The phantom portion of the American College of Radiology ACR Computed Tomography CT
advertisement

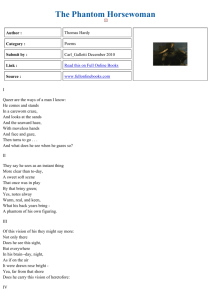
The phantom portion of the American College of Radiology „ACR… Computed Tomography „CT… accreditation program: Practical tips, artifact examples, and pitfalls to avoida… Cynthia H. McColloughb) and Michael R. Bruesewitz Department of Radiology, Mayo Clinic College of Medicine, Rochester, Minnesota 55905 Michael F. McNitt-Gray Department of Radiological Sciences, UCLA School of Medicine, Los Angeles, California 90095 Krista Bush Accreditation and Standards, American College of Radiology, Reston, Virginia 20191 Thomas Ruckdeschel Alliance Medical Physics, Alpharetta, Georgia 30004 J. Thomas Payne Radiation Oncology Department, Abbott Northwestern Hospital, Minneapolis, Minnesota 55407 James A. Brink Yale-New Haven Hospital, New Haven, Connecticut 06520 Robert K. Zeman George Washington University Medical Center, Washington, DC 20037 共Received 13 March 2004; revised 17 May 2004; accepted for publication 18 May 2004; published 19 August 2004兲 The ACR CT accreditation program, begun in 2002, requires the submission of approximately 20 images, several completed data sheets and printouts of three Excel worksheets. The procedure manual is very detailed, yet participants unfamiliar with the program or having minimal CT experience have needed to redo aspects of their submission, or in some cases do not receive accreditation, due to mistakes made by the physicist. This review of the phantom portion of the ACR CT accreditation program supplements the ACR provided instructions with additional photos of phantom setup, region-of-interest 共ROI兲, and image placement on the film sheets, and examples of completed portions of actual 共but anonymous兲 submissions. Common mistakes, as well as uncommon but interesting images, are shown and explanations are given as to what could have been done to avoid the problem. Additionally, a review of CT dose measurement techniques and calculations will enable the physicist to better assist sites where typical exam doses are above the ACR reference values. © 2004 American Association of Physicists in Medicine. 关DOI: 10.1118/1.1769632兴 Key words: ACR accreditation, ACR CT phantom, CT image quality, CT radiation dosimetry, CTDI I. INTRODUCTION The ACR CT accreditation program, begun in 2002, requires the submission of approximately 20 images, several completed data sheets, and printouts of three Excel worksheets. As part of the accreditation program materials, a detailed procedure manual is provided to assist the medical physicist in performing the required scanning, measurements, calculations, and documentation 共through submission of films兲. Still, some participants have needed to redo aspects of their submission, or in some cases do not receive accreditation, due to mistakes made in the submitted materials In the spirit of the ACR accreditation program, which is meant to be primarily educational in nature, this review supplements the ACR-provided instructions with additional photos of phantom setup, region-of-interest 共ROI兲 placement, and examples from actual 共but anonymous兲 submissions. Common mistakes, as well as uncommon but interest2423 Med. Phys. 31 „9…, September 2004 ing images, are included and explanations given as to the source of the problem. Finally, we review the CT dose measurement techniques and calculations to enable the physicist to better assist sites whose typical exam doses are above the ACR reference values. This review is organized by the various performance tests included in the submission process. For all tests, an example of an acceptable test result is included. II. ACR CT ACCREDITATION PHANTOM The ACR CT accreditation phantom has been designed to examine a broad range of image quality parameters. These include: • positioning accuracy; • CT No. accuracy; • slice width; 0094-2405Õ2004Õ31„9…Õ2423Õ20Õ$22.00 © 2004 Am. Assoc. Phys. Med. 2423 2424 McCollough et al.: Phantom portion of the ACR CT accreditation program 2424 FIG. 1. 共a兲 Diagram of the four modules of the ACR CT accreditation phantom. 共b兲 Photograph of a properly aligned phantom. 共c兲 Centering left to right on both the phantom and the phantom base 共optional兲 substantially simplifies the alignment process. 共d兲 Top view of a properly aligned phantom. 共e兲 Side view of a properly aligned phantom. The white Teflon rings on the optional phantom base may cause streak artifacts and should be moved away from the central portions of each module, which are indicated by the four white lines circumscribing the phantom. • • • • low contrast resolution; high contrast 共spatial兲 resolution; CT number uniformity; and image noise. The ACR CT accreditation phantom 共model 464, Gammex-RMI, Middleton, WI兲 is a solid phantom containing four modules, and is constructed primarily from a waterMedical Physics, Vol. 31, No. 9, September 2004 equivalent material 关Fig. 1共a兲兴. Each module is 4 cm in depth and 20 cm in diameter. There are external alignment markings on EACH module to allow centering of the phantom in the axial (z axis, cranial/caudal兲, coronal (y axis, anterior/ posterior兲, and sagittal (x axis, left/right兲 directions. There are also ‘‘HEAD,’’ ‘‘FOOT,’’ and ‘‘TOP’’ markings on the phantom to assist with alignment. An optional phantom support base may be purchased to assist in phantom alignment. 2425 McCollough et al.: Phantom portion of the ACR CT accreditation program 2425 TABLE I. Typical image acquisition technical parameters. kVp mA Time per rotation 共s兲 Scan FOV 共cm or name兲a Display FOV 共cm兲a Reconstruction algorithm Axial (A) or helical (H) Z-axis collimation (T, in mm兲b No. of data channels used b (N) A: Table increment 共mm兲 or H: Table speed 共mm/rot兲 (I) b Pitchc Reconstructed scan width 共mm兲 Reconstructed scan interval 共mm兲 Dose reduction technique共s兲d Adult head 共cerebrum portion兲 High resolution chest Adult abdomen Pediatric abdomen 共5 y.o.