In-Home Care Planning Committee Members

In-Home Care Planning Committee
Members
*Tim Bulson
Matthew N. Denenberg, MD, FACEP, FAAP
Spectrum Health Research Department
Helen DeVos Children’s Hospital
Cyntha Hunter, RN
Connie Maxim, EMT-P
Jo Meyer
Al Nieboer
Pamela Ronning
Eric Smith
Michelle Thompson
*Committee chair
Ravenna Public Schools
Region 6 Bio Defense Network Coalition
Central Michigan Home Care
Gerber Memorial Health Services
Grand Valley State University
Reel Response Solutions, LLC
Metropolitan Medical Response System
Objectives
Primary Objective: Describe how home health care agencies and services will be integrated into an overall pandemic response plan.
Secondary Objective: Develop a plan to outline how these recommendations will be based on a combination of in home care and home care agency models to provide meaningful health care services during a community pandemic response.
Assumptions
1) As a result of pandemic and the ensuing long-term medical surge, there will be altered EMS vehicle licensing standards, leading to altered EMS personnel staffing for both emergent and non-emergent transports.
2) Home care agencies will suffer the same level of absenteeism as other health care agencies, while demand for service will not change, or may increase.
3) One result of this project is that the Pre-ED Triage Committee will provide EMS and 911 medical dispatchers with triage cards (or a similar device) that will direct their response to callers who have or suspect they have the flu vs. a life-threatening condition that warrants
EMS transport. This mechanism will determine which patients meet the criteria for immediate or delayed EMS service vs. those advised to remain at home. Those who are deemed homebound will be likely become eligible for resources of this plan.
4) This committee’s outcome / plans will describe one option for how communities can provide basic medical support and links to basic life needs (e.g. food, water and fuel) to residents in their homes.
5) Primary care systems will rely heavily on public communications models to instruct patients where and how to seek treatment for the flu.
6) The region, if not the state, will use the Modular Emergency Medical System (MEMS) model to allow for surge considerations and to therefore open an Acute Care Site (ACS) to cohort patients. Similarly, the overall regional plan will define sites to transfer patients whose illness
(flu) has progressed; such placement will be articulated by the approved triage criteria and
Caring for the Community | preparing for an influenza pandemic 1
overall regional plan. This is in accord with the MEMS overview that allows each region to define the mechanisms, roles and responsibilities for MEMS activation.
7) Accessibility to basic health care (e.g. hospitals, clinics and physician offices) will exist at some level, no matter the level of pandemic flu, e.g. minimum community standards. Altered minimum standards will enhance the need for in-home care services.
8) Traditional home care service agencies will suffer the same effects as other health care agencies, e.g. higher demand, lower staffing, and the need to work in tandem with others to meet not only the demands of their clients, but of others who, because of the pandemic, will request in-home care.
Background and Need
Beyond the need to meet a clearly stated CDC objective for in-home care as part of the pandemic flu planning process, this committee agrees with assumptions made by Region 6 pandemic planning committees and similar organizations that have said some level of in-home care plans must be developed as part of overall pandemic planning efforts; this is the overarching assumption from which the committee worked.
The Outpatient and In-Home Care Plan will be specifically designed to help support patients / residents who are homebound due to one or more of these conditions:
They are denied immediate or delayed EMS response because their condition is not acute enough, but need some level of triage or medical oversight due to flu or flu-like illness.
Are already home care recipients who need continued support for a chronic medical condition.
Have an illness or social/economic condition that prevents them from getting basic life-sustaining resources (e.g. a kidney dialysis patient or frail elderly person) or are unable to drive or get transportation to resources.
Otherwise demonstrate a valid need to have designated providers (e.g. medical or support teams) determine whether some measure of health care resources / life sustaining resources that can / should be provided to them at home via the local emergency management program.
Are looking for links and support to their education system, particularly families with elementary and middle school children.
This committee suggests the implementation steps associated with this plan will be described in the
Region 6 Pandemic Flu Plan, which will also identify a “pre-emergency department triage matrix” that will articulate community-accepted, alternate standards of care and references to this Outpatient and In-Home
Care Plan. The broad Region 6 plan will articulate levels of response (with increasing levels of pandemic threat, i.e. A, B, C, etc.) and that the plan this committee develops would be activated at regional “Level C.”
(See the Pre-E.D. Triage Matrix for further detail.)
This committee assumes that at Level A, the plan will be widely circulated to all providers for its assimilation and understanding; at Level B the Region will be ready to implement the in-home care portion of the plan: at Level C there will be a state-declared disaster and the in-home care plan will be fully implemented.
Committee members brought significant and varied background and experience to this project:
Eric Smith is an EMT-P– EMS in rural Mid-Michigan with experience in planning for and with emergency management.
Caring for the Community | preparing for an influenza pandemic 2
Connie Maxim is an EMT-P Project Coordinator with vast experience working with local, regional and state response partners; she also brought EMS staff experience, from a regional level. She has experience in the nexus of this grant.
Matt Dennenberg is an MD with extensive clinical and administrative expertise in Emergency
Department care and case management in an urban setting.
Al Nieboer is a Nurse Practitioner with many years experience in practice in a rural health clinic and in a physician’s office setting as a mid level provider.
Jo Meyer is a Licensed Medical Social Worker who has worked with home health care agencies in a county with significant tribal relations and college campus settings. She also has experience in community mental health settings.
Cyntha Hunter is a Registered Nurse who has worked in public schools, nursing homes and long term care settings and has been involved in intake, education and case management work.
