Household out-of-pocket health care expenditure trends: 1980–95
advertisement

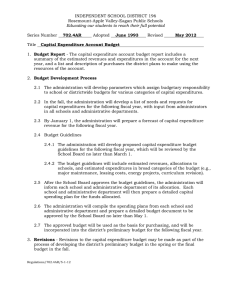
Household out-of-pocket health care expenditure trends: 1980–95 Deanna L. Sharpe,1 Jessie X. Fan2 and Gong-Soog Hong3 1 University of Missouri, MO, USA 2 University of Utah, UT, USA 3 Utah State University, UT, USA Abstract This descriptive study examines household out-of-pocket expenditure trends for health insurance, medical services, prescription drugs and medical supplies using the 1980–95 Consumer Expenditure Surveys. Constant dollar out-ofpocket expenditures for health insurance have risen sharply over time while constant dollar out-of-pocket expenditures for medical services have declined, perhaps reflecting health care market changes. Older consumers spent more in constant dollars and had higher budget shares for all aspects of health care than younger consumers. Although Medicare and Medicaid provide access to basic health care, results indicate that, for older consumers who are poor, health care expenditures may still crowd out spending for other necessities. Keywords Health care, out-of-pocket expenditures. Introduction Health care has become increasingly expensive in the United States. During the 1980s and 1990s, inflation-adjusted national health care expenditures grew between 5% and 6% a year. By the end of the 1990s, national health care expenditures exceeded 13% of U.S. Gross Domestic Product. Health care costs are projected to increase at twice the rate of inflation over the next several years.1 In response, private health insurance companies have passed on cost increases to consumers in the form of higher health insurance premiums, reduced reimbursements and tighter coverage restrictions. Recently, the managed care approach to health care delivery has gained popularity as a means of Correspondence D.L. Sharpe, University of Missouri-Columbia, 239 Stanley Hall, Columbia, MO 65211, USA. E-mail SharpeD@missouri.edu 114 | restraining costs through use of preventive care, prepayment of most medical services and restricting the use of medical services.2–4 The elderly and the poor can obtain basic health care through government funded Medicare and Medicaid respectively.5,6 Tax and transfer payments essentially redistribute a portion of the health care financial burden from these groups to the general population. This redistribution implies that a social contract exists which says that those least able to help themselves as a result of advanced age, limited physical capacity or inadequate economic resources should receive help to meet a basic need. Escalating health care costs have begun to force reconsideration of the form and extent of this social contract, however. Provisions of the 1997 Balanced Budget Act were clearly intended to slow growth in public health care expenditures under Medicare and Medicaid. If accessible and affordable health care for a broad segment of the U.S. population is a public policy goal, assessing household out-of-pocket spending on health care is important for national health policy planning. This study uses 15 years of Consumer Expenditure Survey data to chart trends in constant dollar outof-pocket dollar expenditures and household budget shares for health insurance, medical services, prescription drugs and medical supplies, taking eligibility for government health care programmes into consideration. Findings were used to draw policy implications regarding the effect of health care market changes and the allocation of the health care financial burden. Related literature The health economics literature suggests that the low price that consumers pay out-of-pocket after the insurance company covers the larger share of the costs induces a higher demand for health care.7 In support of this idea, Rubin and Koelln8 found a significant and International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 © 2001 Blackwell Science Ltd D.L. Sharpe et al. • Out-of-pocket health care expenditure trends positive association between having health insurance coverage and the level of out-of-pocket health expenditures; also, the demand for health care increased as financial resources increased. They presented their results as evidence of moral hazard in health care markets and adverse selection in health insurance markets. Moral hazard refers to the increased demand for health care that results from having health insurance coverage. Adverse selection occurs when those most in need of health care services are the ones who purchase health insurance.7 Ace and Sabelhaus9 report that the average household spent 62% more on health care in 1997 than in 1987. In 1987, medical service expenditures took the bulk of the health care dollar, whereas, in 1997, health insurance was the largest component of a household’s health care expenses. Similarly, Paulin and Weber3 found that average spending on health insurance premiums by families rose almost 70% between 1988 and 1993. The out-of-pocket share of health care expenditures for health insurance increased, while the share spent on medical services declined by approximately 10%. Thus, households spent proportionately more on health insurance premiums but less on actual medical services. Out-of-pocket expenditure for in-patient hospital care has declined steadily since the 1980s as a result