USING CONCLUSION, ANALYSIS AND EVIDENCE DIAGRAMS TO SUPPORT Nick Chozos
advertisement

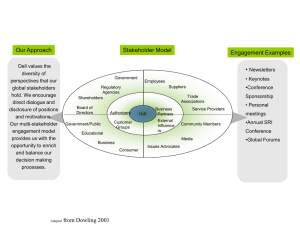
USING CONCLUSION, ANALYSIS AND EVIDENCE DIAGRAMS TO SUPPORT STAKEHOLDER ANALYSIS IN ACCIDENT REPORTS Nick Chozos Glasgow Accident Analysis Group Department of Computing Science University of Glasgow 1. Short Summary Accident reports describe the reasons for a system failure. In many cases, problematic software has been identified as a cause of accidents in accident reports. Although the technical nature of a software failure is identifiable through available techniques, the subsequent organizational and managerial issues that lead to the software failures are an abstract, complex and unquantifiable problem to consider. This paper uses a case study (SIT, 2000) in order to examine the organizational and political dimensions of the causes of an accident resulting from a software failure, and suggests ways to reason about them from a systems perspective. 2. Rationale From the 1st of January, 2000 untill the 20th of May, 2000, 158 pregnant women were screened incorrectly for the risk of giving birth to a child with Downs Syndrome, due to a software malfunction in the Immunology Department of the Sheffield Northern General Hospital. In order to investigate this event, a formal inquiry was conducted. The inquiry team characterise this incident as: "...an intricate tale with its roots going back to the late eighties. From early on events occurred, things were done and decisions were made which had a material bearing on the failure of the Downs Screening software at the Northern General to perform correctly for a period from 1st January 2000." (SIT, 2000, p. 76). The inquiry team argued that the software failure was mainly a result of organizational and managerial decisions and actions taken during the development and use of the software system. As we shall see, organizational problems not only contributed to the failure of the software, but also allowed it to produce false results for a period of over four months. In general, although the technical faults of a software component can be traceable, for instance through techniques such as software fault trees (Leveson et al., 1991), it is challenging to discuss the further organizational and systemic problems that lead to these technical faults taking place, and, most importantly, going undetected and unreported throughout the lifecycle of the development and use of the application (Johnson, 2002). 3. Theoretical background In this paper, we have used two techniques. Stakeholder Analysis, and Conclusion, Analysis and Evidence Diagrams. They are both briefly discussed in this section. 3.1 Stakeholder Analysis Stakeholder analysis originates from the business and management science. However, since its origins, it has been applied in a number of different areas, such as marketing, production (Carroll, 1989), finance, accounting, and information systems’ development (Pouloudi and Whitley, 1997). There are various definitions of what a ‘Stakeholder’ is (Barrett, 2001; Papazafeiropoulou et al., 2001). Freeman (1984, p. 46) defined a stakeholder within an organization as “any group or individual who can affect or is affected by the achievement of an organization’s objectives”. Another approach, provided by Clarkson (1995), describes stakeholders as: “persons or groups that have, or claim, ownership, rights, or interests in a corporation and its activities, past, present, or future. Such claimed rights or interests are the result of transactions with, or actions taken by, the corporation, and may be legal or moral, individual or collective” (p. 106). 1 The approach overall examines social relationships in organizations. Issues such as personal interests, politics and power among stakeholders can also create or promote instability within systems and thus affect the development and use of an information system, especially in complex contexts like healthcare (Atkinson et al., 2001). In this sense, their identification and analysis is an imperative task. Stakeholder theory has three main aspects (Donaldson and Preston, 1995): 1) The descriptive aspect of stakeholder theory concerns the identification, description and possibly explanation of characteristics and behaviours of an organization. 2) The instrumental aspect considers the identification of internal and external organizational connections. 3) The normative aspect, where the theory attempts to elaborate on the function of the organization, and identify various moral and ethical issues that stem from the interconnections within the organizational network. Ethical issues, as stated by Key (1999), are not considered in the traditional philosophical sense; rather, their identification aims at measuring the “ ‘fit’ for utilitarianism” (p. 320), or, bringing to light the necessary trade-offs that need to be made between stakeholders’ goals and the organization’s goals. 