Pamela Ronning, BSN, MPA has 15 years of public health experience and 10 years in nursing education, and has been involved in health district and university settings.
Tim Bulson has more than 15 years of communications experience and served as the Region 6
Coordinator for more than five years. He was also a co-author of the CDC grant funding this project.
Michelle Thompson has a human resources background and extensive experience from an MMRS program management and planning perspective.
Published, relevant background literature: Helpful data and published articles supporting the work of this committee include 2007 Centers for Disease Control (CDC) planning documents focused on community strategies for pandemic influenza mitigation. One of the central topics is the early use of nonpharmaceutical interventions (NPI) as a way to limit spread of the disease. Of particular relevance to this committee is the CDC rationale that NPI may help reduce influenza transmission by reducing contact between sick persons and uninfected persons. Reducing the number of persons infected will also lessen the need for health care services and minimize the impact of a pandemic on the economy and society
(CDC, p. 23). This committee defines the provision of in-home care - e.g. health check, link to food or other basic resources – as an NPI.
This same CDC document also lists a long series of concerns for planners, including a reminder to consider in their planning vulnerable populations (e.g. people who are living alone, the poor or working poor, elderly and particularly those who are homebound, homeless, recent immigrants, disabled, institutionalized or incarcerated). The CDC lists accompanying statistics about many of these populations, outlining the potential detrimental national impact if they are left on their own during a pandemic. The concluding paragraph is most germane to this committee’s work: “Communities will need to plan for how these vital supports can continue both for this population as well as for other groups with unique physical and mental challenges in light of efforts to protect lives and limit the spread of disease,” (CDC, p. 53).
Another support for the overall goal of this portion of the Region 6 plan a recommendation in an Agency for
Healthcare Research and Quality (AHRQ) planning guide for Mass Medical Care with Scarce Resources :
“It is important for community planners to highlight the concept of the home as a ‘safe haven’ in their risk communication strategies and develop measures to support this concept. Emergency planners, therefore, must incorporate the likelihood of home care delivery in all aspects of their planning efforts. This planning must focus on the possibility that some rudimentary degree of medical care will be needed,” (Phillips, p.
49).
Further specific home care planning guidance comes from the U.S. Department of Health and Human
Services “ Home Health Care Services Pandemic Influenza Planning Checklist ,” with a series of
Caring for the Community | preparing for an influenza pandemic 3
recommendations that meet committee objectives. HHS recommends a plan for the management of patients during a pandemic, which covers the following issues:
Plans have been developed to manage patient care during the height of a pandemic to accommodate the increased number of patients who will need home care services.
The scope of services that the agency will provide and those that will be denied or referred to other providers has been clearly defined.
The role and responsibility of the agency regarding distribution of infection control supplies (e.g., masks, hand hygiene materials), food, medications, and other necessities in the home to patients and their families has been discussed with a local or regional pandemic influenza planning group.
Plans include decision tools for determining which patients can have altered service schedules based on their health conditions, needs, and available resources.
Local plans and criteria for the disposition of patients have been discussed with area hospitals and other home care agencies. (Hospitals may discharge patients to home and home health care agencies early to free-up bed space for critically ill patients.)
The plan considers how social service agencies (e.g., Red Cross, Salvation Army) will help meet the needs of families in the community (e.g., by providing child- or elder-care meals, shopping services) in homes where there are patients with pandemic influenza, particularly where the primary adult support person living in the home is ill.
The plan considers how the agency will maintain a database of clients who require electricallydependent technology-driven care (e.g., ventilators, breathing treatments, suction, pumps, turning devices), oxygen, special nutrition requirements, dialysis, etc.
This HHS checklist also provides suggestions for home care agency supply stockpiles, contingency plans for supplies and staff shortages, and to engage all local planning partners in pre-pandemic work.
The Committee Process
Approach toward objectives : Committee members began with an “ideal scenario” they believed would provide the maximum in-home medical care and other resources (e.g. basic medical interventions, links to schools for families with children, links to community resources for the elderly, and delivered meals). While optimal, it included cost- and staff-prohibited options, particularly automatic visits to entire communities.
Acknowledging these drawbacks, the group pared down its optimal plan, while keeping an eye on the benchmark grant goal of providing some measure of in-home care and inclusion of home care agencies and their needs. The committee reached consensus on a pragmatic plan that does not appear to exceed
Region 6 resource availability, includes medically sound objectives and meets CDC requirements.
Tough Decisions : As the committee moved from an ideal to a pragmatic plan, the group used extended discussions to reach consensus. Specific “tough topics” included:
How to provide at least minimal resources to as many people as possible despite limited resources
How to define reasonable minimums for care and basic life needs
How to schedule home visits even before a resident(s) may request one
The need to understand and meet racial, ethnic, language and similar needs of large population groups with few staff
The need for security and safety of those who will provide care in homes, taking into account the wide geography in the region (e.g. from concentrated urban to very rural)
A need to seek advice and clarification on providing care to illegal aliens and urban homeless populations
Caring for the Community | preparing for an influenza pandemic 4
Ultimate Process : Overall, this committee followed a series of written objectives it defined in its first two meetings. The process generally follows this outline and the accompanying diagram:
Overall Goal: Commit to designing an operations plan that would provide for basic in-home care needs for those who demonstrate a need. The final plan includes these minimally required operational priorities to work:
The plan will function best if it uses already recognized functional or geographic areas as its framework, namely school districts within an area(s) experiencing a pandemic.