of the movement of employer-sponsored insurance, Medicare, and Medicaid to managed care, and increasing numbers of treatments in ambulatory settings. These changes resulted in fewer hospital admissions and in-hospital days, which, in turn, slowed the increase in out-of-pocket spending for hospital care. Out-of-pocket expenses for physician services fell by 9.2% between 1980 and 1992 and have increased slowly since 1992 with annual growth rates of less than 10%.10 Ace and Sabelhaus9 reported that average out-ofpocket expenses for prescription drugs have been fairly stable although the aggregate outlays for prescription drugs have increased since the mid-1990s. Baker and Kramer11 explained that bulk rate, mail-order prescription drug services, generous insurance coverage and inexpensive generic drugs might have contributed to the stable growth (as opposed to significantly greater growth) in out-of-pocket expenses for prescription drugs. © 2001 Blackwell Science Ltd Method Data Data for this study are from the interview portion of the 1980–95 Consumer Expenditure Surveys (CES). The CES collects data quarterly from approximately 5000 consumer units (generally, household members related by blood, marriage, adoption or other legal arrangement) in a rotating panel design.12 Consumer units typically contribute data for five consecutive quarters. Each quarter, 20% of the sample is replaced with new participants. Although the survey focuses on both regular and relatively large household expenditures, limited demographic, social and economic data are also obtained from consumer unit members. Sample For each year from 1980–1995, consumer units that contributed to four consecutive quarters of information in a given year and that were complete income reporters were selected. A few cases that had expenditure values for medical services greater than two standard deviations from the mean were deemed outliers and were excluded. The final sample in this study consisted of 14 513 consumer units (for all years combined). Analysis To make comparisons using constant dollars across time, expenditure levels for each year were converted to 1996 dollars using the Consumer Price Index (CPI). Then, overall trends in out-of-pocket expenditures for health insurance, medical services, prescription drugs and medical supplies made between 1980 and 1995 were charted using the entire sample. This approach facilitates comparison of similarities and differences in expenditure trends among the four types of health expenditures, but presumes that all consumers within the sample face similar health care costs. Use of Medicare or Medicaid, however, could reduce out-ofpocket costs for eligible households. To account for Medicare eligibility, the sample was subdivided into those under age 65 years (younger consumers) and those aged 65 years or older (older con- International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 | 115 Out-of-pocket health care expenditure trends • D.L. Sharpe et al. 1200 Constant dollar (1996 $) sumers). As Medicaid use was not reported in the early years of the CES data used in this study, poverty status was used to proxy access to Medicaid. Although the specific requirements for receiving Medicaid have varied over time, as a means-tested programme it is generally available to those with low income. In both age groups, those who had expenditures at or below 125% of the official poverty threshold were classified as poor (designated as lower income in the figures); all others were classified as non-poor (designated as higher income in the figures). Data limitations in the CES led to use of total expenditures to proxy income.13 The choice of the 125% was based on recent criticism that the official poverty threshold is too stringent and does not adequately identify the poor.14 1000 Health insurance 800 Prescription drugs Medical supplies 600 Medical services 400 200 0 80 82 84 86 88 90 Year 92 94 96 Figure 1 Out-of-pocket expenditures (in 1996 constant dollars) on health care by expenditure categories: 1980–95. Variables Four types of health-related expenditures, as categorized in the CES data, were examined: health insurance, medical services, prescription drugs and medical supplies. Health insurance included commercial health insurance, Blue Cross or Blue Shield plans, health maintenance plans, Medicare premiums, commercial Medicare supplements, and other types of medical insurance such as dental insurance. Medical services included net outlay for services of physicians and other medical professionals, lab and hospital services (other than room), dental care, and eye exams, treatment or surgery. Net outlays for medicines and prescription drugs were combined. The net outlay for purchase of eye glasses or contact lenses, medical or surgical equipment (e.g. ice bags, heating pads, orthopaedic appliances, etc.), supportive or convalescent medical equipment (e.g. wheelchair, braces, etc.), or hearing aids comprised out-of-pocket spending for medical supplies. Findings Overall trends Lines for the four types of health expenditures for all consumers (Fig. 1) indicate that, before the late 1980s, out-of-pocket expenditures for medical services were above out-of-pocket expenditures for health insurance. After that time, out-of-pocket expenditures for 116 | health insurance exceed out-of-pocket