Acquiring, Maintaining, and Customizing Organizational
advertisement

From: AAAI Technical Report SS-97-01. Compilation copyright © 1997, AAAI (www.aaai.org). All rights reserved.
Acquiring, Maintaining, and Customizing Organizational
WorkProcess Descriptions
Douglas B. Fridsma, John Gennari, and Mark Musen
Section on MedicalInformatics
Stanford UniversitySchoolof Medicine
StanfordUniversity
Stanford, CA94305-5479
{fridsma, gennari, musen}@smi.stanford.edu
Abstract
Models
of workprocessesandof organizations’
activities
are an importantpart of workfiow
systemsandsimulation,
andcaptureproceduralknowledge
stored withinthe organization.However,
acquiring,maintaining,andcustomizingthesemodels
canbe difficult. Toassist the acquisition andmaintenance
of organizationalmodels,we
havedeveloped
a set of knowledge-acquisition
tools suitable for use in the domain
of medicalorganizations.In
modeling
medicalorganizationprocesses,three areas of
expertisemustbe broughttogether.Expertisein medical
care, organizational
structure,andmodeling
is necessary
to describeaccuratelythe processof medical
caredelivery
for simulationor workflow
management.
Weproposea
method
of modeling
workprocessesthat usesthe Protege
suite of tools to generateorganization-specific
workprocess descriptions.Wehavecreateda set of Protegeknowledge-acquisition
tools customized
for medical,organization, andmodeling
experts, andhaveuseda prototype
systemto create detailed,site-specificprocessdescriptions. In our prototype
system,wehaveidentifieda set of
transformation
operatorsthat shouldmakepossibleadditional computer-based
support.Webelievethis methodologywill improve
acquisitionof an organizational
model,
andmakeit easier to maintainan accuratemodelin the
face of changesin medicalprocessor organizational
structure.
Work Process Descriptions
Therehas beena recent interest in creating organization
modelsthat are predictive of organizationalperformance,
or capableof providinginsight into theories of organizations (Levitt et al, 1994). Organizationmodelscan capture the tacit knowledgecontained in organizational
processes, and allow organizations to evaluate and improve these procedures. However,for these computerbasedsimulationsto be successful, builders of organization modelsmustinvest significant effort into creating
detailed modelsof organizational structure and work
processes. Building accurate organization modelsrequires the modelbuilders to havea detailed understand40
ing of the organization, the workthat it does, and the
interactions betweenthe workprocess and the organization structure. In complexdomainssuch as medicine,
organization modelconstruction can be a particularly
difficult task, and mayrequire bringing together many
different areas of expertise(Bumset al, 1995).It is only
by bringingtogether these areas of expertise, that model
builders can craft a representativedescription of a particular work process and organization. If the model
builders are successful, their modelwill reflect the
structure and processesas they existed whenthe modelis
constructed.
In medicine,protocols for patient care can be considered workprocessdescriptions in that they describe the
steps necessaryto care for a patient witha particular illness (Field & Lohr, 1990). There has been significant
effort at both national andinstitutional levels to create
standard care plans, critical pathways,and protocols to
reduce practice variability and to improvethe quality of
patient care. Whenproperly followed, protocols do have
the desired effect of improvingpatient care while reducing patient care costs (Loback& Hammond,
1994).
Unfortunately, medicalprotocols are not static. For
medicalprotocols to be accepted, most undergochanges
to makethem specific to a clinical setting. These
changes maybe as simple as specifying the preferred
formularydrugs available at an institution, indicating
whichreferral formsare required to order a particular
laboratorytest, or designatingwhocan schedulea procedure. Moreradical eustomizationsinclude changingthe
order of guideline activities to streamlineschedulingof
patients in the clinic. Manyinstitutions recognizethe
importanceof creating medicalprocessdescriptions that
are specific to their organization, and havea medical
director or committeesof health care providersto create
these specialized protocols. Theseadministratorstransformthe generic protocolsinto a site-specific protocols
moreacceptableto the practitioners in the institution and
more capable of effecting change in medical practice
(Gensensway,1995).