This is supported by an AHRQ suggestion that a community can maximize EMS transport capability by considering “Non-critical calls should be batched by geographic area,” (Phillips, p. 47). The committee recommends using school districts as the geographic model for this plan because:
1) Most Michigan residents can identify the school district they live in.
2) School districts already have buses, bus routes and drivers that would support the committee’s team concept.
3) School districts have already formed databases with family demographics and other baseline resident information.
4) They provide well-equipped facilities from which to work, e.g. computers, office equipment, telephones and other communications, cafeterias and other support systems.
To be operational and functional, success in home care will require an overarching combined Call
Center / Base of Operations from which a command and control system will support the teams that would provide the identified essential functions to people who meet appropriate criteria. This is also supported by Phillips (p. 47) and one of his rationales designed to lessen the EMS dispatch burden in a crisis: “Call screening strategies should be in place to determine the level of urgency required to respond to calls.” The committee recommends that call centers be established for large geographic areas (e.g. one or more counties encompassing multiple school districts) and that functional operations bases from which teams will work be established within these areas, perhaps one base per school district. Each base would support at least one medical team and one nonmedical team. Teams would be dispatched to homes according to a schedule determined by calls triaged by the call center.
This committee recommends that the community support a Base of Operations to then provide command and control for these detailed levels of the plan: o Support In Home Care Teams Dispatched as needed
Medical teams (Page 1 & 2) that require
• Go Kits/Supply Packs to complete their mission
• Communications with each other and the Operations Base
• Minimum of 2 members per team, plus a driver o At Least 1 RN or Paramedic o Second Person Medically trained / licensed, if possible
Non-Medical Teams (Page 1) that require
• Go Kits/Supply Packs to complete their mission
• Communications with each other and the Operations Base
• Educational person
• Nutritional person
• Minimum of 2 persons on a team; one to drive
Safety/Security of Teams
Caring for the Community | preparing for an influenza pandemic 5
• As noted, no team has less than 2 persons
• Continual communications with each other and operations base
• Pre-determined schedule and ongoing Call Center Communications links o Supplies/Equipment for Operations Base
Electronic equipment; e.g. communications, command and control
Office equipment
Supplies on the supply sheet (TBD)
Educational information for call staff and teams
Nutritional needs o Staffing for Call Centers
RNs to answer phones or be available to talk with call taker
24-hour coverage
Physician contact 24 Hours (e.g. serve as a resource for RNs) o Duties of Call Center staff
Call reception
Telephone triage
Clerical
Confidentiality
Telephone education
Restocking supply kits
Planning/scheduling o Supplies , to include
Food and water
Secure supplies
Secure forms o Forms
Household assessment
Individual medical evaluation
Reimbursement forms o Transportation
Private vehicle
• 2-person team
• Supplies/forms, etc
Included in the above outline of minimum steps, under the heading “forms,” is the implied need to collect pertinent data points each time a medical team visits a home. This committee recommends using, or minimally modifying, existing home health care agency forms, to use what is familiar whenever possible and to minimize any need to create new forms.
One AHRQ publication written to outline patient tracking system options notes there are already a number of common data that home health care agencies collect on new clients; this list may be the nexus for data points tracked and updated in this plan. The AHRQ list shows:
Upon admission to the HHA, a nurse consults with physicians to create a written plan of care. Data elements include:
Name
Date of birth
Social Security number
Caring for the Community | preparing for an influenza pandemic 6
Payer/insurance (if any) and insurance policy number
Family contacts/next of kin/emergency contact
Demographics
Physician name
Physical capabilities and assistance needed with activities of daily living
Care regimen and duration
This intake information could be considered a census of patients for each HHA, and could be adapted to feed into a national patient tracking system. (AHRQ p. 59) Though this AHRQ recommendation was specific to tracking home health care patients during a forced evacuation, the data points and suggestion they feed into a local or regional tracking system is as logical as the AHRQ recommendation that this information be fed into a national patient tracking system used during evacuations.
The Conclusion
Objectives and detailed description of final report
The committee’s overall conclusion is:
That a plan to use existing geography and infrastructure, particularly school districts, as a framework on which to build an in-home and outpatient care system can work. The system will require three key tiers:
Local or regional call centers residents will use to express their needs
Call centers supported by operations centers, with a minimum number established per school district
Medical and non-medical teams based at the operations centers to complete home visits o Both teams will evaluate residents for needs and use pre-determined algorithms to provide service or make further referrals o All data compiled by each team will be centralized at the operations center and shared with the call center and the appropriate EOCs
This is supported by Phillips, who lists one of the key steps to managing a mass casualty event is the
“Facilitation of home-based care for patients in cooperation with public health and home care agencies,” (p.
65). Further work should be done to meet the objectives set here, and to expand as needed to meet pandemic-specific recommendations found in Phillips’ work, outlined as:
Address the myriad challenges of providing health care services in the home setting to people with substantial disability and/or an established illness or without family or other resources to provide care. Community planners should consider the following issues related to providing care in the home setting:
Develop alternative ways to provide care to people in the community such as primary care vans that go into neighborhoods to provide care, answer questions, and provide resources.
Establish telephone hotlines to answer questions regarding the avian flu virus, such as using “Ask-A-Nurse”-type telephone support services and make use of existing hotlines.