3.1.1 Stakeholder Analysis In Information Systems Development Stakeholder analysis has been identified in literature as a tool to facilitate information systems development, by being integrated with development approaches such as Soft Systems Development Methodology (Vidgen, 1997), Soft Systems and Information Technology Methodology, Participative Simulation Modelling (Atkinson et al, 2001). It has been suggested as a tool to study various parameters of development projects’ success or failure, such as level of commitment, attitudes and expectations of various information systems stakeholders (Pouloudi, 1999). 3.2 Conclusion, Analysis and Evidence Diagrams Conclusion, Analysis and Evidence (CAE) diagrams are graphs. The roots represent individual conclusions from an accident report. Lines of analysis that are connected to items of evidence support these. Each item of evidence either weakens or strengthens a line of analysis. CAE Diagrams can help to reason about the conclusions against the evidence provided (Johnson, 2001). Analysis1.1 Evidence1.1.1 Evidence1.1.2 Conclusion1 Analysis1.2 Evidence1.2.1 Evidence1.2.2 Analysis1.3 Evidence1.3.1 Evidence1.3.2 Figure 1: Example CAE Diagram 4. Methodology As mentioned, our aim is to further investigate the findings of the inquiry, in order to understand the organizational and political dimensions of the software failure, and consider an approach to deal with them from a systems’ design perspective. In order to do so, we have used stakeholder analysis and CAE Diagrams. More specifically, we have decided on one important conclusion drawn by the inquiry team, and produced the CAE Diagram for it. In the text corresponding to the findings of the CAE diagram, there is a number of stakeholders mentioned. Therefore, the CAE Diagram has helped in identifying and focusing our analysis on the 2 specific persons and organizations that were important to the specific conclusion about the incident, thus filtering from the abundance of people that are mentioned throughout the report. According to Turner (1978), organizations are vulnerable to socio-technical accidents. Disasters arise from an interaction of the human and organizational arrangements of the socio-technical systems set up to manage complex and ill-structured risk problems (Pidgeon, 1997). Hence, the purpose of stakeholder analysis in this case, is to discuss people’s roles, perceptions and relationships, in order to measure the socio-political context of the specific system’s failure that is reflected in the conclusion the CAE diagram has elaborated upon. 5. Case Study: The Downs Syndrome Screening Software Failure in the Sheffield Northern General Hospital The Downs Syndrome Screening Software Failure incident took place in the Immunology Department of the Sheffield Northern General Hospital. There, clinicians were using a software program to calculate the risk factor of pregnant women giving birth to children with the Downs Syndrome. The system had faced a number of problems through the 12 years of its life. In particular, it is wasn’t Y2K compliant, although some actions had been taken to assure its safety against the bug, the result was 158 women screened wrongly as being at low risk, where in fact they were in the high-risk category. Out of the 158 wrongly screened women, four Down' s syndrome pregnancies went undetected. Two of the women later gave birth to babies with the Down' s syndrome, while two other women terminated their pregnancies (BBC, 2000). Following this incident, a formal inquiry was conducted, in order to identify the reason behind the failure, and to make recommendations for the improvement of the system’s safety. 5.1 The Downs Syndrome Screening Process The Department of Immunology at the Northern General Hospital provides the Downs Screening service for GPs in Sheffield and surrounding areas and ten NHS Trusts and hospitals. The process of Downs Screening is a complex multidisciplinary process involving obstetricians, radiologists and the diagnostic laboratory. Several blood tests are taken at 15 – 17 weeks which are sent to the laboratory for analysis. Calculations are then used to assess the risk of the foetus being affected by Downs syndrome. These start with the age-related risk which is derived from known incidence of pregnancies affected by Downs syndrome based on maternal age. This risk is modified using a likelihood ratio of the presence of an affected foetus derived from the concentrations of the markers to provide the final risk value. The calculation relies critically on accurate estimation of the projected maternal age at delivery which, in turn, is based on the ultrasound measurements of foetal age and the date of birth of the mother. The PathLAN software makes the necessary calculations to produce the final likelihood ratio, and the results are then passed on the obstetrician who will suggest a more definite diagnostic procedure to women that are assessed as being at high-risk. 5.2 Regarding the Software Development Downs Screening had begun in Sheffield within the Immunology Department at the Royal