兲 120 170 2 Head 共25 cm兲 25 Std A 2.5 4 10 140 120 0.8 Large 共50 cm兲 38 Bone A 1.25 1 10 120 240 0.8 Large 共50 cm兲 38 Std H 3.75 4 11.25 120 110 0.8 Large 共50 cm兲 30 Std H 2.5 4 15 ¯ 5 5 ¯ ¯ 1.25 10 ¯ 0.75 共HQ兲 5 5 mA modulation 1.5 共HS兲 5 5 mA modulation a FOV⫽field of view z-axis collimation (T)⫽the width of the tomographic section along the z-axis imaged by one data channel. In multidetector row 共multislice兲 CT scanners, several detector elements may be grouped together to form one data channel. Number of data channels (N)⫽the number of tomographic sections imaged in a single axial scan. Maximum number of data channels (N max)⫽the maximum number of tomographic sections for a single axial scan. Increment (I)⫽the table increment per axial scan or the table increment per rotation of the x-ray tube in a helical scan. c Applied to helical scanning. Compute pitch according to the IEC definition: Pitch⫽table speed (mm/rotation)/N•T (mm)⫽I/N•T. For some scanners, this computed value might differ from the value given by the manufacturer. d If selectable, list selection, otherwise leave blank. Example: mA modulation based on patient attenuation. b The Appendix contains a brief description of each module contained within the ACR CT accreditation phantom, and includes a cross-sectional diagram of each module which shows the various test objects contained within each module. Figures 1共b兲–1共e兲 show a phantom that has been properly aligned with the scanner patient positioning lights. A. Table I of site scanning data form A critical element of the submission process is the completion of Table I of the site scanning data form—the description of the site’s scanning protocols. The acquisition parameters reported in Table I should be representative of the scan protocols used for the site’s routine clinical scans. These parameters will be used for scanning the image quality and dose phantoms and should be consistent with the acquisition parameters used for the clinical exams submitted as part of the accreditation process. Table I refers to the following routine examinations. 共1兲 Adult head: Head CT 共for headaches or to exclude neoplasm, brain CT, top of the head兲. 共2兲 High resolution chest: High resolution chest 共HRC兲 CT for evaluation of diffuse lung disease. 共3兲 Adult abdomen: Abdomen CT 共for detection of possible liver metastases or lymphoma兲. 共4兲 Pediatric abdomen: Pediatric abdomen CT 共for blunt trauma, acute abdominal pain, or infection兲. Assume a 5-year-old, patient. The following example shows a correct completion of Table I for a four-row multidetector row scanner 共Light Medical Physics, Vol. 31, No. 9, September 2004 Speed QX/i, General Electric Medical Systems, Milwaukee, WI兲. 1. Common Table I errors The most common error observed in the completion of Table I occurs for multidetector-row CT systems, where the Z-axis collimation (T, as defined earlier兲 is often confused with the reconstructed scan width. For single-slice CT scanners, the Z-axis collimation and reconstructed slice width are the same. However, with multislice CT scanners, these parameters often have different values. The Z-axis collimation 共also referred to as detector collimation兲 is chosen prospectively 共prior to scan acquisition兲. It determines the appropriate x-ray beam collimation and, hence, is a critical parameter for dose measurements. For the example of the four-detector row CT system described in Table I, a 5-mm-thick image is reconstructed from the projection data acquired by the fourdetector rows, each one of those rows having a Z-axis width of 3.75 mm. Hence, many physicists incorrectly report the detector collimation as 5 mm 共instead of the correct value of 3.75 mm兲. Similarly, the number of data channels used (N, as defined earlier兲 is an important acquisition parameter. Knowledge of both T and N 共and table increment per rotation, I) is required to accurately compute the correct value of pitch. 共The value of pitch reported on some systems is not consistent with the International Electrotechnical Commission’s definition, which is used in the ACR program.兲 However, the 2426 McCollough et al.: Phantom portion of the ACR CT accreditation program 2426 user interfaces for many CT systems do not clearly identify the values of these important acquisition parameters. Additionally, some 16-detector-row scanners use only 12-detector rows for certain acquisition modes, yet the user is not explicitly notified whether N⫽12 or 16 for a given clinical protocol. Hence, serious confusion can exist as to the exact values of T, N, and I for clinical exam protocols, which are typically prescribed in terms of reconstructed scan width, table travel speed 共mm/rotation兲, and for some systems, pitch. To assist users in determining the correct values of T, N, and I, information regarding specific scanner models is provided on the frequently asked questions 共FAQ兲 page of the ACR accreditation web site: www.acr.org. 2. Essential criteria for Table I • Detector configuration must be correctly reported. • Pitch must be correctly reported. • Other scan parameters must appear correct. B. SMPTE test pattern Prior to filming any images, a SMPTE test pattern 共Society of Motion Picture and Television Engineers兲 should be printed using the appropriate window width and window level. Users who are unfamiliar with this procedure, should review Gray et al.1 and contact their local service engineer for assistance. A SMPTE test pattern is REQUIRED to demonstrate the quality of the submitted hard-copy film. Failure to submit a SMPTE test pattern results in automatic failure of the physics portion of the accreditation. Alternate patterns are accepted, but not recommended. Figures 2共a兲–2共b兲 show an example of an acceptable SMPTE image and an image with various deficiencies. 1. Essential criteria for SMPTE test pattern • SMPTE or other video test pattern must be present in the first box of each film sheet. • The 95% square must be visible 共whites must not be saturated兲. • The 5% square must be visible 共blacks must not be saturated兲. • No aliasing of bar patterns or other artifacts. C. Phantom and scanner alignment—Modules 1 and 4 The ACR CT accreditation phantom is used for all image quality scans and must first be positioned carefully on the CT table. The HRC protocol from Table I must be used. Even if the site’s HRC protocol does not use a scan width of less than 2 mm, it is essential to use a scan width of less than 2 mm for phantom alignment. In the situation where testing has begun and the physicist must yield the scanner for clinical use, the phantom must be realigned 共modules 1 and 4兲 and new alignment images filmed before proceeding. Figures 3共a兲–3共d兲 show an example of acceptable phantom alignment and several images with various deficiencies. Medical Physics, Vol. 31, No. 9, September 2004 FIG. 2. 