(Phillips, p. 138)
Caring for the Community | preparing for an influenza pandemic 7
Supporting Documents
Appendix 1 .............................................................Flu Related In Home Medical Care Scope of Services
Appendix 2 ..........................................................................Home Team Medical Supplies and Equipment
Appendix 3 ............................................................................................................Pan Flu Medical Go Pack
Appendix 4 ........................................................................Home Health Care Services - Routine Supplies
Appendix 5 ............................................................................... Home Health Care - Non-Routine Supplies
Appendix 6 .........Centers for Disease Control Interim Recommendations with In-Home Use Guidelines
Appendix 7 ..........................................CDC Recommendations Facemask Use to Prevent Transmission
Appendix 8 ....................................................................................................... Home Care Planning Issues
Appendix 9 .............................................................................Pandemic Flu Household Assessment Form
Appendix 10 ....................................................................................................Individual Medical Evaluation
Appendix 11 ....................................................................................................................Schematic Diagram
Appendix 12 ................................................................................................................................. References
Caring for the Community | preparing for an influenza pandemic 8
Appendix 1
Spectrum Health CDC Pan Flu Grant:
Outpatient Care Planning Committee
Flu Related In Home Medical Care Scope of Services
Medical team will provide a brief medical exam, per design, of sick household members
Will provide basic Flu Medical Education o Educational referrals to www.panflu.gov
, www.cdc.gov
, www.ready.gov o Educational materials provided to patient, as prepared by appropriate local health district,
Michigan Department of Community Health, or other local governing body
Symptom Relief o Fever control with acetaminophen and ibuprofen o Flu related and Benign Pain control with acetaminophen and ibuprofen o Education about over the counter(OTC) medication
Hydration o Oral Rehydration
Proven effective and underutilized
Oral Hydration and nutrition advice and encouragement
Antiemetic use followed with oral hydration education
• Household fluids i.e., juice, soda pop, milk, etc.
• World Health Organization oral rehydration “recipe” o Oral rehydration salt packs contained in “Go Pack” o Intravenous Hydration
IV fluids
• Limit to two liters per adult
• Limit two calculated boluses for children, based on the professional discretion and expertise of the provider
• Dextrose for hypoglycemic patients, especially diabetic persons
Antiemetics to control emesis and allow for continue home oral hydration
• Adult dosing for promethazine and Ondansetron
• Pediatric dosing for promethazine and Ondansetron
• No promethazine under two years of age o Subcutaneous Hydration
Potentially implemented as new technology evolves
Respiratory care o Trial of bronchodilator for wheezing patients greater than 12 months
Albuterol MDI with spacer
• Limit to two puffs 20 minutes apart o Leave inhaler with patient if it achieves desired effect
Post in-home care o Assist to expedite higher level of care if patient fails or is too ill for in-home care o Communicate with patient and operations to convey need for further visits and non medical assistance o Assist patient with primary care communication o Educate patient about non-medical needs resources
Caring for the Community | preparing for an influenza pandemic 9
Appendix 2
Spectrum Heath CDC Pan Flu Grant:
Outpatient Care Planning Committee
Home Team Medical Supplies and Equipment
Equipment o Stethoscope
Personal
Disposable if personal not available o BP cuff o Thermometers, disposable or reusable with covers o Pulse ox o Glucose meter device
Lancets
Test strips
Medical Supplies o Gauze pads 4 x 4 o Bandages o Tape o Alcohol swabs
Personal Protection Devices o Latex-free gloves o Masks, with level of protection to match threat o Gowns, should be disposable and imperviable o Sharps containers, one small per team o Medical waste containers, one small per team o Hand sanitizer o Hand soap, medical grade
Individual medical evaluation forms
Clerical supplies o Pens o Notepads o Clipboard o Locking/secure document container for HIPPA compliance o Paperclips/rubber bands o Waste container for document requiring shredding/secure destruction
Caring for the Community | preparing for an influenza pandemic 10
Appendix 3
Spectrum Health CDC Pan Flu Grant:
Outpatient Care Planning Committee
Pan Flu Medical Go Pack©
Water resistant bag with multiple compartments, external pockets for IV fluid bags.