expenditures for medical services. The two lines no longer track together but diverge, with out-of-pocket expenditures for health insurance continuing to rise and out-of-pocket expenditures for medical services declining. These findings are consistent with previous research3,7 and probably reflect both the prepayment of medical services and restricted access to medical services under managed care. Increases in prescription drug costs have received blame for rising health care costs.15 Fig. 1 suggests, however, that constant dollar out-of-pocket prescription drug expenditures have remained relatively constant over time. Taken together, these facts suggest that some of the higher cost may be indirectly borne by the consumer in the form of higher health insurance premiums. Alternatively, employees may have received reimbursement for prescription drug costs from their employer’s medical savings account. Or, the relatively low spending by some consumers may offset the high level of spending on prescription drugs by other consumers. Not surprising, constant dollar out-of-pocket expenditures for medical supplies were relatively low and flat across all years of this study. Many commonly used medical supplies are relatively inexpensive; few consumers would purchase more costly medical supplies. Thus, average spending for medical supplies across a broad spectrum of consumers would remain low. International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 © 2001 Blackwell Science Ltd D.L. Sharpe et al. • Out-of-pocket health care expenditure trends 2000 Trends in budget share of total out-of-pocket expenditure on health care Trends by expenditure type Health insurance expenditure As seen in Fig. 3, heath insurance expenditures trend upwards rather sharply for all consumers except the young poor. While the latter group also experienced increasing expenditure levels, the change over time was not quite as dramatic as it was for other groups. In this respect, the group-specific expenditure trends mirror the expenditure trends seen in the overall analysis. Costs are not borne equally by all consumers, however. Over the 15-year period, those aged 65 years and older spent more than those under age 65 years, despite their Medicare eligibility. Within each age group, the expenditure level of the poor is below that of the non-poor, < 65 higher income 1000 < 65 lower income 500 Total health care budget share (%) 18 ≥ 65 higher income 16 ≥ 65 lower income 82 84 86 88 90 Year 92 94 96 Figure 3 Out-of-pocket expenditures (in 1996 constant dollars) on health insurance by age and income groups: 1980–95. 14 ≥ 65 higher income 12 10 ≥ 65 lower income 8 < 65 higher income 6 < 65 lower income 4 2 0 80 20 ≥ 65 lower income 1500 0 80 Health insurance budget share (%) Older consumers devoted a larger share of their budget to all health care expenditures than younger consumers did, a share that generally increased over time (Fig. 2). Older consumers with lower incomes spent a larger proportion of their budget on health care than those with higher incomes. Among younger consumers, those with higher incomes devoted a larger budget share to health care, perhaps reflecting both an increased ability to pay and a willingness to make human capital investments in health. Health insurance (1996 $) ≥ 65 higher income 82 84 86 88 90 Year 92 94 96 Figure 4 Budget share of health insurance by age and income groups: 1980–95. 14 < 65 higher income 12 10 < 65 lower income 8 suggesting that, among the poor, either Medicaid is an effective substitute for own purchase of health insurance or a substantial number opt to be under- or uninsured. 6 4 2 80 82 84 86 88 90 Year 92 94 96 Figure 2 Budget share of total out-of-pocket expenditures on health care by age and income groups: 1980–95. © 2001 Blackwell Science Ltd Health insurance budget share As a share of the household budget, out-of-pocket spending on health insurance is clearly a greater burden for those aged 65 years and older than for those who are younger (see Fig. 4). Indeed, for older individuals, health insurance expenditures have required an increas- International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 | 117 Out-of-pocket health care expenditure trends • D.L. Sharpe et al. Medical services expenditure The level of expenditure on medical services for the groups shown in Fig. 5 repeats the slight downward trend depicted in the overall analysis (Fig. 1). It is not entirely clear what contributed to the volatility in spending among the non-poor aged 65 years and older. Introduction of the Consolidated Omnibus Reconciliation Act of 198516 may have encouraged some retiring employees to purchase continued group health coverage from their former employer, allowing them to use health care as needed rather than forgoing or postponing medical services. Market adjustment to the new legislation may have contributed to the subsequent up and down swings before a decided downward trend prevailed. Expenditure levels were clearly lower for the poor in both age groups, perhaps reflecting either substantial subsidization of the cost of medical services by Medicaid or limited utilization of medical services by the poor. 2000 Medical services (1996 $) ≥ 65 higher income ≥ 65 lower income 1500 < 65 higher income 1000 < 65 lower income 500 0 80 82 84 86 88 90 Year 92 94 96 Figure 5 Out-of-pocket expenditures (in 1996 constant dollars) on medical services by age and income groups: 1980–95. 