27:535-539, 1997 14. Mezzetti M, Dell’Agnola CA, Bedoni M, et al: Videoassisted thoracoscopic resection of pulmonary sequestration in an infant. Ann Thorac Surg 61:1836-1838, 1996 15. Albanese CT, Sydorak RM, Tsao KJ, et al: Thoracoscopic lobectomy for prenatally diagnosed lung lesions. J Ped Surg 38:553-555, 2003 16. Hong-Xu Z, D’Agostino RS, Pitlick PT, et al: Phrenic nerve injury complicating closed cardiovascular procedures for congenital heart disease. Ann Thorac Surg 39:445-449, 1985 17. Mouroux J, Padovani B, Poirier NC, et al: Technique for the repair of diaphragmatic eventration. Ann Thorac Surg 62:905-907, 1996 18. Suzumura Y, Terada Y, Sonobe M, et al: A case of unilateral diaphragmatic eventration treated by plication with thoracoscopic surgery. Chest 112:530-532, 1997 19. Arca MJ, Barnhart DC, Lelli JL, et al: Early experience with minimally invasive repair of congenital diaphrag- 220 20. 21. 22. 23. 24. 25. 26. 27. 28. Georgeson and Robertson matic hernias: results and lessons learned. J Ped Surg 38:1563-1568, 2003 Gueugniaud PY, Abisseror M, Moussa M, et al: The hemodynamic effects of pneumoperitoneum during laparoscopic surgery in healthy infants: assessment by continuous esophageal aortic blood flow echo-Doppler. Anesth Analg 86:290-293, 1998 Gluer S, Petersen C, Ure BM: Simultaneous correction of duodenal atresia due to annular pancreas and malrotation by laparoscopy. Eur J Ped Surg 12:423-425, 2002 Bax NM, Ure BM, van der Zee DC, et al: Laparoscopic duodenoduodenostomy for duodenal atresia. Surg Endosc 15:217, 2001 Rothenberg SS: Laparoscopic duodenoduodenostomy for duodenal obstruction in infants and children. J Ped Surg 27:1088-1089, 2002 van der Zee DC, Bax NM: Laparoscopic repair of acute volvulus in a neonate with malrotation. Surg Endosc 9:1123-1124, 1995 Gross E, Chen MK, Lobe TE: Laparoscopic evaluation and treatment of intestinal malrotation in infants. Surg Endosc 10:936-937, 1996 Mazziotti MV, Strasberg SM, Langer JC: Intestinal malrotation abnormalities without volvulus: The role of laparoscopy. J Am Coll Surg 185:172-176, 1997 Bass KD, Rothenberg SS, Chang JH: Laparoscopic Ladd’s procedure in infants with malrotation. J Ped Surg 33:279-281, 1998 Bax NM, van der Zee DC: Laparoscopic treatment of intestinal malrotation in children. Surg Endosc 12:13141316, 1998 29. Waldhausen JH, Sawin RS: Laparoscopic Ladd’s procedure and assessment of malrotation. J Laparoendosc Surg 6:S103-S105, 1996 30. So HB, Schwartz DL, Becker JM, et al: Endorectal “pullthrough” without preliminary colostomy in neonates with Hirschsprung’s disease. J Ped Surg 15:470-471, 1980 31. Coran AG, Teitelbaum DH: Recent advances in the management of Hirschsprung’s disease. Am J Surg 180:382387, 2000 32. Georgeson KE, Cohen RD, Hebra A, et al: Primary laparoscopic-assisted endorectal colon pull-through for Hirschsprung’s disease–A new gold standard. Ann Surg 229:678-682, 1999 33. Iwanaka T, Arai M, Kawashima H, et al: Findings of pelvic musculature and efficacy of laparoscopic muscle stimulator in laparoscopy-assisted anorectal pullthrough for high imperforate anus. Surg Endosc 17:278281, 2003 34. Yamataka A, Segawa O, Yoshida R, et al: Laparoscopic muscle electrostimulation during laparoscopy-assisted anorectal pull-through for high imperforate anus. J Ped Surg 36:1659-1661, 2001 35. deVries PA, Pena A: Posterior sagittal anorectoplasty. J Ped Surg 17:638-643, 1982 36. Georgeson KE, Inge TH, Albanese CT: Laparoscopically assisted anorectal pull-through for high imperforate anus–A new technique. J Ped Surg 35:927-931, 2000 37. Rangel SJ, Henry MC, Brindle M, et al: Small evidence for small incisions: Pediatric laparoscopy and the need for more rigorous evaluation of novel surgical therapies. J Ped Surg 38:1429-1433, 2003