Hallamshire Hospital in 1988 under the direction of a Dr A, as mentioned in the report. The software used by the Sheffield Northern General NHS Trust to calculate the risk of foetus being affected by Downs Syndrome, was written by an external consultant and paid for from Dr A’s research funds. The software was based on an established algorithm. It was written in GWBasic operated on a dedicated PC. Between 1988 and January 2000, the algorithm has been used in different pieces of software, the software had undergone changes, had been moved between two hospitals, had been set up on different operating systems, and had been maintained either in-house by people with self-acquired IT skills, or external consultants, with self- acquired IT skills (SIT, 2000, p. 76). 5.3 The Inquiry Team Report 3 The inquiry team, made up by medical experts and a solicitor, who also sought the advice of computing experts, performed a formal inquiry that lasted over five months. The overall conclusion is that organizational factors led to the software failure in the Sheffield Great Northern Hospital (SIT, 2000, p. 77). The report covers facts spanning twelve years, from when the software was originally developed, till the day where patients were notified of the problem. The document of 120 pages mainly discusses managerial decisions that were made, the people involved, their actions, and the affect those decisions and actions had on the software. 5.4 Conclusion, Analysis and Evidence Diagram The conclusion we have chosen to examine is the following: C1: Nobody therefore had a means of knowing, or even of acquiring a feel, whether an individual result was unusual (SIT, 2000, p. 77). Our aim is to discuss why the error went undetected for a period of 4 months, and this conclusion is deemed as one of the main reasons why, according to the inquiry team. In figure 2, the CAE diagram for conclusion C1 is depicted, and then its components are presented1. C1: Nobody therefore had a means of knowing, or even of acquiring a feel, whether an individual result was unusual (p. 77). A2: To the Systems Managers, to Mr W and to the technical staff operating the software daily, the algorithm was like a black box: information was fed in and a result was generated. (p. 77) A1: Only Dr. A understood the algorithm. (p. 77) E1 E2.2 E2.1 A3: There was no error-trapping (rewording p. 77) E2.3 E3 Figure 2: CAE Diagram Throughout the analysis and evidence components of the CAE Diagram, a number of stakeholders were identified. In the following section, they are presented and discussed. 5.5 Stakeholder Analysis The three aspects of stakeholder theory, as presented in section 3.2 were applied with regard to the positions, views and relationships of the stakeholders identified in the previous section. 5.5.1 The Descriptive Aspect: Stakeholder Identification In brief, the stakeholders identified in the CAE diagram in 5.3 are: (Immunology Dept., Sheffield Hospital) Dr A, Dr B, Mr R, Mr K, Mr L, a Liaison sister, lab staff and clinical staff and (Hartlepool) Mr W, as well as a Mid wife Coordinator in another hospital. In table 12, some of the stakeholders are presented, in terms of their roles, interests, perceptions and relation to the PathLAN. Stake holder Dr A Dr B 1 2 Responsibility HoD until Dec 1999. In charge of PRU, NEQAS and PQA Limited. Also holds a post in Sheffield University. HoD after Dec 1999 Influence on the System Relationship to the Software Perceptions, views, concerns Very High Original designer, only one that understands the algorithm Highly Supportive, and confident that the software is safe High No direct relation Beginning of May 2000, stressed concerns about logs not being Due to space restrictions, figure 2 is not discussed Due to space restrictions, table 2 is not fully presented 4 Mr R Retired in Dec. 1999 Very High Technical Manager Laboratory Manager maintained (p. 70) Had stressed concerns about Y2K in ’96 (p. 46). Mr K Computer Systems manager Laboratory Manager after Mr R’s retirement High Following Mr R’s retirement, shared Mr R’s responsibilities with Mr L, although the role ‘Computer Systems manager’ had cessed. Was seeking assurances by Hartlepool and received them (p. 54). Hartle pool Maintenance and support at SGN’s request Very High Maintained the software, suggested PathLan, only other hospital that used it. Stopped using it a year prior to the accident. Hartlepool was assured PathLan is Y2K compliant, and no other bugs resided in the code (p. 65). Laboratory IT Manager at Hartlepool, subcontracted to Great Northern High Technical Support Has stressed concerns about Y2K compliance (p. 65) Nurses and Doctors Medium Mr W Clinical and Lab Staff Users, Keep Log files after Jan Confident in the 2000 systems’ success (p. 77) Table 1: Stakeholder Identification 5.5.2 The Instrumental Aspect: Stakeholder Relationships The instrumental aspect of stakeholder analysis considers the identification of internal and external connections of stakeholders and stakeholder groups. The