118 | 6 Medical services budget share (%) ingly large proportion of the household budget over time. This proportion was greater and the upward trend in the budget share was steeper for the poor in the older group. In contrast, the budget share levels for both the non-poor and poor among the young show only a slight increase over time. ≥ 65 higher income 5 ≥ 65 lower income 4 < 65 higher income 3 < 65 lower income 2 1 0 80 82 84 86 88 90 Year 92 94 96 Figure 6 Budget share of medical services by age and income groups: 1980–95. Medical services budget share All four groups devoted an increasingly smaller share of their budget to medical services over time (see Fig. 6). Within each age group, though, the share of the budget allocated to medical services was lower for the poor than for the non-poor. At least until the early 1990s, the budget shares for medical services for older consumers were greater than that of younger consumers. After 1992, the continuing decline in the medical services budget share for older poor consumers crossed the line for the younger non-poor consumers, a line that declined only slightly over the time period studied. Prescription drug expenditure While the analysis of trends in health care spending for all consumers indicated that prescription drug expenditure had remained relatively flat over time, the disaggregated trends clearly indicate that older consumers spent considerably more than younger consumers on prescription drugs (see Fig. 7). Indeed, expenditures by poor and non-poor older consumers move decidedly upwards, while those of poor and non-poor younger consumers appear to remain relatively constant over time. This difference may reflect the fact that older individuals typically have a greater need for prescription drugs owing to declining health. Prescription drugs may be used to prevent or postpone more costly medical procedures.17 Younger individuals may have greater access to prescription drug benefits through their International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 © 2001 Blackwell Science Ltd D.L. Sharpe et al. • Out-of-pocket health care expenditure trends 700 160 Prescription drugs (1996 $) 600 500 ≥ 65 lower income 400 < 65 higher income < 65 lower income 300 200 100 0 80 Medical supplies (1996 $) ≥ 65 higher income 140 ≥ 65 higher income 120 ≥ 65 lower income 100 < 65 higher income 80 < 65 lower income 60 40 20 82 84 86 88 90 Year 92 94 0 80 96 82 84 86 88 90 Year 92 94 96 Figure 7 Out-of-pocket expenditures (in 1996 constant dollars) on prescription drugs by age and income groups: 1980–95. Figure 9 Out-of-pocket expenditures (in 1996 constant dollars) on medical supplies by age and income groups: 1980–95. employer-sponsored group health plan. In contrast, Medicare does not cover prescription drug costs; thus, those over age 65 years must either pay the costs outof-pocket or purchase a Medicare supplement that covers prescription drugs. 65 years and older, however, the budget share for prescription drugs trended decidedly upwards, with the lines for the poor typically slightly higher than the nonpoor among this group.These findings suggest that older consumers bear a relatively greater burden in paying for prescription drugs than younger consumers, a burden that is heavier for the poor among older consumers. Prescription drug budget share Figure 8 indicates that the budget share allocated to prescription drugs among those under age 65 years remained relatively flat and at about the same level over time for both the poor and the non-poor. For those aged Prescription drugs budget share (%) 4 ≥ 65 higher income ≥ 65 lower income 3 < 65 higher income 2 < 65 lower income 1 0 80 Medical supply expenditure Trends in medical supply expenditure for the disaggregated groups (see Fig. 9) are clearly more volatile than the overall trend analysis revealed. The non-poor spent more than the poor. Within each income group, older consumers generally paid more out-of-pocket than younger consumers. 82 84 86 88 90 Year 92 94 96 Figure 8 Budget share of prescription drugs by age and income groups: 1980–95. © 2001 Blackwell Science Ltd Medical supply budget share The budget share for medical supplies reflects the same volatility seen in the trend lines for expenditures (see Fig. 10). Still, it is clear that out-of-pocket expenditures for medical services represent a larger share of the budget for those age 65 years and older than for younger individuals, probably reflecting a greater need for medical supplies among older consumers. Policy implications Policy implications related to the health care expendi- International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 | 119 Out-of-pocket health care expenditure trends • D.L. Sharpe et al. Medical supplies budget share (%) 1 ≥ 65 higher income 0.8 ≥ 65 lower income 0.6 < 65 higher income 0.4 < 65 lower income 0.2 0 80 82 84 86 88 90 Year 92 94 96 Figure 10 Budget share of medical supplies by age and income groups: 1980–95. ture trends examined in this study centre on two issues: (1) the possible effect of recent health care market changes on consumer behaviour and the quality of health care received; and (2) the allocation of the health care financial