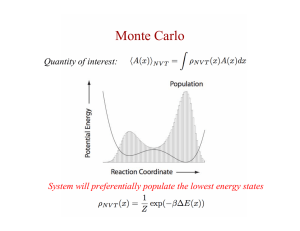
Why Monte Carlo for IMRT? Monte Carlo and IMRT ASTRO 2003
advertisement

Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU eTarget Primary Collimator Flattening Filter IC Jaw X1 Jaw X2 Objectives MLC Leaf Monte Carlo in Treatment Planning Applications: IMRT and 4D Radiation Therapy J.V. Siebers EPID MC in IMRT QA MC in IMRT optimization MC for 4D planning Virginia Commonwealth University Medical College of Virginia Hospitals Richmond, Virginia USA Mid exhale End exhale Early exhale Peak inhale Peak exhale Respiration End inhale Why Monte Carlo for IMRT? Conventional dose algorithms can be inaccurate for Small fields Regions of dose gradients (radiation disequilibrium) Heterogeneous conditions 54% within 2%,2mm Early inhale Mid inhale Dose Calculation is a two step process Incident fluence prediction Energy deposition in the patient/phantom 1 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU Conventional method for IMRT fluence prediction Why Monte Carlo for IMRT? Target Collimator Vacuum Win Flattening Filter Ion Chamber Phantom-based measurement IMRT QA often shows dose deviations Jaws Intensity Matrix MLC Profile Dose difference histogram over image Convolution Dose difference vs. DTA 54% within 2%,2mm Ψ ( x, y ) f = Ψ ( x , y ) i × I ( x , y ) MC using TPS Intensity Matrix does Not improve fluence prediction Why MC for IMRT? MC can directly transport particles through moving MLC Target Collimator Vacuum Win Flattening Filter Ion Chamber Convolution Jaws (b) (c) MLC Monte Carlo (same fluence) Effects of MLC on fluence are approximated Ignores MLC scatter, beam hardening, … Transport particles through detailed geometry of moving MLC MLC tonguegroove, leakage, scatter, and particle energy dependent effects are inherently taken into account 2 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU Why MC for IMRT? Use in of Monte Carlo in IMRT QA Patient Dose Verification MC agrees with phantom measurements Measured Calculated Obtain acceptable IMRT plan Copy plan and compute with MC Monte Carlo can accurately predict incident (b) (c) fluence Measurement and Monte Carlo 97% within 2%,2 mm Yes <3% DVH difference? No Notify planning team Print and sign DVHs and dose differences Yes Differences acceptable? Include in chart No Modify plan based on MC Typical IMRT QA result Head and Neck Comparison Study 31 plans, 28 patients Initial plans with VCU-IMRT Superposition/Convolution dose algorithm Intensity modulation via transmission compensator matrix Plans recomputed with Monte Carlo EGS4-based system Intensity modulation via simulation through moving MLC leaves Isodoses and dose-volume indices compared GTV: D98, DMean, D50, D2, EUD, and homogeneity index (HI) CTV: D95 and DMean ETC: D90 and DMean Parotids: DMean and D50 Cord/Brainstem: D2 3 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU Head and Neck Head and Neck Comparison Superposition/Convolution Monte Carlo Target structure dose comparisons Difference (DMC-DSC) DSC Dose differences typically < 5% Head and Neck Comparison Study How algorithms compare with film measurements? Results Average dose difference < 3% 4/31 plans within 3% for all dose indices 28/31 plans within 5% for all dose indices Possible Causes Fluence Prediction Heterogeneities MC better predicts fluence 4 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU Phantom differences are predictive of patient dose differences Sub-studies: Fluence prediction error (TU-FF-A1-01, …) Heterogeneity error (SU-EE-A1-01, …) If use MC to predict fluence modulation, then SC dose prediction is within 3% for all dose indices. Initial Intensity (I I(x,y)) Patient Comparison 1 7 Create Leaf Sequence Create Deliverable Intensities (ID (x,y)) 8 Compute Dose (D O) 2 Evaluate Plan Objective 3 Converged? 4 Recomputed with MCMLC Adjust I(x,y) 6 SC optimized Monte Carlo in IMRT Optimization No Yes Optimized Intensity (IO(x,y)) and Dose D O = D D 5 Why rather than just post-process recalculation? Reduce optimization convergence error How differ from normal optimization? 