共a兲 Good SMPTE image. Neither blacks nor whites are saturated. No artifacts. 共b兲 Unacceptable SMPTE image. The whites are saturated 共note that the 95% square is not visible兲 and numerous horizontal line artifacts are present. 1. Essential criteria for phantom alignment • Image thickness must be 2 mm or less. • All four BBs must be seen in one image and have similar appearance. • Longest wire must be centrally located (⫾1 wire兲 on both top and bottom ramp. 2427 McCollough et al.: Phantom portion of the ACR CT accreditation program 2427 FIG. 3. 共a兲 Excellent alignment. Longer central wires are in the center of both the top and bottom ramps. All four BBs are equally bright. Note the Teflon rings from the phantom stand. 共b兲 Poor alignment. Text annotation covers some BBs, making them difficult to see. The central wire is visible on the top ramp but not on the bottom ramp. Also, image orientation 共left/right兲 is wrong. 共c兲 Poor alignment. The central wire is visible on the bottom ramp but not on the top ramp. Top and left BBs are not as bright as the right BB. Annotation covers the bottom BB. The gray ring partially around the location of the high precision solid water rod is from the phantom manufacturing process and is not a scanner artifact. This ring is not considered to be problematic and is present in varying degrees on most of the phantoms produced. 共d兲 FOV too large: Alignment for module 4 is fine, but the reconstruction field of view 共FOV兲 is too large 共should be 21–25 cm兲. D. Module 1—CT number calibration CT scanners are quantitative devices where pixel brightness should accurately reflect the atomic number and physical density of the material within an image voxel. By defini-tion, the CT number of water and air are assigned values of 0 and ⫺1000, respectively. The CT numbers for all other materials can vary somewhat depending on the system’s x-ray beam spectra and Medical Physics, Vol. 31, No. 9, September 2004 other issues such asbeam hardening and scatter. The various phantom materials have been assigned CT numbers consistent with average values obtained from multiple scanner models. A measured value that is out of the recommended range is not a major deficiency, although the CT number of water is expected to be 0⫾7 HU for images acquired at any slice thickness or kVp setting. The high-precision solid water rod in module 1 has 2428 McCollough et al.: Phantom portion of the ACR CT accreditation program 2428 FIG. 4. 共a兲 Good CT number calibration image. ROIs are well positioned. Note the subtle gray shading around the high-precision water rod. This is from the phantom manufacturing process and is not a scanner artifact. 共b兲 CT numbers out of recommended range: This image demonstrates mean CT numbers for water, acrylic, and polyethylene that are outside the program recommendations. 共c兲 Image lacks the necessary text annotation. Essential details such as kVp, mAs, scan thickness, reconstruction algorithm, etc., are all missing. These technical factors must be displayed on all filmed images. been shown to give mean CT numbers of approximately 0⫾2 HU for a wide range of CT scanner models. Hence, mean CT numbers for water that are not within the program tolerances indicate that scanner calibration should be repeated. Figures 4共a兲– 4共c兲 show an example of acceptable CT number calibration image and two images with various deficiencies. Medical Physics, Vol. 31, No. 9, September 2004 1. Essential criteria for CT number calibration • ROIs must be placed within the cylinders. • Polyethylene mean CT number must be between ⫺107 and ⫺87 HU. • Water mean CT number must be between ⫺7 and ⫹7 HU (⫾5 HU preferred兲. 2429 McCollough et al.: Phantom portion of the ACR CT accreditation program 2429 FIG. 5. 共a兲 Good slice thickness image. In this example, we count 15 wires for both the top and bottom ramp, which indicates a scan thickness of 7.5 mm. 共b兲 Not centered: The image submitted should have been obtained at the table position where the scan is centered on the center of the ramp 共the longer wire should be centered within the other wires兲. In this case of a 10 mm scan thickness, the scan width may extend beyond the ramp 共where there are no more wires兲 and, hence, the measurement may not be accurate. Additionally, the reconstructed FOV is too large 共400 mm兲. Note: The white ring around the high precision water rod is adhesive from the manufacturing process. It is not problematic for the purposes of the accreditation program. 共c兲 Streak artifacts coming off of the wire ramp. These are not typical. Also streaks are seen coming in from the bottom left and right from the Teflon roller on the phantom stand. When setting up the phantom, the ring should be placed under the far ends of the phantom to avoid these streaks. 共d兲 Slice thickness too large: The measurement appears to have been performed correctly yet the measured scan width is too large. The prescribed width is 1.5 mm, but six wires are counted on the top ramp 共3 mm兲, and five wires counted on the bottom ramp 共2.5 mm兲. Additionally, the reconstructed FOV is too large 共400 mm兲. • Acrylic mean CT number must be between ⫹110 and ⫹130 HU. • Bone mean CT number must be between ⫹850 and ⫹970 HU. Medical Physics, Vol. 31, No. 9, September 2004 • Air mean CT number must be between ⫺1005 and ⫺970 HU. • The adult abdomen protocol from Table I must be used. 2430 McCollough et al.: Phantom portion of the ACR CT accreditation program 2430 FIG. 6. 共a兲 Acceptable image. This 140 kVp image has a mean CT number for water of 0.28 HU. In the 80, 100, and 120 kVp images from this scanner 共not shown兲, the mean CT number of water was 1.46, 0.90, and 0.53 HU, respectively, demonstrating solid scanner calibration independent of kVp setting. 