burden between public and private payers in the health care market. Impact of health care market changes As previously discussed, the steep rise in health insurance expenditure for all except the poor among the younger consumers may reflect the shift towards prepayment of medical services under managed care plans. The rise in health insurance spending may also reflect the trend toward requiring the ultimate consumer to share a larger proportion of the total cost. If such cost sharing reduces the moral hazard, both consumers and health care markets can benefit. Out-of-pocket costs will more accurately reflect the true cost of health care, thus encouraging consumers to make wise choices. Consequently, the health care market may become more competitive. On the other hand, should the increase continue, consumers will either cut back on other areas of their budget to afford health insurance or, ultimately, they will not be able to afford the higher premium and will either be underinsured or become uninsured. The latter situation can have large social costs. If treatment for health conditions is not sought until a crisis occurs 120 | (e.g. emergency room visits), the care is costly, making payment collection difficult. The cost of uncollected payments will probably shift to those who purchase health insurance or who make various other types of payments for health care use. If the reduction in out-of-pocket costs in medical services noted in this study is the result of increasing efficiency in ways that did not compromise patient care, both the consumer and the health care industry benefit. However, the decline in medical services expenditure may also reflect managed care practices of reducing in-hospital days or limiting physician visits or access to specialists. Recent passage of a California law allowing patients to sue health maintenance organizations (HMOs) for punitive damages suggests disagreement exists regarding care quality in managed care settings.18 At present, few states have similar laws permitting HMOs to be sued for malpractice. Pressure to pass such legislation may arise, however, if consumers believe that cost reductions compromise health care quality for themselves or for family members. Allocation of health care financial burden Study results indicate that older consumers spend more on health insurance and devote a larger share of their budget to health insurance than younger consumers do, regardless of income level. Among those aged 65 years and older, those who can pay (i.e. the non-poor) apparently do pay, as their out-of-pocket costs for all types of health care expenditure were relatively higher than that of other groups. Examination of budget share trends, however, suggests that the rising health-related expenditures of older consumers, especially those who are poor, may ‘crowd out’ other budget items. For those who have relatively low or fixed incomes, serious problems can arise if purchase of other necessities must be forgone to afford health care. Medicare provides basic health insurance to virtually all those aged 65 years and over at no or low cost. The upward trend in health insurance expenditures among those aged 65 years and older strongly suggests that older consumers do not consider Medicare alone to be sufficient for their health insurance needs, thus they purchase relatively costly supplemental insurance. Public spending cutbacks may have little practical impact on International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 © 2001 Blackwell Science Ltd D.L. Sharpe et al. • Out-of-pocket health care expenditure trends those able to afford alternative coverage in the private sector. For those who cannot afford such coverage, however, the ability to obtain adequate health care may be compromised. Medicare does not fund long-term care nor does it cover prescription drugs. Medicaid, however, covers both items to a limited extent for those who meet stringent requirements for low income and resources. Indeed, many seniors strategically spend down their assets to qualify for Medicaid so that they can afford long-term care. Currently, over 40% of Medicaid costs cover nursing home and intermediate care. Although the aged, disabled and blind comprise only one-fourth of Medicaid recipients, their care accounts for twothirds of programme costs.19 If Medicaid cost reduction restricts such payments, the health care financial burden of seniors needing nursing home and related care will substantially increase. In some cases, the burden may be borne by family members or other payers. In other cases, poor quality or inadequate care may be obtained owing to financial constraints. Trends in both the level of expenditure on and budget share for prescription drugs are markedly higher for older consumers than for younger consumers, owing in part to more extensive use of prescription drugs among older consumers. On average, older individuals take over 10 different prescription drugs every day.17 Addition of prescription drug benefits to Medicare is currently being debated.20,21 Given the high cost of prescription drugs coupled with an ageing population, it is clear that any effort to fund prescription drug purchase under Medicare must be carefully structured to avoid obligating government to pay a bill that spirals ever higher. At the same time, to