Not only do these medicalprotocols change,organizations undergoa constant flux of employeesand restructuring of responsibilities. Eachtime a changeoccurs, the
modelbecomesout of date, and can no longer accurately
predict the organization’s performance. Updatingthe
organization modelforces the modelbuilders to constantly accommodate
for changes in the organizational
and process models. To update the workprocess, many
experts must be broughttogether---experts whocreated
the original workprocess, experts whounderstand the
organizational changes, and experts whounderstandthe
modelingrequirements.This task can be difficult, if not
impossible,and needsto be repeatedeach time a significant change occurs. The need to accommodate
changes
in the modellimits the reusability of modeldescriptions--the incrementalworkto modifyan existing model
maybe morethan the cost of modelingthe neworganization fromscratch.
There has been recent work in generating reusable
work-processdescriptions that can be shared amongdifferent organizations (Maloneet al, 1993). Thesereusable work-processdescriptionsare intendedto be used as
the building blocks for modelingexisting organizations
or for creating neworganizations. Whereasthese efforts
are beginningto standardizerepresentationsof processes
(Leeet al, 1994),theystill requiresignificantexpertise
modeling, and a clear understanding of the domainof
interest. Theselibraries of work-processdescriptionsdo
not solve the problemof providingthe neededexpertise.
Themodelbuilder is still faced with the dauntingtask of
maintaining both the organizational and process informationat a sufficient level of detail for simulationand
workflowmanagement.
Our work has focused on improving the methods of
acquiring, maintainingand customizingthese workprocess descriptions.In this paper, wedescribean alternative
wayof creating detailed, customizedorganization descriptions. Our methoddivides the work of knowledge
acquisition amongthe domainexperts, applies transformation operators to the work process description, and
brings thembacktogetherusing the Prot6g6suite of tools
to generatea cohesivemodelof both the organizationand
the workprocess.
Prot6g6
TheProteg6suite of tools providesa methodology
for the
construction of knowledge-based
systemsand knowledgeacquisition (KA)tools (Eriksson et al, 1995). These
tools are generatedby the Prot6geenvironment,basedon
a modelof the domaincreated by a knowledgeengineer.
Becausethese tools are domain-specific,they are easy to
41
use by domain experts who maybe unfamiliar with
knowledge
base representationissues.
In the area of organizational work processes, the
knowledgebase contains informationabout the workflow
of an organization,or informationabouta single process,
such as a specific medicalcare guideline, within an organization. For Prot6g6to construct an appropriate KAtool, an expert in the area of simulation and workflow
managementmust build an appropriate domain model
that captures the distinctions and terminologyneeds of
the simulation systemor workflowmanager.Prot6g~uses
this domainmodelto generate a KA-toolthat could be
used by domainexperts to build a knowledgebase about
a particular organizationor organizationalworkprocess.
TheProteg6approachis well-suited for domainswhere
the knowledge
content is dynamic.Thus, if the description of the workflowchanges, the domainexpert can
easily modifythe knowledge
base to reflect this change.
Likewise,if the organizationchanges,or evenif the underlying modelof the organizationchanges,Prot6ge can
rapidly create newKA-tools or knowledgebases that
reflect these changes. However,becausethe generated
tools are based on a common
ontologyof terms, they can
remaincoordinatedin the face of these changes.
Medical Process Descriptions
Early workwith the Prot6g¢environmenthas beenin the
constructionof knowlodge-acquisition
tools for populating knowledge
bases in medicine.Recently,Tuet al (Tu,
1995,1996), haveused Prot6g6to assist in the acquisition of protocols for patient care. Theseprotocols describe the steps necessaryto care for patients witha particular problemand are examplesof a processdescription
specific to medicine.In medicine, protocols, clinical
pathways,and clinical guidelines are examplesof medical workprocessesthat havebeencreated with the goal
to improvethe efficiency and quality of medical care
(Lobach & Hammond,
1994).