共b兲 Incorrect mean CT number for water. This 80 kVp image has a mean CT number of ⫺6.8 HU, which is at the limit of the program tolerances, suggesting the need for scanner recalibration 共many states require water values between ⫺5 HU and ⫹5 HU). Significant ring artifacts are apparent, indicating that the scanner requires calibration or service. 共c兲 Incorrect mean CT number for water. This 90 kVp image has a mean CT number of 12.6 HU, which is well beyond program limits and indicates the need for scanner recalibration at this kVp setting. 共d兲 Filming artifacts: This 80 kVp image has a mean CT number of ⫺2.7 HU, which is acceptable. However, horizontal artifacts are well visualized. These are from the hard-copy camera device 关same camera as used for Fig. 2共b兲 showing the poor quality SMPTE兴. The medical physicist should note and address artifacts seen in any of the accreditation images. E. Module 1—slice thickness and CT number of water versus slice thickness The width of the CT image is most completely described by a section sensitivity profile, particularly for spiral 共helical兲 images. For the purposes of the ACR CT accreditation program, only axial slice widths are measured. These are measured using a series of discrete wires positioned on a ramp Medical Physics, Vol. 31, No. 9, September 2004 inclined with respect to the axial plane such that the spacing between contiguous wires represent 0.5 mm along the z axis. Thus, an estimate of slice width 共in mm兲 can be obtained by counting the number of well-visualized wires and dividing the total number by 2. Very subtle appearing wires should not be counted. Interobserver variability by this method is about 0.5 mm. Additionally, the mean CT number of water is 2431 McCollough et al.: Phantom portion of the ACR CT accreditation program 2431 FIG. 7. 共a兲 Good low contrast resolution image. Adult abdomen protocol. Minimum resolvable rod size⫽5 mm 共need to see all four rods clearly兲. Measured CTDIw⫽22.8 mGy, CTDIvol⫽15.2 mGy. 共b兲 Acquisition and analysis errors. Head scan FOV was used 共large scan FOV should be used for an abdomen protocol兲. ROI positioned radially too far from center. Minimum resolvable rod size⫽6 mm. 共The 5 mm rods are not all well visualized.兲 共c兲 Ring artifact and other deficiencies. The low contrast test object is rotated by 90°. This is a manufacturing error and the site was advised to contact the phantom provider for replacement or repair. The streaks at the lower left and right of the image are from the Teflon roller on the phantom stand. The ROI is positioned radially too far from center. Most importantly, there is a dark ring artifact. Finally, some text annotation covers the low contrast test objects. Minimum resolvable rod size⫽4 mm 共although one is partially hidden by text兲. 共d兲 Failed low-contrast test. The 6 mm diameter low contrast rods are not visible. This site would fail the accreditation. The contrast between the background and the large rod should be 6⫾0.5 HU. Site measures 4.3 HU, but the ROI is not properly positioned. Site was advised to repeat measurement of contrast just to make sure the phantom was not the problem 共we have not found any cases were the phantom was the problem, but it is best to be sure兲. The scan protocol likely needs to be revised or the scanner serviced. 共e兲 Failed low-contrast test. The 6 mm diameter low contrast rods are not all clearly visible. This site would fail the accreditation. The likely cause is the use of the detail reconstruction kernel for an abdomen protocol. This kernel is much too sharp and, hence, the image much too noisy, which severely degrades low contrast resolution. The other scan parameters and dose appear appropriate. 共f兲 Wrong window width and level settings. The images were printed at the wrong window width 共39兲 and level 共91兲. This large of deviation from the prescribed levels 共100/100兲 is not acceptable, as it dramatically alters the appearance of the image and program criteria have been established relative to specified window width and level settings. Also, essential details such as kVp, mAs, scan thickness, reconstruction algorithm, etc., are all missing. These technical factors must be displayed on all filmed images. The reconstructed FOV is also too large 共36 cm instead of 21–25 cm兲. Medical Physics, Vol. 31, No. 9, September 2004 2432 McCollough et al.: Phantom portion of the ACR CT accreditation program 2432 F. Module 1—CT number of water versus kVp setting The mean CT number of water must be evaluated at each kVp setting that can be selected by the operator, regardless of the frequency of use of those settings in the site’s actual clinical practice. Figures 6共a兲– 6共d兲 show an acceptable module 1 image at a nonstandard kVp setting 共i.e., not the kVp noted in Table I for the adult abdomen protocol兲, as well as several images with various deficiencies. 1. Essential criteria for CT number of water versus kVp • Image data are required for all selectable kVp settings. • Water mean CT number must be between ⫺7 and ⫹7 HU (⫾5 HU preferred兲. G. Module 2—low contrast resolution The assessment of low contrast resolution is a difficult yet clinically relevant task. The scan parameters that increase image noise levels can cause subtle 共low contrast兲 objects to be poorly visualized. Alternatively, parameters choices that lower image noise and improve low contrast resolution can result in excessive patient doses. To decrease interobserver variability for this test, the user is instructed to select the smallest set of low contrast objects for which all four objects can be clearly delineated. It is common for sites to claim to be able to see smaller rods than do the reviewers. Figures 7共a兲–7共f兲 and 8共a兲– 8共f兲 show examples of good low contrast resolution images and several images with various deficiencies, using the adult abdomen and adult head protocols, respectively. Common problems include the use of wrong window and level settings, poor positioning of the ROIs 共they should be at the same radial distance from isocenter兲, use of scan parameters that differ from those listed in Table I, and the presence of artifacts. FIG. 7. 共Continued.兲 evaluated at each slice thickness. Figures 5共a兲–5共d兲 show an acceptable slice thickness image and several images with various deficiencies. 