relationships of stakeholders discussed in the previous section, are depicted in figure 33. Dr. B Dr A Mr W algorithm MR R Mr M Mid Wife Coordinator Clinical Staff PathLan Hartlepool Trust Immunology Department, Sheffield Northern General Hospital Other Hospital Figure 3: Stakeholder Relationships 5.5.3 The Normative Aspect: Discussing Ethical Issues The normative aspect of stakeholder analysis revolves around the discussion on ethical issues. It has been suggested that moral issues can be identified by studying stakeholder relationships (Kujala, 2001). According to ethical reasoning, issues of morality appear whenever a person (or an ‘actant’- or a stakeholder) is confronted with a dilemma, and one’s decision has a consequent affect on others (Artz, 1994). The identification of points where a stakeholder was faced with one or more dilemmas, and the decisions made (and not made) can potentially tell us a lot about what happened, or what can happen, as making a wrong decision when faced with a dilemma, could well be part of the causes of the system’s failure. 3 This is still work in progress, and findings are not complete 5 A problem with ethical discussion in the field of computing is that it is often very difficult to predict consequences due to the complexity that characterises computerized information systems, and even more difficult to determine a link between action and consequence, before something happens (Artz, 1994). However, by examining the incident with hindsight, we are already aware of points were a ‘wrong’ decision was made. Therefore, rather than studying all stakeholder relationships, the discussion on stakeholder relationships in this case focuses on examining how a specific decision which we can determine as eventually critical according to its consequences relates to various stakeholders, in terms of how it was caused and what its affects were to other people. As an example, we can consider the following: There are five incidents mentioned in the report were stakeholders, mainly users (Mid-wife coordinator, Liaison Sister) were raising concerns to people in the Immunology Dept. (Mr M, Dr B, Mr K), however, no actions were taken. It is therefore important to study the reasons why the decision not to follow up on concerns was taken by people responsible. 5.5.4 Using the Findings of Stakeholder Analysis Stakeholder analysis has been used in the information systems area extensively for assisting in the requirements capture (Atkinson et al, 2001). It is known for being applied along with Soft Systems Development Methodology (SSDM), and other ‘soft’ approaches, such as Soft Information Systems and Technology Methodology (SISTeM) and Participative Simulation Modelling. For instance, SSDM is a problem-based development approach- it is used to bring about improvement in areas of social concern (Lehaney and Paul, 1996). Stakeholder Analysis is used to ‘shed light’ on issues within an organization that can be an obstacle to an information system development project (Pouloudi, 1999). Currently, we are considering the use of Soft Systems Models in order to model the problems that are identified in the findings of stakeholder analysis in this paper. 6. Discussion The incident was the ending of a story lasting over a decade. Although the obvious cause was the incompliance of the software to Y2K, identifying why this happened has taken the inquiry team five months and 120 pages, discussing facts, people and their decisions and actions taken over 12 years. The technical part of the failure is deemed as obvious, and once concerns finally reached the people responsible, it took 37 minutes to spot and fix (SIT, 2000, p. 78). However, the organizational, political and ethical issues behind the development and use of the software program are not as straightforward. Stakeholder analysis is a tool that has primarily been used during the analysis stage of information systems’ development. It has been suggested as a tool to study various parameters of development projects’ success or failure, such as level of commitment, attitudes and expectations of various information systems stakeholders (Pouloudi, 1999). Although stakeholder analysis has not been used in accident analysis, here we have applied it in order to produce a ‘rich picture’ regarding one aspect of the software failure. One conclusion drawn by the Inquiry team, and all the corresponding information was initially selected from the report using CAE diagrams, and it was then analysed with stakeholder analysis. 