Although protocols can improve the efficiency and
quality of patient care whenthey are used, they suffer
from manyof the same problemsthat detailed process
descriptions have. First, goodmedicalprotocols are expensive to create. Mostare created by medicalexperts
and basedon extensive reviewof the medicalliterature,
case-controlledclinical trials, and consensusstatements
of national organizations. The expenseand complexity
of literature reviews,clinical trials, andconsensusmeetings motivates guideline authors to share protocols
amongdifferent institutions so that others can take advantageof their work.It is difficult however,
for creators
of nationalprotocolsto anticipateall the possiblecontingenciesthat a specific organizationmightrequire. Often
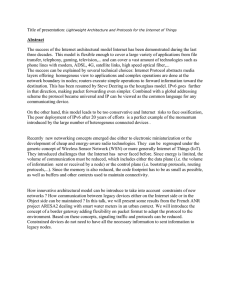
Generic
Guideline
Site-Specific
Guideline
quirements of a particular simulation system. People
skilled in simulation techniques must be certain that the
information they require from the organization and
medical experts for the purposes of simulation is included
in the final model.
Thus, to create models of organizations suitable for
simulation or workflowapplications, three areas of expertise must be brought together: This process of creating medical protocols for simulations is shownin Figure
1. Medical experts whocreate the process descriptions,
organization experts who mapthese process descriptions
to the organization activities that accomplishthe goals of
the protocols, and model builders who understand the
requirements of the simulations or workfiow systems
must be coordinated to create an accurate organization
model. Before accurate models of medical organizations
can be constructed, tools that assist in bringing together
expertise in these three areas must be developed.
Organization
Characteristics
Simulation
Ch~~racteristics
Guideline
Simulation
FigureI. Theprocess of creating protocol models.Process modelsrequire modificationsfor bothorganizational
and simulationcharacteristics
MakingGeneric Protocols Site Specific
this situation leads to protocols that are broad in their
recommendations,so institutions have the flexibility to
change and adapt a national protocol for use within a
particular institution.
Although underspecified protocols make it easier for
these protocols to be shared, these high-level process
descriptions are inadequate for simulations or workflow
systems. A generic medical protocol might suggest a
goal condition to be achieved, but not specify howthat
goal should be achieved within an organization. The
protocol might suggest an alternative that does not exist
within that organization, or one for which there are
cheaper, organization-specific alternatives.
A clinic director, familiar with the resources and skills
of the organization, is responsible for taking a national
protocol for patient care and adapting it for the particular
resources of that organization. Thus, the experts who
create the process description are often not the sameones
who are charged with customizing the protocol for an
organization, or modelingit for the purposes of simulation or workflow. At most institutions, it is a long and
difficult process of committee meetings to customize a
national protocol for use within a particular setting. As
with other process descriptions,
when new medical
knowledgebecomesavailable or when there is a change
in the wayin which medical care is delivered, the protocols are no longer accurate.
Even organization-specific protocols may not be adequate for simulations or workflow systems. Adding detail of routing or verifying processes and timing events
maybe required for a simulation. Organization experts
and medical experts may not have expertise in the re-
To assist the coordination of these experts in creating
accurate organizational models, we have used the Prot6ge
system to create a series of customized knowledgeacquisition tools, suitable for use by each of these experts.
Wehave entered a protocol used at the Stanford University Bone Marrow Transplantation Clinic into these
knowledge-acquisition tools and are extending this
framework to provide additional computer support for
protocol specialization.
The Stanford Bone Marrow Transplantation
(BMT)
Clinic has recently adapted a series of inpatient medical
protocols for patient care for use in an outpatient setting.
These protocols were initially drawnfrom formal clinical
trials, and were meantto be used in an inpatient setting.
However,two changes have occurred within the clinic.
