Quality of Life of Substance Abuse Treatment Patients:
advertisement

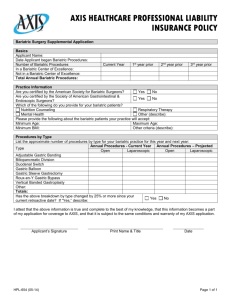
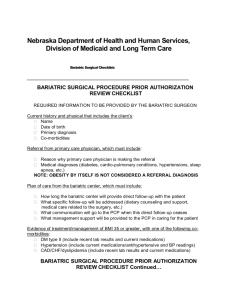
Quality of Life of Substance Abuse Treatment Patients: Post-Bariatric Surgery Cases Versus Controls Karen K. Saules, Ashley Wiedemann, Valentina Ivezaj, Summar Reslan, Daniel Wood & Lauren Skilton Eastern Michigan University, Department of Psychology Introduction Results Quality of life (QOL) among post-bariatric surgery patients is high, approximating that of healthy controls by one year postsurgery (Andami et al., 2005). Evidence from our laboratory, however, suggests that post-bariatric patients are overrepresented in substance abuse treatment programs (Saules et al., 2011). We hypothesized that QOL of post-bariatric surgery patients admitted to substance abuse treatment would be relatively poor, overall, and significantly worse than that of other substance abuse treatment patients. Relative to controls, and consistent with the bariatric treatment population in general, bariatric patients were more likely to be female (74% vs. 38%, Chi-Square (1) = 13.3, p < .001). Bariatric patients’ weight loss approximated that reported in the literature for bariatric patients in general, with a maximum pre-surgical BMI of 53.1 ± 11.2 and a mean current BMI of 32.0 ± 7.6. Bariatric patients and controls differed on BMI, with non-bariatric patients having a mean BMI of 25.3 ± 4.5, t (103) = −5.6, p <.001. BMI, however, was not significantly associated with any of the assessed dimensions of QOL. Method Post-bariatric substance abuse patients had significantly lower psychological QOL compared to non-bariatric controls, t (96) = −2.5, p <.05. As noted, bariatric patients were disproportionately female, but a linear regression model that included both gender and bariatric status indicated that it was bariatric status, and not gender, that accounted for significant variance in the prediction of Psychological QOL. Bariatric cases and controls did not differ on anxiety or depression scores, but bariatric patients were much more likely to have histories of physical (65% vs. 32%, p < .01), emotional (70% vs. 38%, p < .05), and sexual abuse (61% vs. 25%, p < .01). Abuse history, however, was not significantly related to Psychological QOL. PARTICIPANTS/PROCEDURES: The sample included 42 postbariatric patients and 56 controls, all recruited from an inpatient substance abuse treatment program. Bariatric patients were identified during the admission history and physical. All nonbariatric patients were eligible to serve as controls, and those who volunteered are included here. Overall, the sample had a mean age of 43.4 ± 11.9 years and a mean education level of 14.1 ± 2.2 years, neither of which differed as a function of bariatric status. MEASURES: The WHOQOL-BREF (Murphy, Herrman, Hawthorne, Pinzone, Evert, 2000) is a 26-item measure developed by the World Health Organization (1996) to assess quality of life (QOL) in four domains: (1) Physical, (2) Psychological, (3) Social, and (4) Environmental. In addition, the first two WHOQOL-BREF are examined separately: Item 1 asks about the individual’s overall perception of QOL, and Item 2 asks about the individual’s overall perception of his/her health. The Patient Health Questionnaire (PHQ) was used to assess depression and anxiety (Spitzer, Kroenke, & Williams, 1999) Body Mass Index (BMI) was obtained from the medical record for all patients, although pre-surgical BMI for the bariatric patients was obtained from self-report. 5 Quality of Life for Substance Abuse Treatment Patients: Post-Bariatric Cases vs. Controls 20 * 15 14.1 12.9 13.9 13.3 12.2 12.1 Bariatric Control 11.3 10.5 10 5 0 Physical Psychological Social Environmental Presented at the 2011 Annual Meeting of the Society of Behavioral Medicine Psychological Quality of Life for Substance Abuse Treatment Patients: Meant Item Scores for Post-Bariatric Cases vs. Controls Bariatric 4 * * 3.3 3.2 3 2.8 Control 3.1 2.8 2.9 2.9 * * 2.8 2.8 2.3 2.7 2.3 2 1 0 Enjoy Life Meaningful Able to Appearance Satisfied with Life Concentrate Acceptance Self Positive Mood The mean score for each item that comprises the Psychological QOL scale is shown above, as a function of bariatric status. Discussion Results suggest that bariatric patients who experience post-surgical substance use disorders of the magnitude warranting inpatient treatment have low overall QOL. Hawthorne et al. (2006) present WHOQOL-BREF community norms that, when transformed for the 420 scoring metric used in this report, correspond to norms of 15.5 for Physical, 15 for Psychological, 15 for Social, and 31.5 for Environmental QOL, all of which are high by comparison to the present sample. In the Psychological domain, however, bariatric patients’ QOL was significantly lower than the already low scores observed for control substance abuse cases. Furthermore, the low QOL is not simply a function of dissatisfaction over bodily appearance. While not directly related to QOL, bariatric patients had strong histories of physical, emotional, and sexual abuse. Future research should evaluate whether a history of physical, emotional, and/or sexual abuse elevates risk for development of substance use disorders after bariatric surgery. Quality of Life of Substance Abuse Treatment Patients: Post-Bariatric Surgery Cases Versus Controls Karen K. Saules, Ashley Wiedemann, Valentina Ivezaj, Summar Reslan, Daniel Wood & Lauren Skilton Eastern Michigan University, Department of Psychology References Adami, G.F., Ramberti, G., Weiss, A., Carlini, F., Murelli, F., & Scopinaro, N. (2005). Quality of life in obese subjects following biliopancreatic diversion. Behav Med. 31(2), 53-60. Hawthorne, G., Herrman, H., & Murphy, B. (2000). Interpreting the WHOQOL-BREF: Preliminary population norms and effect sizes. Social Indicators Research, 77, 37-59. Murphy, B., Herrman, H., Hawthorne, G., Pinzone, T., Evert, H. (2000). Australian WHOQoL instruments: User’s manual and interpretation guide. Australian WHOQoL Field Study Centre, Melbourne, Australia. Spitzer, R.L., Kroenke, K., & Williams, J.B.W. (1999). Validation and utility of a self-report version of PRIME-MD; The PHQ Primary Care Study. Journal of the American Medical Association, 282, 1737-1744. Contact: ksaules@emich.edu