1. Essential criteria for CT slice thickness • Image data required for HRC, ⬃3, 5, and 7 mm slice thicknesses. • Water mean CT number must be between ⫺7 and ⫹7 HU (⫾5 HU preferred兲. • The slice width must be within 1.5 mm of the prescribed width. Medical Physics, Vol. 31, No. 9, September 2004 1. Essential criteria for low contrast resolution • Adult abdomen and adult head protocols from Table I must be used. • Window width⫽100. • Window level⫽100. • All four cylinders of the 6 mm rods must be clearly visible. H. Module 3—uniformity Proper calibration of a CT system should result in an image of a uniform phantom that appears uniform and is with- 2433 McCollough et al.: Phantom portion of the ACR CT accreditation program 2433 FIG. 8. 共a兲 Good low contrast resolution image. Adult head 共brain兲 protocol. Minimum resolvable rod size⫽5 mm. The measured CTDIw 共43.0 mGy兲 is below the reference value 共60 mGy兲. However, the module is rotated 共manufacturing error兲 and the annotation is covering some of the test objects. The bright ring around the periphery is not atypical for the head low contrast resolution image, as many scanners assume the presence of skull around the brain and apply a bone correction algorithm. Since the phantom does not have a high-atomic number shell, the bone correction algorithm creates the ring artifact observed. 共b兲 Shading artifact and somewhat high dose. This image has a minimum resolvable rod size⫽5 mm. However, the measured CTDIw 共67.2 mGy兲 is slightly above the reference value 共60 mGy兲. A shading artifact is present where the right portion of image 共left side of phantom兲 appears brighter than the left. 共c兲 Very high dose. Adult head 共brain兲 protocol. This image has a minimum resolvable rod size⫽6 mm 共all 4 of the 5 mm rods are not clearly present兲. However, the measured CTDIw 共114 mGy兲 is almost twice as high as the reference value 共60 mGy兲. ROIs are in the correct position. This site needs to work with their service and applications to optimize the scan parameters such that they can still pass the low contrast resolution 共6 mm or less兲 while hopefully lowering their dose. The high dose required to achieve the necessary level of image quality is in part due to this system’s use of xenon gas detectors. 共d兲 Wrong scan parameters: This image has a minimum resolvable rod size⫽5 mm. However, the image was acquired using the wrong scan parameters. Table I prescribed a 5 mm scan at 160 mA and 2 s 共320 mAs兲 but this scan was taken at 320 mA and 2 s 共640 mAs兲 and is only 2.5 mm thick. 共The two errors should theoretically negate one another in terms of the appearance of the low contrast image.兲 The measured CTDIw 共87.4 mGy兲 is well above the reference value 共60 mGy兲. ROIs are is a good position. 共e兲 Ring artifacts and other problems. This image shows subtle rings artifacts and has the text annotation covering the essential test objects. The window and level settings are not correct. The technique is rather high 共700 mAs兲 likely due to the choice of a 2.5 mm scan thickness, which is typically considered too thin for routine brain evaluations. The measured CTDIw 共105 mGy兲 is almost twice as high as the reference value 共60 mGy兲. The background ROI is not in the correct position. 共f兲 High dose. Good low contrast resolution image using the adult head 共brain兲 protocol. Minimum resolvable rod size⫽4 mm. However, the measured CTDIw 共73.6 mGy兲 is above the reference value 共60 mGy兲. Medical Physics, Vol. 31, No. 9, September 2004 2434 McCollough et al.: Phantom portion of the ACR CT accreditation program 2434 • The center CT number must be between ⫺7 and ⫹7 HU (⫾5 HU preferred兲. • Adult abdomen protocol must be used. • Window width⫽100. • Window level⫽0. • No image artifacts. I. Module 4—high contrast resolution The high contrast resolution image must be viewed using a window width⫽100 and a window level⬇1100 共the window level should be adjusted slightly to optimize visualization of the higher frequency bar patterns兲. The physicist must determine the highest spatial frequency for which the bars and spaces are distinctly visualized. Figures 10共a兲–10共c兲 and 11共a兲–11共c兲 show examples of good high contrast resolution images and several images with various deficiencies, using the adult abdomen and high resolution chest protocols, respectively. 1. Essential criteria for high contrast resolution • The adult abdomen and adult HRC protocols from Table I must be used 共especially correct reconstruction algorithm兲. • Window width⫽100. • Window level⬇1100. • The 5 lp/cm bar pattern must be clearly resolved for adult abdomen. • The 6 lp/cm bar pattern must be clearly resolved for HRC. J. CTDI measurements FIG. 8. 共Continued.兲 out artifacts. Uniformity is quantitated by measuring the mean CT number with a ROI at the center and four edge positions value and calculating the absolute value of 关center mean CT No.—edge mean CT No.兴 for all four edge ROIs. The difference between the edge and center should measure ⭐5 HU. The image should also be carefully examined for artifacts such as rings or streaks. Figures 9共a兲–9共f兲 show an example of a good uniformity image and several images with various deficiencies. 1. Essential criteria for image uniformity • Edge-to-center mean CT number difference must be ⬍5 HU for all four edge positions. • Correct size and location of ROIs. Medical Physics, Vol. 31, No. 9, September 2004 The ACR CT accreditation program requires submission of images from the CTDI measurements primarily to verify the correct phantom size and position, ion chamber usage, and correct acquisition parameters during the CTDI measurements. Figures 12共a兲–12共f兲 show examples of a good CTDI image and several images having critical deficiencies. The standard 16 and 32 cm acrylic CTDI phantoms, 100 mm ionization chamber, and calculation methods are used.2–10 The CTDI measurement must be performed using an axial scan with all other technical parameters 共kVp, mA, exposure time, N, T) the same as the original protocol. For some scanners, this will require paying careful attention to the technical parameters when switching from helical to axial mode. It is absolutely essential that the detector configuration used for the helical scan prescribed in Table I be used for the axial scan for measuring CTDI. In some scanners this may require going into ‘‘service mode’’ to achieve these settings. The FAQ section of the ACR accreditation web site provides additional guidance for this issue: www.acr.org. 1. Essential criteria for CTDI measurements for the adult head protocol • Adult head protocol must be used. • An axial scan must be used. 2435 McCollough et al.: Phantom portion of the ACR CT accreditation program 2435 FIG. 9. 