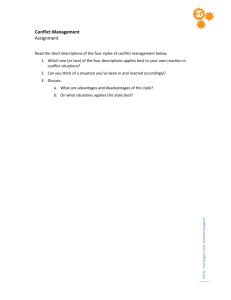
i i""~ Pa~Oata
[~Pe~zck~
Pdicie~
[ ~..~1 $=_..._aprplk’,me~aLIdaic~alE~5~:]l~Re,oum~
Re=ounce
iO p~m
I~!1/
Figure 2. The Proteg6ontology editor with the BMT
organizationontology.The le~ panel showsthe terms
usedin the model,and the right showsthe details of
the term Organization.
42
First, advances in medical care have madenew therapies
possible, simplifying the process of giving chemotherapy
and bone marrowcells. Second, pressures to control the
cost of expensive procedures have encouraged organizations to moveinpatient therapies to an outpatient setting.
Because of these changes in both the process of giving
care and in the organizational structure, the Stanford
BMTclinic has modified a collection of protocols for use
in the outpatient setting. Wehave used their lung cancer
protocol as an example of the changes that occur when
work process descriptions must be changed because of
changesin the structure of the organization.
Weused three knowledge-acquisition tools in our
prototype system the first was provided by the Prot6ge
environment, and the other two generated by Proteg6.
The first tool, the ontology editor allows modelbuilders
to define the information required by the simulation or
workflowsystem. Figure 2 is a snapshot of the ontology
editor with part of the BMTorganization ontology. The
ontology provides the terms needed for a simulation or
workflowdescription, and the relationships amongthese
terms. For our organization model, we used a common
ontology extended to include each of the different knowledge-acquisition tools that we created. This provides an
underlying commonrepresentation which facilitates
bringing together several areas of expertise in a cohesive
manner.
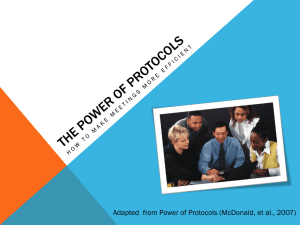
Another tool, shown in Figure 3a, provides the
mechanismto enter a generic protocol. This sharable
protocol requires additional information including intentions, goals, and requirements, not typically present in
generic protocols. This richer representation allows the
Screena:
Screenb:
Figure3. Screena showsthe generic KAtool displaying the BMT
protocol prior to modification.
Screen b showsthe CAMINO
tool, displaying the BMT
protocol, nowmodifiedfor the Stanford BMT
outpatient
clinic. Theactivity StagingandWorkup
in Screena has beenexpandedinto the first 2 columnsin Screenb.
experts whocreate these generic protocol to provide additional guidanceto organizationexperts in mappingthe
generictasks to the organization.
Finally, we created a tool, CAMINO,
whichprovides
assistanceto the organizationalexpert in (1) creatingand
maintaininga description of the resources, tasks, and
skills within their organization, and (2) providing
editing environmentto assist organizational experts in
mapping
these generic processdescriptions to the organizational tasks that will accomplish
these goals or intentions. In Figure3, weshowa portion of a generic guideline anda site-specific guideline. Thegeneric activity
"Staging and Workup"in Figure 3a is expandedinto a
series of site-specific tasks in the site-specific guideline
in Figure3b. Additionalactivities that satisfy insurance
verification requirementsof the organizationhavebeen
addedafter the "BeginProtocol" step, and are shownin
the left-hand side of Figure3b. At present, possiblemappings into the organizationare chosenfroma pick list of
organizational activities, but wehave defined a set of
transformationoperators, described below, that should
provideadditional computer-based
supportfor intelligent
mappingof generic processdescriptions to organizationspecific activities. Thiswill be particularly importantin
maintainingaccurate processdescriptions in the face of
organizationalor processchanges.
satisfy the post-conditionsor intentions of the deleted
activity.
AggregationThe protocol mayindicate two different
activities that the organizationalwaystreats as a unit and
does not further describe sub-activities. For example,a
guideline mayindicate to checka patient’s bloodpressure and then his pulse. Theclinic protocol mayonly be
concernedthat vital signs are taken, whichinclude a
bloodpressure andpulse. Here, the generic protocol has
moredetail than is necessaryfor doingthe tasks within
the organization.
