Integrating Health into Comprehensive Planning DESIGN FOR HEALTH Planning Information Sheet:
advertisement

DESIGN FOR HEALTH
University of Minnesota | August 2007
Planning Information Sheet:
Ann Forsyth
Integrating Health into
Comprehensive Planning
Version 2.0
DESIGN FOR HEALTH is a collaboration between the University of Minnesota and
Blue Cross and Blue Shield of Minnesota that serves to bridge the gap between the
emerging research base on community design and healthy living with the every-day
realities of local government planning.
Planning Information Sheet: Integrating Health into Comprehensive Planning
Design for Health
www.designforhealth.net
© 2007
University of Minnesota
Permission is granted for nonprofit education purposes
for reproduction of all or part of written material or images,
except that reprinted with permission from other sources.
Acknowledgment is required and the Design for Health
project requests two copies of any material thus produced.
The University of Minnesota is committed to the policy
that all persons shall have equal access to its programs,
facilities, and employment without regard to race, color,
creed, religion, national origin, sex, age, marital status,
disability, public assistance status, veteran status, or sexual
orientation.
Design for Health is collaboration between the University of
Minnesota and Blue Cross and Blue Shield of Minnesota.
The following people were involved in the development of
the Information Sheet Series:
Series Editor: Dr. Carissa Schively
Contributors: Dr. Ann Forsyth, Dr. Kevin Krizek, Dr. Carissa
Schively, Laura Baum, Amanda Johnson, Aly Pennucci
Copy Editor: Bonnie Hayskar
Layout Designers: Anna Christiansen, Tom Hilde, Kristen
Raab, Jorge Salcedo, Katie Thering, Luke Van Sistine
Website Managers: Whitney Parks, Joanne Richardson
Suggested Citation: Design for Health. 2007. Planning
Information Sheet: Integrating Health into Comprehensive
Planning. Version 2.0. www.designforhealth.net
Design for Health
w w w.designforhealth.net
2
Planning Information Sheet: Integrating Health into Comprehensive Planning
Introduction
officials speak of health in relation to physical
activity, the natural environment, public safety,
healthy eating, mental health, social capital,
pollutants, and epidemiological issues related to
such topics as mortality, obesity, and respiratory
diseases. The following common definitions
of health illustrate that the connection to the
built environment is often isolated or indirectly
connected to the built environment (Ison 2000):
This first sheet in the series helps communities
begin thinking about how to integrate health
into their planning and design decisions. We
showcase: background information on the
relationship between health and the built
environment; various approaches to integrate
health into comprehensive planning; examples
from the Twin Cities region and across the U.S.
related to integrating health and planning; and
opportunities to integrate health into a traditional
comprehensive plan framework, focused on the
requirements of the Twin Cities Metropolitan
Council.
• “Health is a state of complete physical,
mental, and social well-being, and not merely
the absence of disease or infirmity,” as defined
by the Preamble to the Constitution of the
World Health Organization (WHO 1948).
•“Health is the reduction in mortality,
morbidity, and disability due to detectable
disease or disorder, and an increase in the
perceived level of health,” as defined by the
World Health Organization Regional Office
for Europe in “HEALTH21: The Health for
All Policy Framework for the WHO European
Region” (WHO Regional 1999).
Key Points
•Commonly used definitions of health tend to
ignore the built environment; however, there
is growing interest in the link between the
built environment and health. Comprehensive
planning is one approach to linking the
traditional notions of planning (land use,
transportation, community facilities, housing,
and parks and open space) with health themes
(physical activity, the nature environment,
public safety, healthy eating, mental health,
social capital, pollutants, and epidemiological
issues).
•“Health is a resource for everyday life, not
the object of living. It is a positive concept
emphasizing social and personal resources
as well as physical capabilities,” as defined
in WHO’s “Health Promotion Glossary”
(Nutbeam 1998).
•Comprehensive plans can help facilitate
decisions about health and the built
environment. To do so, it is important to
understand state and regional regulations that
often require a consistent set of elements where
health topics can be interwoven.
•“Health is the capacity of people to adapt to,
respond to, or control life’s challenges and
changes,” as defined in “Health Impact
Assessment as a Tool for Population Health
Promotion and Public Policy” (Frankish et al.
1996).
•There are four approaches to incorporate
health into comprehensive planning: plan
update, corrective/selective amendments,
revised codes and ordinances, and a separate
health-related plan.
Public Health Overview
Design for Health
w w w.designforhealth.net
Ann Forsyth
There is growing interest in the link between the
built environment and health. The traditional
notions of planning encompass land use,
transportation, community facilities, housing,
and parks and open space, while public health
Bicycle parking garages feature green roofs in Hammarby
Sjöstad, Stockholm, Sweden
3
Planning Information Sheet: Integrating Health into Comprehensive Planning
patterns contribute to increased reliance on the
automobile, for example, and thus increased
emissions (Handy 2005), while other material
suggests that the congestion of central cities
or higher-density areas leads to dangerous air
quality (FHWA 2006), particularly for active
individuals, such as cyclists and pedestrians
(EPA 2007). The topic of air quality, however,
gets increasingly complicated because air is not
contained by political boundaries, and this makes
it difficult to coordinate a joint-planning response
(Randolph 2004).