共a兲 Good uniformity image. This image obtained with the adult abdomen protocol from Table I, with the exception of kVp value, shows no artifacts 共cupping, streaks, rings, etc.兲 共note that it is a helical scan, as would be expected for body imaging兲. The data sheets require measuring the mean CT number at the center and four edge positions, but for many systems only three ROI measurements can be displayed at one time. This is acceptable. 共b兲 Cupping artifact. This image visually demonstrates substantial cupping 共darker CT numbers towards the center of the phantom兲, even though the measured CT values are not substantially different from center to edge. Also, the reconstruction FOV is too large and the image was filmed with the wrong window and level settings. 共c兲 ROIs too large. This image shows very good uniformity, however, the sizes of the ROIs are too large. The bright BBs off center and near the edge are missing from the image, most likely due to the site not having filmed the image that is positioned over the center of module 3. 共d兲 Ring artifacts. Concentric ring artifacts are visible in this uniformity image. The four edge ROIs are placed somewhat too near to center. 共e兲 Bright ring artifact around the periphery and helical 共windmill兲 artifacts coming off of the bright BBs. The ROI sizes are too large. 共f兲 Dark ring artifact. The ring around the phantom is not reflected in the acceptable ROI measurements. The ROIs are of good size and position. The BBs appear crisp in spite of a helical pitch factor of 1.5. • Phantom should be in the head holder. • Phantom must be 16 cm in diameter. • The nonchamber holes must be filled. Medical Physics, Vol. 31, No. 9, September 2004 • Complete the dose calculator Excel spreadsheet correctly. 共Parameters must match Table I and actual scan parameters.兲 2436 McCollough et al.: Phantom portion of the ACR CT accreditation program 2436 • Print and submit the dose calculator Excel spreadsheet. • The CTDIw should not exceed 25 mGy. 3. Essential criteria for CTDI measurements for the adult abdomen protocol • • • • • • Adult abdomen protocol must be used. An axial scan must be used. Phantom must be on the table top. Phantom must be 32 cm in diameter. The nonchamber holes must be filled. Complete the dose calculator Excel spreadsheet correctly. 共Parameters must match Table I and actual scan parameters.兲 • Print and submit the dose calculator Excel spreadsheet. • The CTDIw should not exceed 35 mGy. III. CTDI CALCULATIONS An Excel spreadsheet is provided to calculate CTDIw, CTDIvol, DLP, and effective dose from the CTDI measurements.2,3,6 –11 Clinical dose estimates are made using the clinical scan parameters from Table I. Although CTDI measurements are made using an axial scan, exam dose estimates can be made for spiral acquisitions using the parameter CTDIvol, which takes into account gaps or overlaps between the radiation beams from contiguous rotations of the x-ray source. Table II shows a dose calculation worksheet that has been correctly completed. The sample parameters correspond to the adult abdomen protocol given earlier in Table I. IV. DISCUSSION AND CONCLUSIONS FIG. 9. 共Continued.兲 • Print and submit the dose calculator Excel spreadsheet. • The CTDIw should not exceed 60 mGy. 2. Essential criteria for CTDI measurements for the pediatric abdomen protocol • • • • • • Pediatric abdomen protocol must be used. An axial scan must be used. Phantom must be on the table top. Phantom must be 16 cm in diameter. The nonchamber holes must be filled. Complete the dose calculator Excel spreadsheet correctly. 共Parameters must match Table I and actual scan parameters.兲 Medical Physics, Vol. 31, No. 9, September 2004 The provided figures demonstrate acceptable levels of image quality and dose, as well as a variety of image artifacts and scanner performance errors. However, many examples of physicist error have also been shown. The most common operator errors are listed in Table III. The goal of the program is to document high quality scanner performance. In order to fairly assess image quality and dose for a wide range of scanner models and scan acquisition parameters, a reasonable amount of standardization has been necessary in the formatting of the submitted image data. Errors such as filming the images in the wrong location or with the wrong window width and level settings can make an application difficult or even impossible to review fairly. Physicist errors such as not including a SMPTE or other test pattern, severe misalignment of the phantom, or measuring CTDI with the wrong phantom or in helical mode will result in the physicist having to repeat the submission. Thus, paying close attention to the provided instructions is essential. Additionally, the ACR has chosen to assess image quality and dose for four standard imaging applications 共adult abdomen and head, pediatric abdomen, and high resolution chest兲. If a site’s clinical image quality is to be assessed by this program, it is imperative that the submitted phantom images be acquired with the relevant clinical protocols. Hence, 2437 McCollough et al.: Phantom portion of the ACR CT accreditation program 2437 FIG. 10. 共a兲 Good high contrast resolution image. Adult abdomen protocol. The window setting is 100 and the level setting is 1100, allowing the higher frequency bar patterns to well visualized. The limiting spatial resolution 共the highest spatial frequency where the bars are still clearly distinguishable兲 is 7 lp/cm. 共b兲 Wrong window width and level settings. Here the window and level settings have not been properly set (width⫽832 instead of 100, level ⫽1376 instead of 1100兲. The limiting spatial resolution is 6 lp/cm, which is passing. A better window width and level setting would likely show that the 7 lp/cm is the limiting spatial resolution value. 