Labeled as: “Pan Flu Medical Go Pack©”
IV Start supplies
Intravenous (IV) start kit, latex-free with tegaderm dressing o 1- tegaderm iv dressing (6cm x 7cm) 10 per bag, 1- impermeable drape, 2- 2 inches x 2 inches gauze sponges, 2- alcohol wipes, 1- pvp-iodine prep, 1- latex-free tourniquet, 1- transpore' tape (36 Inches), 1- i.d. label o Various angiocaths
20G x 1" IV, 10 per bag
22G x 1” IV, 10 per bag
24G x ¾ ” IV, 10 per bag
IVF o IV extension sets, 10 per bag o .9 NS(Normal Saline) 1000 ml bags
Two liters per go bag
Case of 24 in vehicle to be replenished to “Go Bags” as needed o 5% Dextrose .9 NS(Normal Saline) 500 ml bag
One bag per go bag
Five extra in vehicle
Medications
Antipyretics o Acetaminophen extra strength tablets (500 mg x 2) individual dose packs, 10 per bag o Ibuprofen tablet (200 mg) individual dose packs, 10 per bag o Acetaminophen liquid (160 mg/5ml, 10 ml) individual dose pack, 5 per pack
Antiemetic o Phenegran
Tablets (25 mg), 10 per bag
Rectal suppositories (25 mg) 5 per bag o Ondansetron
Oral dissolving tablet (4 mg), 5 per bag
25% Dextrose Solution o 25-gram ampoules, 2 per bag o Oral glucose gel, 15 g tubes, 2 per bag
Bronchodilators o Albuterol
Metered dose inhaler with spacers, 3 per bag
Oral rehydration salts (ORS) packs, 10 per bag
Lubricating jelly, individual packs, 5 per pack
Caring for the Community | preparing for an influenza pandemic 11
Appendix 4
SH CDC Pan Flu Grant:
Outpatient Care Planning Committee
Home Health Care Services
Routine Supplies
Item Medicare Number
Accu Check Test Strips
Aloe Vesta Prot Oint
Applicator Non-Sterile Cotton Tip
Applicator Sterile Cotton Tip
Bandaids ¾ ”
Brief Adult Stretch
Cleanser Cal Stat 4oz
Dressing Nugel 30GM
Enema Kit
Gown Disposable Imperv
Gown Plastic Universal
Heel Protector
Incentive Spirometer
K-Y Jelly 2oz
K-Y Jelly 4oz
Mask CPR Microshld LMCB
Mask Hifh Eff Reg
Mask High Eff Small
Mask FLSHLD
Mask Isolation (Yellow)
Ointment Providone/Iodine
Soap Septi Soft
Sharps Container
Stethoscope Sprague Rappo
Syringe Ear
Thermometer Probe Covers
Toothettes Oral Freshner
Underpads
M#101226
M#100294
M#103531
M#103549
M#100024
M#101254
M#015743
M#007306
M#106646
M#111245
M#115981
M#104935
M#110258
M#112459
M#111245
M#105271
M#111235
M#111232
M#105272
M#100198
M#104026
M#100686
M#104414
M#105882
M#106088
M#001805
M#106302
M#106385
Caring for the Community | preparing for an influenza pandemic 12
Appendix 5
Home Health Care:
Non-Routine Supplies
Item Medicare Number
ABD 7 ½ x 8
Ace Wrap 6”
Ace Wrap 4”
Ace Wrap 3”
Ace Wrap 2”
Acticoat 4x4
Adaptic 3x8
Adaptic 3x3
Adhesive 1” – 253
Adhesive ½ ” - 5103
Adhesive 3” – 5107
Alcohol Prep Pads/Wipes
Allevyn 6x6
Aquacel 4x4
Bag Drain Urine Leg-Anti 19oz
Bag Leg Dispoz
Bag Urine Drain
Betadine 8oz
Betadine Swabstix
Bulk Non-Sterile Drsg 2x2
Butterfly #23 23Gx3/4”
Butterfly #21 21Gx3/4”
Calcium Alginate Rope Alg
Catheter 8FR
Catheter Self 8FR
Catheter Red Rubber 14FR
Catheter 5cc 14FR
Catheter Infection Control 5cc 16FR
Catheter 5cc 16FR
Catheter 5cc 18FR
Catheter 5cc 20FR
Catheter 5cc 22FR
Catheter 5cc 24FR
Catheter 5cc 26FR
Catheter 30cc 16FR
Catheter 30cc 18FR
Catheter 30cc 20FR
Catheter 30cc 22FR
Catheter 30cc 24FR
Catheter Plug
Catheter Quick 22x1
Catheter Secure-Leg Strap
Catheter Strap
Catheter Texas
Catheter Tray 16fr w/bag
Cath Pedi Suction-Angio
Catheter 30cc 24FR 3/w
Catheter 15fr Uteral (straight)
M#100362
M#100115
M#100107
M#100099
M#100081
M#018163
M#108571
M#100347
M#106112
M#106104
M#106138
M#105510
M#018976
M#100293
M#011014
M#103622
M#103911
M#104026
M#114223
M#100420
M#105301
M#105023
M#022620
M#112565
M#007058
M#007055
M#100826
M#015709
M#100834
M#100842
M#100859
M#100867
M#100875
M#113910
M#100883
M#100891
M#100909
M#100917
M#111286
M#105593
M#114571
M#111468
M#017280
M#100743
M#007059
M#100612
M#110098
M#110700
Caring for the Community | preparing for an influenza pandemic 13
Catheter Seamless Foley w/o C M#007895
Item Medicare Number
Catheter All Purpose 16FR 941
Cavilon 3M No Sting Barrier
Cavilon 3M No Sting Barrier
Clear Absorbent Adherent
Coban 2 layer M2094
Coban 4”
Cotton Balls Sterile
Duoderm 4x4
Duoderm Extra Thin
Foam Adhesive Drsg 51/2” x 51
Gauze Mesalt Drsg
Gloves Sterile Size 6 ½
Gloves Sterile Size 7
Gloves Sterile Size 7 ½
Gloves Sterile Size 8
Graduate Cylinder Cup 32oz
Hemovac Mini-Jackson Pratt
Hydrosorb 4x4
Irrigation Bulb Syringes
Irrigation Tray with Piston
Kaltostat
Kerlix
Kerlix 2”
Kerlix Sponge Fluff
Kling Sof-Band 1”