6.1 Ideas for Collaboration The purpose of this paper is to present stakeholder analysis as a tool that can provide with valuable insights about social and political characteristics of an adopting organization during a software development project, although it could be used in accident analysis as well. The organizational decisions and actions that contributed significantly to this software failure, and the political context within which they were formulated are the issues that stakeholder analysis opts to measure during a development project, before they determine its outcome. However, its integration with design tools and techniques, such as Soft Systems Development Methodology is necessary in order to utilise stakeholder analysis’ findings, and facilitate an effective development approach. Therefore, once the analysis of this case study is concluded, it will be interesting to consider design methods that can address the social problems that had a great impact on the outcome of this information system. Finally, we are going to apply stakeholder analysis in a similar system made up by various medical centres and a hospital here in Glasgow, in order to contrast some of the issues discussed in this 6 paper in a ‘real’ case. Again, the three aspects of stakeholder analysis should be integrated with design techniques to utilise its findings. 7 7. References Adelakum O., and Jennex E. M. (2002). Stakeholder Process Approach to Information Systems Evaluation. Americas Conference on Information Systems 2002. [available at pal.lternet.edu/lter/biblio/ finalms/jennex_AMCIS-2002-final-submital1.rtf] Artz, J. (1994) Virtue vs. Utility: Alternative Foundations of Computer Ethics. Proceedings of the Ethics in the Computer Age Conference. Gatlinburg, Tenn. November 11-13, 1994. Atkinson C. J. , Eldabi T., Paul R. J. and Pouloudi A (2001). Integrated Approaches to Health Informatics Research and Development. Logistics Information Management, 15 (2), pp. 138-152. Barrett, M. (2001). A Stakeholder Approach to Responsiveness and Accountability in Non-Profit Organizations. Social Policy Journal of New Zealand, 17, pp. 37-51. BBC News (2001). Millennium Bug Blamed for Test Errors. [Internet: http://news.bbc.co.uk/1/hi/health/1541557.stm (Last accessed: 2 November, 2004). Available at] Clarkson, M.B.E. (1995). A Stakeholder Framework for Analysing and Evaluating Corporate Social Performance. Academy of Management Review, 20(1), 92-117. Freeman, R.E. 1984. Strategic Management: A Stakeholder Approach. Boston: Pitman. Johnson, C. W. (2000). Viewpoints and Bias in Accident and Incident Reporting. Foresight and Precaution: Proceedings of European Safety and Reliability Conference ESREL 2000, Eds. M.P. Cottam, D.W. Harvey, R.P. Pape and J. Tait, Balkema, Rotterdam, The Netherlands, pp. 1395-1402 Johnson, C. W. (2001). The London Ambulance Service, Computer Aided Despatch System: A Case Study in the Integration of Accident Reports and the Constructive Design of Safety-Critical Computer Systems, Reliability Engineering and Systems Safety, 71 (3), pp. 311- 326. Johnson, C. W. (2002). Forensic Software Engineering: Are Software Failures Symptomatic of Systemic Problems? , Elsevier's Safety Science, One of the `Best Papers' from SAFECOMP 2000, 40 (9), pp. 835847. Key, S. (1999). Toward a New Theory of the Firm: A Critique of Stakeholder “Theory”. Management Decision, 37 (4), pp. 317-28. Kujala, J. (2001). Analysing Moral Issues in Stakeholder Relations. Business Ethics: A European Review, 10 (3), pp. 233-247. Lehaney, B. and Paul R. J. (1996) Soft Systems Methodology and Simulation Modelling. Proceedings on the 1996 Winter Simulation Conference, 1996, pp. 693-700 Leveson N.G., Cha S.S. and Shimeall T.J. (1991), Safety Verification of Ada Programs using Software Fault Trees, IEEE Software, 8(7), pp. 48-59. Papazafeiropoulou, A., Pouloudi, A. and Currie, W.L. (2001). Applying the Stakeholder Concept to Electronic Commerce: Extending Previous Research to Guide Government Policy Makers, Proceedings of the 34th Hawaii International Conference on System Sciences. Pidgeon, N.F. (1997). The limits to safety? Culture, politics, learning and man-made disasters, Journal of Contingencies and Crisis Management, 5(1), 1-14. 8 Pouloudi A. and Whitley E.A. (1997). Stakeholder identification in inter-organizational systems: Gaining insights for drug use management systems. European journal of information systems 6(1), pp. 1-14. Pouloudi, A (1999). Aspects of the Stakeholder Concept and their Implications for Information Systems Development. Proceedings of the 32nd Hawaii International Conference on System Sciences.pp. 1-17. Pouloudi A. and Whitley E. A. (2000) Representing human and non-human stakeholders: On speaking with authority. In Organizational and social perspectives on information technology (Baskerville Richard, Jan Stage and Janice I De Gross eds.), pp. 339-354, Kluwer, Aalborg, Denmark. Sheffield Inquiry Team (2000). Report of the Inquiry into the Computer Software Error in Downs Syndrome Screening. [Available at: http://www.nhsetrent.gov.uk/press/nghreport.htm] (Last accessed: 2 November, 2004). Smith (2002). Relationship between Quality, Safety and Organisational Behaviour, Quality and Safety in Health Care. 11, pp. 98-100 Turner, B. A. (1978). Man Made Disasters. Wykeham Science Press, London. Vidgen, R. (1997). Stakeholders, Soft Systems and Technology: Separation and Mediation in the Analysis of Information System Requirements. Information Systems Journal (7), pp. 21-46. 9