共c兲 Wrong window width and level settings. Here the window width setting is correct but the level has not been adjusted 共from the nominal value of 1100兲 to allow the higher frequency bar patterns to be visualized. The limiting spatial resolution is 7 lp/cm, but a better level setting might show that the 8 lp/cm is the limiting value. working closely with the site’s lead technologist to correctly document the clinical scan parameters in Table I is essential. The physicist must then be diligent to use the scan parameters from Table I in the image quality and dose tests. Through participation in this accreditation program, we believe that the medical physicist will become a more inteMedical Physics, Vol. 31, No. 9, September 2004 grated member of the CT imaging team. While we acknowledge the serious time commitment required for completing a successful CT accreditation application, we believe that the program has helped many to detect and resolve deficiencies in the their scanner performance 共i.e., equipment problems兲 or scanner utilization 共i.e., exam protocols兲. The end result, 2438 McCollough et al.: Phantom portion of the ACR CT accreditation program 2438 FIG. 11. 共a兲 Good high contrast resolution image. High resolution chest protocol. The window width is 108 共acceptable兲 and the window level had been adjusted to 1156 such that the higher frequency bar patterns are well visualized. The limiting spatial resolution is between 9 and 10 lp/cm. 共b兲 Wrong window width and level settings and wrong reconstruction algorithm. The window width setting is not correct 共41 instead of 100兲 and the window level 共1192兲 setting does allow the higher frequency bar patterns to be visualized. Additionally, a high resolution reconstruction algorithm was not used, such that only the bar patterns between 6 and 7 lp/cm can be visualized. 共c兲 FOV too large. The reconstruction FOV is too large, causing the large pixel size to limit the ability to resolve the higher spatial frequency bar patterns that should be visible using the bone algorithm. an increase in the overall quality of CT imaging and a more judicious use of ionizing radiation, is worth the time and attention of the medical physics community. ACKNOWLEDGMENTS The authors of this exhibit gratefully acknowledge the assistance of many people in the development of this proMedical Physics, Vol. 31, No. 9, September 2004 gram, including Pamela Wilcox, Lenny Lucey, and Penny Butler of the ACR, and numerous medical physics colleagues who have provided constructive feedback and invaluable input regarding the program. They additionally would like to thank Dr. Frank Zink and Dr. Jim Kofler, Shawna Leitzen, and Tim Daly, all of the Mayo Clinic, for their assistance with numerous phantom scans during the development stages of this program. 2439 McCollough et al.: Phantom portion of the ACR CT accreditation program 2439 FIG. 12. 共a兲 Good CTDI image. Adult head 共brain兲 protocol. The 16 cm diameter phantom is centered in the head holder and the chamber cavities are filled. The detector configuration for the scan matches that given in, the respective, Table I 共2.5 mm detector collimation兲. 共b兲 Incorrect CTDI scan—helical scan. A helical scan was incorrectly used for acquiring the CTDI measurement. The data from these measurements are not valid for CTDI calculations. 共c兲 Incorrect CTDI scan—wrong size phantom for pediatric dose measurement. The large 共32 cm diameter兲 CTDI phantom was incorrectly used for the pediatric abdomen CTDI measurements. The data from these measurements are not valid for the pediatric CTDI calculations. The incorrect phantom size was discovered by the ACR reviewer after noting that the measured doses were extremely low and seeing that the 30 cm diameter FOV was completely filled in the phantom image. 共d兲 Correct multislice detector configuration used. This image of an adult abdomen CTDI scan corresponds to the scan parameters given in the Table I example above 共with the exception of a different mA value兲. The clinical protocol prescribes a helical 5 mm scan thickness using a pitch of 0.75 and a table speed of 11.25 mm/rotation. These parameters can only be achieved using the 4⫻3.75 mm detector configuration. Here the axial CTDI dose scan is correctly performed using the 4⫻3.75 mm detector configuration 共3.75 mm/4i兲. 共e兲 Incorrect multislice detector configuration used. This image of an adult abdomen CTDI scan corresponds to the scan parameters given in the Table I example above. The clinical protocol prescribes a helical 5 mm scan thickness using a pitch of 0.75 and a table speed of 11.25 mm/rotation. These parameters can only be achieved using the 4⫻3.75 mm detector configuration. Here the axial CTDI dose scan is incorrectly performed using the 4⫻5 mm detector configuration 共5 mm/4i兲. 共f兲 High dose. This head CTDI image uses the same exam parameters as for the head low contrast resolution image shown in Fig. 8共c兲. The technique is high 共160 mA, 3 s兲 and yields a CTDIw of 114 mGy. Medical Physics, Vol. 31, No. 9, September 2004 2440 McCollough et al.: Phantom portion of the ACR CT accreditation program 2440 TABLE II. Sample dose calculation worksheet. CTDI Body Phantom 共32-cm diameter PMMA Phantom兲 Measured kVp 120 mA 240 Exposure time per rotation 共s兲 0.8 Z axis collimation T 共mm兲 3.75 4 # data channels used (N) Axial (A): Table Increment (mm)⫽(I) 11.25 OR Helical (H): Table Speed (mm/rot)⫽(I) Active Chamber length 共mm兲 100 Chamber correction factor 1 Center Measurement 1 共mR兲 152 Measurement 2 共mR兲 155 Measurement 3 共mR兲 154 Average of above 3 measurements 共mR兲 Body CTDI at isocenter in phantom 共mGy兲 12 o’clock position Measurement 1 共mR兲 311 Measurement 2 共mR兲 309 Measurement 3 共mR兲 309 Average of above 3 measurements 共mR兲 Body CTDI at 12 o’clock position in phantom 共mGy兲 CTDIw 共mGy兲 Clinical exam dose estimates 共using measured CTDIw and site’s Adult Abdomen Protocol from Table I兲 CTDIvol 共mGy兲 ⫽CTDIw* N * T/I DLP 共mGy-cm兲 ⫽CTDIvol* 25 Eff Dose 共mSv兲 ⫽DLP* 0.015 FIG. 12. 共Continued.