Kling Sof-Band 2”
Kling Sof-Band 3”
Kling Sof-Band 4”
Lyafoam ‘A’ 4x4
Medipore Dressing 3M 5 7/8 x 1
Mesalt Ribbon
Mepitel 4x7.2
Montgomery Straps
Gauze Mesalt Ribbon
Gauze Sponge 4x4 (Allegiance)
Gauze Sponge 4x4 Sterile 16 Ply
Gauze Sponge 4x4 (Curity)
Gauze Vaseline 1x8
Gauze Vaseline 3x18
Gloves Non Sterile
Gloves Sterile Size 6
Gloves Single Sterile (L)
Duoderm Sacral
Fibracol Collag Drsg 2x2
Fibracol Plus Collagen Wnd 4x4 3/8”
M#100693
M#021524
M#020440
M#022325
M#06666
M#111583
M#104455
M#101336
M#100298
M#016840
M#011926
M#012134
M#021212
M#007739
M#020843
M#001167
M#012784
M#100552
M#013313
M#104745
M#104886
M#104786
M#104885
M#104794
M#104802
M#104810
M#104828
M#104547
M#115675
M#101270
M#106096
M#105064
M#013306
M#111427
M#000535
M#100749
M#100123
M#100131
M#100149
M#100156
M#100295
M#012661
M#020843
M#020585
M#101791
Caring for the Community | preparing for an influenza pandemic 14
18G Needle 1 ½ ” M#108308
Item Medicare Number
20G Needle 1 ½
21G Needle 1 ½ ”
22G Needle 1”
25G needle 5/8”
”
3cc IM/21G x 1 ½ ” Needle
3cc Sub-Q 22G x 5/8” Needle
22G Needle 1 ½ ”
25G Needle 1 ½ ”
5cc L-LOK Syr/Sterile
22G Angio-Cath 1”
18G Angio-Cath
Needle Huber 90 Degrees
Needle 19x1 ½ Filter
Suture Removal Kit
Syringe Sterile 5cc L-LOK
Syringe Sterile 10cc L-LOK
Syringe Sterile 20cc L-LOK
Syringe Sterile 30cc L-LOK
Syringe TB 1cc 27x1/2”
Syringe Cath-Tip 60cc
Nugauze w/iodoform ¼ ”
Nugauze w/iodoform ½ ”
Nugauze plain ¼ ”
Nugauze plain ½ ”
Nugauze plain 1”
Nugel Drsg 30Gm
Ostomy Sur-Fit Flexible Collar 2 ¼ ”
Ostomy Sur-Fit Flexible Tan Collar 1 ¾ ”
Ostomy Sur-Fit Flexible Tan Collar 1 ¼ ”
Ostomy Sur-Fit Drainable Pouch 2 ¼ ”
Peri Pads
Pleurx Drainage Kit 600ml
Pleurx Drainage Kit 1000ml
Polymem Wound Care Drsg
Prisma 28cm
Skin Staple Remover
Promogran Wnd Dressing 4.1 Sq
Silvasorb Gel 1.5oz
Sorbsan 4x4
Sorbsan Rope 12”
Sponge Bulk 4x4
Sponge Gen. Use 4x4
Sponge 2x2 Sterile
Sponge Drain Excillon 4x4
Sponge Soft Drain 2x2
Steri Strips 1”
Steri Strips
Steri-Strips
½
¼
”
”
M#115279
M#108282
M#115196
M#111567
M#108472
M#111021
M#111591
M#111617
M#107763
M#100612
M#100602
M#101535
M#107615
M#018940
M#018941
M#006032
M#006033
M#014084
M#007306
M#013198
M#013199
M#013200
M#013201
M#105361
M#022784
M#
M#021117
M#003752
M#012661
M#116731
M#022732
M#17928
M#001529
M#100446
M#109108
M#000767
M#100529
M#002076
M#105933
M#105932
M#105940
M#114579
M#107763
M#108399
M#112086
M#112003
M#114868
M#108431
Caring for the Community | preparing for an influenza pandemic 15
Tape Durapore 1” M#112425
Tape Durapore 2” M#106161
Item Medicare Number
Tape Durapore 3”
Tape Microfoam 3”
Tape Microfoam 4”
Tape Micropore 1”
Tape Micropore 2”
Tape Micropore 3”
Tape Transpore 1”
Tape Transpore 2”
Tape Transpore 3”
Tegaderm Absorb 3x3.75
Tegaderm Ag 4x5
Tegaderm Ag 2x2
Tegaderm 4x4
Tegaderm 4x8
Tegaderm 2x3
Tegagel hydrogel Wound Filler
Tegasorb Sacral
Telfa Pad 8x3
Telfa Pad 2x3
Tielle Wound Hydr Drsg 4 ¼ x 4
Tielle Hydro 2x2
Tube 18” Ltx Ext 24/c 150
Tray Trach Cleaning
Tray Irrigation w/60cc Syringe
Unna Boot Drsg Gelocast 4”
Urostomy Belt (Medium)
Urostomy Pouch Sur-Fit 32MM
Urostomy Pouch Sur-Fit 45MM
Urostomy Transparent Pouch
Urostomy wafer 1 ½ ” Flange
Wound Wash Saline 8oz
Wound Wash Saline 7oz
Webril Sterile Roll 4”
Wound Wash Saline
Xerfoam Drsg 5x9
Xerform Drsg 4x4
M#106179
M#112850
M#110916
M#106229
M#104612
M#108605
M#106237
M#111047
M#104620
M#022792
M#001567
M#023583
M#100354
M#111195
M#111435
M#022712
M#021561
M#101664
M#006618
M#011684
M#012131
M#000422
M#106740
M#105064
M#019169
M#013629
M#013202
M#013203
M#013628
M#013627
M#012754
M#012753
M#100271
M#012753
M#163166
M#012689
Caring for the Community | preparing for an influenza pandemic 16
Appendix 6
Centers for Disease Control – Interim Recommendations with In-Home Use Guidelines
Table 1. CDC Interim Recommendations for Facemask and Respirator Use for Home, Community, and Occupational Settings for Non-Ill Persons to Prevent Infection with Novel H1N1
1 2
Setting:
Community
No novel H1N1 in community
Novel H1N1 in community: not crowded setting
Novel H1N1 in community: crowded setting
Persons not at increased risk of severe illness from influenza
(Non-high risk persons)
Facemask/respirator not recommended
Facemask/respirator not recommended
Facemask/respirator not recommended
Persons at increased risk of severe illness from influenza (High-Risk
Persons) 3
Facemask/respirator not recommended
Facemask/respirator not recommended
Avoid setting.