ExpansionA site-specific protocol mayrequire more
detail than that specified in the generic protocol. For
example,the protocol mayindicate that chemotherapy
shouldbe given; the site-specific protocol, however,may
specify pre-hydration requirements, monitoringtasks,
and follow-upvisits as part of the processof giving the
chemotherapy.
In this situation, the descriptionof tasks
in the organization is moredetailed than the task descriptionsin the protocol.
SubstitutionSubstitution is a combinationof addition
and deletion. Theoriginal activity is deleted, andoneor
morea~ivities are addedto the guideline For computerbasedsupportof this operator, a similarity metricmustbe
defined, and used to determinewhichtasks are suitable
alternativesto the protocoltask that is to be substituted.
For example,if the similarity metric wasbasedon activity intention, then substituted a~ivities wouldhavethe
sameunderlying intention. Other metrics mightinvolve
not only intentions, but post-conditions, skill requirements,andother activity characteristics.
Temporalreordering It should be possible to reorder
a~ivities that do not haveexplicit temporalconstraints to
be consistent with the organization’s procedures. For
example,if the protocolindicates that onetest shouldbe
doneanda seconddonebasedon the results of the first,
it maybe moreefficient for the organization(and convenientfor the patient) to do these tests at the sametime
and then to evaluate themboth simultaneously. Wedid
not see evidence of temporal reordering in the BMT
protocols, but there were muchtighter temporal constraints on the outpatient protocol than the inpatient
protocol, given the additional constraints of the outpatient clinic andstaffing limitedto businesshours.
Separating the organization modelfrom the generic
workprocess description and using explicit transformations to link the genericworkprocessdescriptionsto organization tasks has significant benefits. If there are
changeswithin the organization, only the organization
modelrequires updating--the generic workprocess description wouldnot change,and a newsite-specific protocol could be generated using this neworganization
Protocol Adaptation as Plan Revision
The transformation operators used by CAMINO
can be
described more explicitly if we view workprocess descriptions as plans that requirerevisionsto satisfy additional constraints of the organization. Moreformal descriptions of plans andrevision strategies has the advantage of providinga sharedlanguageto describe the process of customization, and makingautomatic support for
maintaining and customizingworkprocess descriptions
possible. Basedon our experience with the BMT
clinic
and other medicalprotocols, wehave defined a preliminary set of operators that can be used to modifywork
processdescriptions.
AdditionNewactivities are added to a protocol when
the additional activities satisfy an organizational requirement(checking insurance status), or an implicit
requirementof the protocol (additional testing to determineprotocoleligibility) that has not beenmadeexplicit.
DeletionActivities that are not neededto satisfy organizational or protocol constraints could be removedfrom
the protocol without damageto the revised plan. If the
organizationwasnot capable of performinga particular
activity (and therefore deletedit fromthe workprocess),
anotheractivity wouldneedto be substituted that could
44
model. Conversely, if the generic protocol were to
change, a new site-specific protocol could be generated
using the new intentions and sites within the organization that support those intentions. In this framework,the
authors of the generic protocols maintain separately their
protocol from those activities in the organization model,
but can be linked through the transformation operators.
This makesit easier for individuals whounderstand the
details of the organizationactivities to enter those activities directly, and have another person whounderstands
the overall process arrange those activities in a way that
satisfies both work process and organizational constraints.
patient care, the effort needed to makethese modelsaccurate may prevent more widespread use. Protege provides a wayfor a modelbuilder to define the features that
are important to represent for the purposes of a simulation or workflowsystem, and to use these features to create customized knowledge-acquisition tools suitable for
use by domain experts. Wehave shown that this is an
appropriate tool to use for modeling medical organizations, and can be used to coordinate the transformation of
a generic protocol to a site-specific protocol based on a
generic protocol and a description of an organization. By
distributing the responsibility for maintainingthe organization model amongthe experts within the organization,
complex, models of the organization can be created and
maintained, without the need for one person to be expert
in all areas. It is hoped that these complexmodelswill
give organizations the opportunity to examinethe procedural knowledgestored in their organizations, and acquire, maintain, and customize organization models-models in which the whole is better than the sum of its
parts.