the extent that public policy and managed care directives shift prescription drug and other health care costs back to the household, those with relatively low levels of post-retirement income may have to forego needed medications. The young poor had both the lowest level of spending on and budget share for all four health-related expenditures in this study. Use of Medicaid may have contributed to that situation. Evidence exists, however, that Medicaid reaches only about half of the poor, owing to complex eligibility requirements and state variations in programme funding and implementation.19 Obviously, programme cutbacks will have little direct © 2001 Blackwell Science Ltd effect on those who are eligible but not currently using the programme. To the extent that programme cutbacks reduce health care access for the poor, however, other social costs can rise. Human capital is diminished. Costs of providing care to those who cannot pay will certainly be passed on to those who can pay in the form of higher prices. Conclusion Designing policy that makes health care accessible and affordable for a broad spectrum of the population is challenging. Declining health typically forces older consumers to pay more than younger consumers for all components of health care.Thus, the cost reductions and subsidies provided by Medicare and Medicaid can be important to those aged 65 years and older. Population ageing and increased longevity may shift more public dollars to those over age 65 years than to those of a younger age. Given limited government resources, escalating health care costs could displace other forms of social investment such as education that tend to benefit the younger generation. Legislated spending restrictions on Medicare and Medicaid may shift at least a portion of the burden of health care financing to those consumers least able to absorb the additional costs owing to low or fixed income levels. In light of these factors, difficult decisions must be made in the public policy arena regarding who will receive health care financing, how much will be received and for how long. These decisions will affect the quality of care received and the distribution of the health care financing burden for both current and future generations. References 1. Thorpe, K.E. (1997) Changes in the growth in health care spending: Implications for consumers. National Coalition on Health Care, Washington, D.C. 2. Mizrahi, T. (1993) Managed care and managed competition: A primer for social work. Health and Social Work, 18, 85–91. 3. Paulin, G.D. & Weber, W.D. (1995) The effects of health insurance on consumer spending. Monthly Labor Review, 118 (3), 34–54. 4. Remler, D. & Blendon, R. (1997) What do managed care plans do to affect care? Inquiry, 34, 196–204. International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 | 121 Out-of-pocket health care expenditure trends • D.L. Sharpe et al. 5. U.S. Department of Health and Human Services (2000) Medicare: The official U.S. government site for Medicare information. http://www.medicare.gov/default.asp. November 30, 2000. 6. Health Care Financing Administration (2000) Medicaid consumer information. http://www.hcfa.gov/medicaid/ medicaid.htm. November 30, 2000. 7. Feldstein, P. (1993) Health Care Economics. Delmar Publishers, Albany, NY. 8. Rubin, R. & Koelln, K. (1993) Determinants of household out-of-pocket health expenditures. Social Science Quarterly, 74, 721–735. 9. Ace, G. & Sabelhaus, J. (1995) Trends in out-of-pocket spending on health care, 1980–92. Monthly Labor Review, December, 35–45. 10. Levit, K., Cowan, C., Braden, B., Stiller, J., Sensenig, A. & Lazenby, H. (1998) National health expenditures in 1997: more slow growth. Health Affairs, 17 (6), 99–110. 11. Baker, C. & Kramer, N. (1991) Employer-sponsored prescription drug benefits. Monthly Labor Review, February, 31–35. 12. U.S. Department of Labor (1996) 1994 Interview survey CD ROM/ public use tape documentation. 13. Sharpe, D.L. & Abdel-Ghany, M. (1999) Identifying the poor and their consumption patterns. Family Economics and Nutrition Review, 12 (2), 15–25. 122 | 14. Citro, C.F. & Michael, R.T. (eds.) (1995) Measuring poverty: a new approach. National Academy Press, Washington, DC. 15. Moran, D.W. (2000) Prescription drugs and managed care: can ‘free-market détente’ hold? Health Affairs, 19 (2), 63–77. 16. House of Representatives (1985) Consolidated Omnibus Budget Reconciliation Act of 1985. Report 99–453. US Government Printing Office, Washington, DC. 17. Dubois, R.W., Chawla, A.J. & Neslusan, C.A. (2000) Explaining drug spending trends: Does perception match reality? Health Affairs, 19, 231–239. 18. Wilson, R. (1999) (October 5) Do you have the right to sue your HMO? Cable News Network. http://www.cnn. com/HEALTH/9910/05/hmo.suing.wmd/index.html. November 30, 2000. 19. Cochran, C.E., Mayer, L.C., Carr, T.R. & Cayer, N. Joseph (1996) American public policy: An introduction, 5th edn. St. Martin’s Press, New York. 20. Christensen, S. & Wagner, J. (2000) (March/April) Cost of a medicare prescription drug benefit. Health Affairs, 19, 212–218. 21. Cook, A.E. (1999) Strategies for containing drug costs: implications for a Medicare benefit. Health Care Financing Review, 20 (3), 29–37. International Journal of Consumer Studies, 25, 2, June 2001, pp114–122 © 2001 Blackwell Science Ltd