If unavoidable, consider facemask or respirator
4 5
Home
Caregiver to person with influenza-like illness
Facemask/respirator not recommended
Avoid being caregiver. If unavoidable, use facemask or respirator
4 5
Facemask/respirator not recommended
Other household members in home
Occupational (non-health care)
No novel H1N1 in community
Novel H1N1 in community
Facemask/respirator not recommended
Facemask/respirator not recommended
Facemask/respirator not recommended but could be considered under certain circumstances
4 5
Occupational (health care) 6
Caring 7 for persons with known, probable or suspected novel H1N1 or influenza-like illness
Respirator
Facemask/respirator not recommended
Facemask/respirator not recommended but could be considered under certain circumstances
4 5
Consider temporary reassignment.
Respirator
1 The effectiveness of respirators and facemasks in preventing transmission of novel H1N1 (or seasonal influenza) in various settings is not known. Use of a facemask or respirator is likely to be of most benefit if used correctly and consistently when exposed to an ill person. (Ref. a) MacIntyre CR, et al. EID
2009;15:233-41. b) Cowling BJ, et al. Non-pharmaceutical interventions to prevent household transmission of influenza. The 8th Asia Pacific Congress of Medical Virology, Hong Kong, 26-28 February 2009.)
2 For the purpose of this document, respirator refers to N95 or any other NIOSH-certified filtering face piece respirator.
3 Persons at increased risk of severe illness from influenza (i.e. high-risk persons) include those groups at higher risk for severe illness from seasonal influenza, including: children younger than 5 years old;
Caring for the Community | preparing for an influenza pandemic 17
persons aged 65 years or older; children and adolescents (younger than 18 years) who are receiving longterm aspirin therapy and who might be at risk for experiencing Reye syndrome after influenza virus infection; pregnant women; adults and children who have pulmonary, including asthma, cardiovascular, hepatic, hematological, neurologic, neuromuscular, or metabolic disorders, such as diabetes; adults and children who have immunosuppression (including immunosuppression caused by medications or by HIV); and, residents of nursing homes and other chronic-care facilities.
4 The optimal use of respirators requires fit testing, training and medical clearance. Proper use is recommended to maximize effectiveness. The use of facemasks may be considered as an alternative to respirators, although they are not as effective as respirators in preventing inhalation of small particles, which is one potential route of influenza transmission. There is limited evidence available to suggest that use of a respirator without fit-testing may still provide better protection than a facemask against inhalation of small particles. Respirators are not recommended for children or persons who have facial hair ( see FDA
Web site ).
5 Use of N95 respirators or facemasks generally is not recommended for workers in non-health care occupational settings for general work activities. For specific work activities that involve contact with people who have influenza-like illness (ILI) (fever plus at least either cough or sore throat and possibly other symptoms like runny nose, body aches, headaches, chills, fatigue, vomiting and diarrhea), such as escorting a person with ILI, interviewing a person with ILI, providing assistance to an individual with ILI, the following are recommended: a) workers should try to maintain a distance of 6 feet or more from the person with ILI; b) workers should keep their interactions with the ill person as brief as possible; c) the ill person should be asked to follow good cough etiquette and hand hygiene and to wear a facemask, if able, and one is available; d) workers at increased risk of severe illness from influenza infection ( see footnote 3 ) should avoid people with ILI (possibly by temporary reassignment); and, e) where workers cannot avoid close contact with persons with ILI, some workers may choose to wear a facemask or N95 respirator on a voluntary basis (See footnote 1). When respirators are used on a voluntary basis in an occupational work setting, requirements for voluntary use of respirators in work sites can be found on the OSHA Web site .
6 See case definitions of confirmed, probable, and suspected novel influenza A (H1N1) . Also see infection control in the health care setting .
When respiratory protection is required in an occupational setting, respirators must be used in the context of a comprehensive respiratory protection program as required under OSHA’s Respiratory Protection standard (29 CFR 1910.134). This includes fit testing, medical evaluation and training of the worker.
7 “Caring” includes all activities that bring a worker into proximity to a patient with known, probable, or suspected novel H1N1 or ILI, including both providing direct medical care and support activities like delivering a meal tray or cleaning a patient’s room.
Caring for the Community | preparing for an influenza pandemic 18
Appendix 7
CDC Recommendations For Facemask Use to Prevent Transmission
Table 2. CDC Interim Recommendations For Facemask Use
For Persons Ill With Confirmed, Probable, Or Suspected
Novel Influenza A (H1N1)
1
To Prevent Transmission Of Novel
H1N1
2
Setting Recommendation
Home (when sharing common spaces with other household members)
Facemask preferred, if available and tolerable, or tissue to cover cough/sneeze
Facemask, if tolerable Healthcare settings (when outside of patient room)
Non-healthcare setting
Breastfeeding
Facemask preferred, if available and tolerable, or tissue to cover cough/sneeze
Facemask preferred, if available and tolerable, or tissue to cover cough/sneeze
1 See definitions for confirmed, probable, and suspect novel influenza A (H1N1) infection . Also see information on infection control in healthcare settings .