66 Gy Hot-Spot 57 Gy line not cover PTV Leaf trajectories are required (to transport particles through) 5 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU MC optimized to reduce OCE Optimized with MC (a) Approved plan that did not agree with MC Original SCopt Head and Neck IMRT plan Deliverable Plan SC MC of Deliverable MCopt (deliverable) (b) MC optimized plan restores target coverage MC deliverable optimization can restore original optimized plan Initial desired dose distribution was achievable, but it required different intensities / leaf sequences than predicted by SC to be achieved in the patient Conclusions MC IMRT Optimization MC and IMRT MC/IMRT researchers are developing fast methods to optimize IMRT plans using MC algorithms e- Faster MC codes Hybrid dose calculation algorithms Smoothing/denoising techniques Target Primary Collimator Flattening Filter IC Jaw X1 Jaw X2 MLC Leaf MC more accurate since it inherently includes MLC effects MC accounts for heterogeneities and fluence MC fluence predictors may improve conventional dose calculation accuracy MC optimization reduces optimization convergence errors MC is not currently used for IMRT outside of research centers, but, should be in the future EPID 6 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU Need for MC for lung dose calculation and benefits of 4D Tx previously established tumor Monte Carlo applications to four-dimensional radiotherapy Conventional Need for MC for lung dose calculation and benefits of 4D Tx previously established With 4D imaging The 4D radiotherapy process 4D CT Imaging 4D Radiotherapy Acquisition of a sequence of CT image sets over consecutive phases of a breathing cycle 4D Treatment Planning PTV PTV CTV CTV The explicit inclusion of the temporal changes in anatomy during the imaging, planning and delivery of radiotherapy Designing treatment plans on CT image sets obtained for each phase of the breathing cycle 4D Treatment Delivery Continuous delivery of the 4D treatment plans throughout the breathing cycle Conventional 4D 7 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU Aims Demonstrate a 4D Monte Carlo Method 4D Dose Calculation Method 1 Create deformation fields 2 Define anatomy on reference CT 3 Map anatomy to all CT sets 4 Create treatment plan on reference CT 5 Create treatment plan on all CT sets 6 4D Field Arrangement Combine dose distributions and display on reference CT 4D plan of single beam 6 fields Non-opposed Coplanar 6 MV Autoblock PTV + 0.5 cm 8 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU e- Monte Carlo setup Target Isodoses from 6% uncertainty calculation per beam at peak inhale Primary Collimator Flattening Filter Treatment head: EGS4/BEAM IC Jaw X 1 Jaw X2 MLC Leaf DMLC: VCUDMLC Patient: EGS4/DOSXYZ Run each for phase for 6% statistics EPID Isodoses from 6% uncertainty calculation per beam for all phases Mid exhale End exhale Early exhale Peak exhale Map dose distributions to reference (equi-time) Mid exhale Early exhale Peak inhale Peak exhale Respiration End inhale Peak inhale Respiration End inhale Mid exhale Early inhale Mid inhale Early inhale Mid inhale 9 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU Isodoses from all phases deformed to peak inhale 6% uncertainty beam Mid exhale PTV DVHs Peak exhale Respiration End inhale Combined Individual phases 100 σ=0 σ=2 σ=4 σ=8 σ=16 Volume (%) 80 60 40 Effect of statistical uncertainty on plans 20 End exhale Early exhale Peak inhale Combined 8 phases Mid inhale Early inhale Conclusion Advantages of Monte Carlo dose calc for 4D radiotherapy (1) higher accuracy for calculation in electronic disequilibrium conditions such as those encountered during lung radiotherapy (2) if deformable image registration is used, the calculation time for Monte Carlo is independent of the number of 3D CT image sets constituting a 4D CT (same time for 4D and 3D calculation) 0 0 1000 2000 3000 4000 5000 6000 7000 Dose (cGy) 10 Monte Carlo and IMRT ASTRO 2003 Jeffrey V. Siebers, VCU Acknowledgements / Contributors Paul Keall Ivaylo Mihaylov Weidong Li Iwan Kawrakow Radhe Mohan S. Joshi 11