Discussion
All organizational modelsrequire detailed information to
generate reliable simulations. ORenthe expertise required to create these detailed models is distributed
amongdifferent people who may not be located in the
same place. In medicine, this problem is even more
acute: Workprocess descriptions are often created by
national consensus meetings, and it is the responsibility
of the local organization to adapt these protocols for use
within their owninstitution.
Prot6ge provides a mechanismto coordinate the developmentof these specialized work process descriptions by
creating customized knowledge-acquisition tools that can
be used by domain experts and brought together through
a commonontology of terms. Our current research involves exploring ways of providing computer support to
the process of acquiring, maintaining and customizing
organization-specific work process descriptions. By dividing the work of maintaining complex organization
models amongexperts in work processes, organizations,
and simulation, no one person requires expertise in all
these areas to generate a detailed modelof the organization.
Weare also defining a set of valid transformations and
an explicit way of representing these changes. Wehope
that these transformations will allow better computerbased support for the process of both the initial transformation of a generic protocol to one that is site-specific,
and maintenanceof the site-specific protocol and organization models. Thus, if we have a protocol, a organization modelof activities, and a languageto describe protocol revisions, we can provide computer support to the
process of protocol modification, and maintenance.
Organization-specific models are more accurate at
predicting organization performance than generic models, but such modelsrequire significant effort to develop
and maintain. Although simulations can be used to gain
insight into howorganizational makeuphinders or helps
References
Burns JM, Tierney DK, Long GD,et al., 1995. Critical
pathway for administering high-dose chemotherapy followed by peripheral blood stem cell rescue in the outpatient setting. OncologyNursing Forum,22(8): 1219-24.
H. Eriksson, Y. Shahar, S. W. Tu, A. R. Puerta, &M. A.
Musen. 1995. Task Modeling with Reusable ProblemSolving Methods.Artificial Intelligence 79(2): 293-326.
Field, MJ, Lohr KN,eds. 1990. Clinical Practice Guidelines: Directions for a New Program. IOMreport, National AcademyPress, Washington, D.C..
GensenswayD. 1995. Putting guidelines to work-lessons
fi’om the real world. ACPObserver, 199515:(1).
Lee J, Yost G, and the PIF Working Group 1994. The
PIF Process Interchange Format and FrameworkVersion
1.0 Working Paper 180, MIT Center for Coordination
Science, Mass. Institute of Technology.
Levitt RE, CohenGP, Kunz JC et al. 1994. The "’Virtual
Design Team" Simulation HowOrganizational Structure and Information Processing Tools Affect TeamPerformance, in Computational Organization Theory, ed.
Carley KM,Prietula MJ.
Loback DF, HammondWE. 1994. Development and
evaluation of a Computer-Assisted ManagementProtocol. In Proceedings of the Symposiumon ComputerApplications in Medical Care, 787-791. Washington, DC.:
AmericanMedical Informatics Association.
/45
Malone TW, Crowston K, Lee J et al., 1993. Toward a
handbookof organizational processes In Proceedings of
the 2nd IEEE Workshop on Enabling Technologies Infrastructure for Collaborative Enterprises, Morgantown,
WV,April 20-22.
PROTI~GI~-II
to protocol-based decision support. Artificial
Intelligence in Medicine. 7(1995) 257-289.
Tu SW&. Musen MA. 1996. The EONModel of Intervention Protocols and Guidelines, In Proceedings of the
Symposiumon Computer Applications in Medical Care,
587-591. Washington, DC.: American Medical Informatics Association.
Tu SW,Eriksson H, Gennari JH, et al. 1995. Ontologybased configuration of problem-solving methods and
generation of knowlodge-acquisitiontools: application of
46