2 Ill persons should be placed in well ventilated areas when possible and placed in areas where at least a
6-foot distance can be maintained between the ill person and other well and ill persons. Selected references: a) Blumenfeld HL, et al. J Clin Invest 1959;38:199-212. b) Bridges CB, et al. Clin Infect Dis
2003;37:1094-1101. c) Foster MG and Cookson AH. Lancet 1918 (Nov. 2): 588-90. d) Gregg MB. Ann NY
Acad Sci 1980;353:45-53. e) WHO. Infection prevention and control of epidemic- and pandemic-prone acute respiratory diseases in health care. June 2007. f) Fabian P, et al. Plos One 2008;3:e2691.
Caring for the Community | preparing for an influenza pandemic 19
Appendix 8
Home Care Planning Issues
Incorporating Home Care Into Emergency Planning: Issues to Consider
Register patients being cared for in the home setting with a local emergency management agency and the public health department to ensure access to relevant information.
Ensure adequate stock of routine, chronic care medications.
Ensure adequate stock of basic first aid supplies, including but not limited to bandages, antipyretic medications (acetaminophen, ibuprofen), oral electrolyte solutions, and thermometers.
Ensure that backup utility support is in place if warranted (particularly for those patients requiring electricity support for medical devices).
Establish a “sick room” in the home for the primary management of ill household members, particularly in the event of a transmissible infectious disease.
In the event of caring for patients with advanced symptoms “too sick” for hospital care, coordinate symptom palliation with a home care team coordinated by local public health authorities.
Ensure the availability of a bedside commode or bedpan.
Ensure the availability of a bedside humidifier, if possible.
Source: Phillips, p. 49
Caring for the Community | preparing for an influenza pandemic 20
Appendix 9
Pandemic Flu Household Assessment Form
Name : ______________________ DOB : ______________
Address : _________________________________________
Phone number : ________________ E-mail : ________________
Alternate contact : ____________________________________
Primary care physician and hospital : ________________________________
Others in household (names and ages): ______________________________
____________________________________________________________________________________
Current Medical Concerns : ____________________________________________________________
Barriers to Care : Mental Memory Language Emotional Speech Hearing Financial
Non-Ambulatory Other ___________________________________________
Identified Needs : food medications water fuel baby needs
other___________________________
Education Provided : Flu resources further care referral other ___________________________
Visit Needed Team Assigned:_________________________
Other outcomes : ______________________________________
If needs are not medical in nature refer to non-medical staff and stop assessment.
Caring for the Community | preparing for an influenza pandemic 21
Appendix 10
Individual Medical Evaluation Form
Name : _____________________________ DOB : ___________
Last 4 digits of SS# ___________ Gender : male female
Any legal forms in place : POA ____ DNR ___ Other_______
Allergies : _____________________________________________
History of: CHF COPD Asthma CVA DM Cardiac Mental Pregnant
Other _____________________________
Date symptoms started : _______
Current medical condition:
Vital Signs: BP _____ P ______ Res ____ temp____ SaO ____
General Appearance: ___________________________________
HEENT: _____________________________________________
Respiratory: ___________________________________________
Cardiac: ______________________________________________
GI/GU: _______________________________________________
Neuro: _______________________________________________
Immunizations: flu pneumonia
Action taken in household : __________________________________________________________
Current Medications :________________________________________________________________
Care Provided : _____________________________________________________________________
Visit Frequency needed : __________________________________
Education provided:
____________________________________________________________________________________
If infected with flu, disposition: ________________________________________________
Contacts: ___________________________________________
Caring for the Community | preparing for an influenza pandemic 22
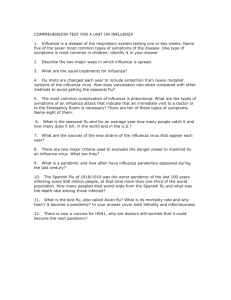
Appendix 11
Schematic Diagram
Caring for the Community | preparing for an influenza pandemic 23
Appendix 12
References
Agency for Healthcare Research and Quality. Recommendations for a National Mass Patient and Evacuee
Movement, Regulating, and Tracking System. Rockville, MD: Agency for Healthcare Research and
Quality; January 2009.
Home Health Care Services Pandemic Influenza Planning Checklist. Prepared by the U.S. Department of
Health & Human Services. Available at http://www.flu.gov/plan/healthcare/healthcare.html#f2 .
Accessed August 20, 2009.
Interim Pre-pandemic Planning Guidance: Community Strategy for Pandemic Influenza Mitigation in the
United States - Early, Targeted, Layered Use of Non-pharmaceutical Interventions. (2007) Centers for Disease Control. Available at www.pandemicflu.gov
Michigan Pandemic Influenza Community Health Plan, 2008. Draft 3.5. Attachment 16: Modular
Emergency Medical System. pp 151, 152.
Phillips SJ, Knebel A, eds. Mass Medical Care with Scarce Resources: A Community Planning Guide .
Prepared by Health Systems Research, Inc., an Altarum company, under contract No. 290-04-
0010. AHRQ Publication No. 07-0001. Rockville, MD: Agency for Healthcare Research and Quality
2007.
Caring for the Community | preparing for an influenza pandemic 24