兲 Calculated 153.7 8.9 309.7 18.0 14.9 19.9 498.3 7.5 module, with the outer surface of the BB at the phantom surface at 3, 6, 9, and 12 o’clock positions within the field of view. To assess CT number accuracy, there are cylinders of different materials: bone-mimicking material 共‘‘Bone’’兲, polyethylene, water equivalent material, acrylic, and air. To assess slice thickness, two ramps are included which consist of a series of wires that are visible in 0.5 mm z-axis increments. B. Module 2 APPENDIX: DETAILED DESCRIPTION OF THE ACR CT ACCREDITATION PHANTOM A. Module 1 Figure 13共a兲 shows a cross-section of module I, which is used to assess positioning and alignment, CT number accuracy, and slice thickness. The background material is water equivalent. For positioning, the module has 1-mm diameter steel BBs embedded at the longitudinal (z axis兲 center of the Medical Physics, Vol. 31, No. 9, September 2004 Figure 13共b兲 shows a cross-section of module 2, which is used to assess low contrast resolution. This module consists of a series of cylinders of different diameters, all at 0.6% 共6 HU兲 difference from a background material having a mean CT number of approximately 90 HU. The cylinder-tobackground contrast is energy independent. There are four cylinders for each of the following diameters: 2, 3, 4, 5, and 6 mm. The space between each cylinder is equal to the diameter of the cylinder. A 25 mm cylinder is included to verify the cylinder-to-background contrast level. 2441 McCollough et al.: Phantom portion of the ACR CT accreditation program 2441 TABLE III. Common operator errors. Scans acquired using parameters that do not match those listed in Table I of the site scanning data form 共kVp, mAs, scan width, detector configuration, reconstruction algorithm, scan and reconstruction FOV, etc.兲 Incorrect detector configuration 共values of N and T兲 listed in Table I Incorrect calculation of pitch or table increment Not submitting a SMPTE pattern or alternate video test pattern Poor phantom alignment 共central wire not centered in ramp, all 4 BBs not the same brightness兲 Placing images in the wrong positions 共boxes兲 on the films submitted to the ACR Filming images with the wrong window width and window level settings Wrong size or wrong position ROIs Submitting images having obvious artifacts or other deficient results Performing CTDI scans using the wrong detector configuration 共values of N and T兲 Not submitting the printed Excel ‘‘dose calculator’’ spreadsheet Not noting the difference between mA, mAs, and effective mAs (⫽mAs/pitch) when completing the forms Not displaying sufficient technical parameters on the printed films 共all scan parameters must be shown兲 Positioning ROIs such that the annotation covers important portions of the image Using too small or too large a reconstruction FOV C. Module 3 D. Module 4 Figure 13共c兲 shows a cross-section of module 3, which consists of a uniform, tissue-equivalent material to assess CT number uniformity. Two very small BBs 共0.28 mm each兲 are included for optional use in assessing the accuracy of inplane distance measurements. They may also be used to assess section sensitivity profiles. Figure 13共d兲 shows a cross-section of module 4, which is used to assess high contrast 共spatial兲 resolution. It contains eight bar resolution patterns: 4, 5, 6, 7, 8, 9, 10, and 12 lp/cm. The aluminum bar patterns provide very high object contrast relative to the background material. Module 4 also has four 1 mm steel beads, as described for module 1. FIG. 13. 共a兲 Cross-sectional diagram of module 1, which contains four cylindrical rods to assess the CT number of different materials, four BBs to confirm accurate positioning, and two inclined ramps consisting of discrete wires that are spaced in 0.5 mm increments along the z axis. 共b兲 Crosssectional diagram of the low-contrast resolution test objects contained in module 2. Each cylinder is comprised of the material having a nominal CT number difference from the background material equal to 6 HU. 共c兲 Cross-sectional diagram used to assess image uniformity in module 3. The two 0.28 mm beads are used for optional assessment of distance accuracy or section-sensitivity profile. 共d兲 Cross-sectional diagram of the high contrast 共spatial兲 resolution test objects contained in module 4. The numerical values shown correspond to the spatial frequency of the respective bar pattern, in lp/cm. Medical Physics, Vol. 31, No. 9, September 2004 2442 McCollough et al.: Phantom portion of the ACR CT accreditation program a兲 Presented at RSNA Annual Meeting, November 2003, Recipient of Magna Cum Laude Award for Educational Exhibit. b兲 Author to whom correspondence should be addressed. Electronic mail: mccollough.cynthia@mayo.edu 1 J. E. Gray et al., ‘‘Test pattern for video display and hard-copy camera,’’ Radiology 145, 519–527 共1985兲. 2 T. B. Shope, R. M. Gagne, G. C. Johnson, ‘‘A method for describing the doses delivered by transmission x-ray computed tomography,’’ Med. Phys. 8, 488 – 495 共1981兲. 3 American Association of Physicists in Medicine, Standardized Methods for Measuring Diagnostic X-Ray Exposures, Report no. 31 共AAPM, New York, 1990兲. 4 American Association of Physicists in Medicine, Specification and Acceptance Testing of Computed Tomography Scanners, Report no. 39 共AAPM, New York, 1993兲. 5 L. N. Rothenberg and K. S. Pentlow, ‘‘CT dosimetry and radiation Medical Physics, Vol. 31, No. 9, September 2004 2442 safety’’ in RSNA Categorical Course in Diagnostic Radiology Physics: CT and US Cross-sectional Imaging. RSNA 共2000兲. 6 European Guidelines for Quality Criteria for Computed Tomography 共European Commission, Luxembourg, 2000兲. 7 International Electrotechnical Commission, Medical Electrical Equipment. Part 2-44: Particular Requirements for the Safety of X-ray Equipment for Computed Tomography, IEC publication No. 60601-2-44, 2nd edition, Amendment 1. 8 H. D. Nagel, Radiation Exposure in Computed Tomography 共COCIR, Frankfurt, 2000兲. 9 M. Gray-McNitt, ‘‘AAPM/RSNA physics tutorial for residents: Topics in CT radiation dose in CT,’’ Radiographics 22, 1541–1553 共2002兲. 10 R. L. Morin, T. C. Gerber, and C. H. McCollough, ‘‘Radiation dose in computed tomography of the heart,’’ Circulation 107, 917–922 共2003兲. 11 C. H. McCollough, ‘‘Patient dose in cardiac computed tomography,’’ Herz 28, 1– 6 共2003兲.