‘Silent voices’ in research with visually impaired children: ethnicity &
advertisement

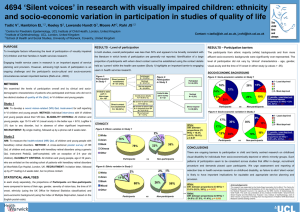
‘Silent voices’ in research with visually impaired children: ethnicity & socio-economic variation in participation in studies of quality of life Tadić V1, Hamblion EL1,2, Keeley S3, Lewando Hundt G3, Moore AT2, Rahi JS1,2 1Centre for Paediatric Epidemiology, UCL Institute of Child Health, London, United Kingdom of Ophthalmology, UCL, London, United Kingdom 3School of Health and Social Studies, University of Warwick, Coventry, United Kingdom 2Institute v.tadic@ich.ucl.ac.uk, j.rahi@ich.ucl.ac.uk PURPOSE RESULTS - Level of participation RESULTS – Participation barriers To investigate factors influencing the level of participation of visually impaired (VI) In both studies, overall participation was less than 50%, and appears to be broadly consistent with The participants from ethnic majority (white) backgrounds and from more children and their families in health services research. the literature in which levels of participation are generally not reported. Identification of a large affluent socio-economic backgrounds were significantly over-represented. The Engaging health service users in research is an important aspect of service proportion of participants with whom direct contact cannot be established using the contact details level of participation did not vary by ‘clinical’ characteristics - age, gender, planning and provision. However, achieving high levels of participation is an held as ‘current’ within the health care system (Study 1) highlights an important barrier to engaging visual acuity and the time of VI onset in either study (p values > .05). ongoing challenge and the participant’s socio-cultural and socio-economic users in health services research. circumstances remain important barriers (Rahi et al., 2003). Socio-economic background Figure 1: Participation in Study 1 METHODS Participated N = 32 (39%) Direct contact established N = 81 (76%) quality of life (QoL) in VI children and young people. Figure 5: Socio-economic variation in Invited vs. Achieved sample in Study 1 Participated N = 44 (29%) Declined N = 25 (31%) 1 - Least deprived 2 3 4 5 - Most deprived Did not respond N = 24 (30%) We examined the levels of participation overall and by clinical and sociodemographic characteristics of patients who took part in two distinct studies of Figure 2: Participation in Study 2 Invited to take part in survey N = 151 Invalid phone details N = 16 (61.5 %) 17% Declined N = 8 (5%) 23% Did not respond N = 99 (66%) 1st quintile: diff. between two proportions (CI 95%) = 0.191 (0.007 – 0.374), p = .025 Figure 6: Socio-economic variation in Invited vs. Achieved sample in Study 2 Moved abroad N = 1 (4 %) 1 - Least deprived 2 3 4 5 - Most deprived young people about their VR QoL. Eligibility criteria: All children and young people, age 10-15 with VI (visual acuity in the better eye < 6/18, LogMar ≥ .51) Recruitment: By single mailing, followed up by a phone 2 weeks later. Ethnicity White: Diff. between proportions (CI 95%) = 0.159 (0.014-0.331); p ≤ 0.09 Figure 3: Ethnic variation in Invited vs. Achieved sample in Study 1 2% 1% Study 2 6% 6% 9% 16% Aim: To measure the health-related (HR) QoL of children and young people with 63% 19% hereditary retinal disorders. Method: A cross-sectional postal survey of HR QoL White Chinese Asian Mixed Black Other Asian Other 12% 24% 1st quintile: diff. between proportions (CI 95%) = 0.147 (0.004 – 0.298), p = .030 reporting of selection bias in health services research on childhood disability, as failure to elicit 7% 2% ‘silent voices’ is likely to have important implications for equitable and appropriate service 11% Statistical analyses planning and provision. 28% 64% For each study separately, the proportions of participants in the Invited sample 80% were compared to those in Achieved sample in terms of their age, gender, White Mixed Such patterns of participation seem to be consistent across studies that differ in design, recruitment procedure and demands placed upon participants. We urge assessment and 1%1% 6% Index of Multiple Deprivation-IMD, based on the English postal code). 17% 30% visual disability for individuals from socio-economically deprived or ethnic minority groups. White Figure 4: Ethnic variation in Invited vs. Achieved sample in Study 2 2nd mailing 2-4 weeks later but no phone contact. National Statistics classification-ONS) and socio-economic background (using the 18% 17% 17% There are ongoing barriers to participation in child and family centred research on childhood are enlisted on the existing cohort of patients with hereditary retinal disorders at severity of vision loss, the time of VI onset, ethnicity (using the UK Office for 21% CONCLUSIONS instrument PedsQL (self-completed, with an exception of 2-4 year old children, N Moorfields Eye Hopital, London, UK. Recruitment: Invitation letter, followed up by 29% 1 - Least deprived 2 3 4 5 - Most deprived 15% 78% of children and young people with hereditary retinal disorders using a generic QoL = 13%). Eligibility criteria: All children and young people, age 2-18 years, who 6% 15% 25% No answer to phone calls & no response from GP N = 3 (11.5 %) children and young people . Method: Individual interviews with VI children and due to any disorder, but in absence of other significant impairments. 16% 16% No answer to phone calls N = 6 (23 %) Direct contact not established N = 26 (24%) Aim: To develop a novel vision-related (VR) QoL instrument for self reporting VI 18% 37% Invited to take part in interviews N = 107 Study 1 27% 1 - Least deprived 2 3 4 5 - Most deprived Asian Other Black White Asian Black Other White: Diff. between proportions (CI 95%) = 0.163 (0.020-0.306); p = 0.043 Asian: Diff. between proportions (CI 95%) = 0.171 (0.052-0.290), p = 0.021 This research was funded by the Guide Dogs Association for the Blind