While planning and public health share similar
roots in the nineteenth and early twentieth
centuries, for some time they have been moving
along separate paths. While planners and public
health professionals have viewed their roles
in the community differently, practitioners
and academics are beginning to uncover the
ties between the two fields as it is becoming
increasingly clear that decisions about the built
environment may influence certain public health
concerns and vice versa. The list below provides a
brief introduction to how public health concerns
are linked to community planning issues. For
more detail see the Design For Health’s Key
Question Research Summaries.
Metropolitan Design Center
Water Quality: Water quality refers to both
drinking water and groundwater/surface water.
Diseases are quickly spread through water
because of its solvent nature, which makes it easy
to pass along to all living things (Frumkin, Frank,
and Jackson 2004). While this is less of an issue
in the United States, because of the country’s
advanced water treatment systems, it is still a
priority for communities as they must coordinate
and manage these very systems or work with
other public/private groups to make sure that
they are protecting surface and groundwater,
and planning for public facilities to protect water
quality (Berke et al. 2006; Randolph 2004).
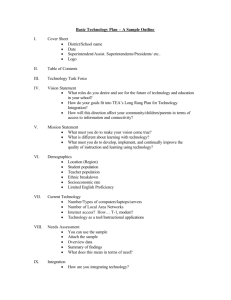
Freeways are sources of air pollution. This image is of
Interstate 35, Minneapolis
Mental Health: The World Bank and the
World Health Organization estimate that by
the year 2020, mental-health disorders will
account for 15 percent of disease, and that
depression will become one of the largest health
problems in the world (Maller et al. 2005, 45-6,).
Vegetated environments have positive effects
on physiological measures, such as heart rate,
skin conductance, muscle tension, and blood
pressure (Maller et al. 2005). There has been an
increasing interest in how nature (defined as
water, trees, bushes, grass, and other kinds of
vegetation) within the built environment can
influence changes in mental health. Exposure
to nature may lead to decreased levels of stress,
greater job satisfaction and faster recovery from
fatigue (Kaplan and Kaplan 1989; Ulrich 1984;
Ulrich et al. 1991; Maller et al. 2005). For planners,
parks and open-space planning is an important
consideration. Many comprehensive plans
identify these resources, assess residents’ needs
Air Quality: Clean air is an important element
in creating healthier communities. Both indoorand outdoor-air quality are important in human
health, with key pollutants including carbon
monoxide, sulfur and nitrogen oxides, carbon
dioxide, lead, and other air toxins and volatile
organic compounds (Frumkin, Frank, and
Jackson 2004, 73). From a planning perspective,
automobile emissions are a key area of concern.
It is estimated that in 1999, there were over 122
million people living in areas where the ozone
levels greatly exceeded national air-quality
standards (Randolph 2004, 44). Pollutants, such
as ozone, can lead to a myriad of short- and
long-term health problems, particularly related
to respiratory diseases such as asthma. There
has been extensive research on the connection
between land-use patterns, transportation,
travel behavior, and air quality. Mounting
evidence suggests that sprawling land-use
Design for Health
w w w.designforhealth.net
4
Planning Information Sheet: Integrating Health into Comprehensive Planning
for parks and open space, and identify areas
for protection as part of the land-use planning
process (Kelly and Becker 2000).
imbalance, that is, more energy being consumed
than expended through physical activity. Thus,
part of the problem of obesity is a problem of
food consumption. At the same time a significant
group of people do not consume adequate
healthy food. Good nutrition has been promoted
over time through public health programs such
as the “5 A Day” campaign to promote fruit
and vegetable consumption and the Special
Supplemental Nutrition Program for Women,
Infants, and Children (WIC). However, access
to nutritious food is emerging as an important
planning issue involving topics from supermarket
and restaurant locations to providing space for
community gardens (Laraia et al. 2005; Chung
and Myers 1999; Kaufman and Pothukuchi 2000;
Morland, Wing, and Diez Riux 2002; Crewe, ed.
2004).
Metropolitan Design Center
Social Capital: Social capital may be
characterized as one’s social network or sense
of attachment to one’s community. It should
be noted that the lack of social capital, like
poor air quality, is not a health outcome but
may be associated with or contribute to health
(Carpiano 2006). Research is mixed on whether
or not the built environment can influence social
capital, partly because it is difficult to define and
measure. Depending upon how social capital
is measured, some research finds that mixeduse, walkable urban areas increase social capital
(Leyden 2003; Lund 2002), while others find that
less dense areas, like suburban communities,
have higher levels of trust in their neighbors
(Williamson 2004). Social capital is one of the least
understood issues in terms of its relationship to
public health, as well as to the built environment.
Public gallery spaces can be enabled through planning. This
example is in New York City, NY
Food Environment: Local, state, and federal
groups have referred to the rising levels of
obesity as a public-health crisis, particularly
because it is connected to a range of other health
issues. Traditionally, planners and public-health
officials have tried to decrease levels of obesity
through the lens of physical activity; however,
there has been a recent movement towards
looking at accessibility to healthy foods. The
current obesity problem is a result of energy
Design for Health
w w w.designforhealth.net
5
Physical Activity: The connection between
urban form and physical activity has been the
area where most debate has occurred in recent
years. While the genetic make-up of humans
determines many of the health risks that each
individual faces, physical activity remains
an important element in combating diseases,
including obesity and heart disease (Frumkin,
Frank, and Jackson 2004). Researchers are moving
beyond an emphasis on either leisure physical
activity (e.g., walking for exercise) or utilitarian
physical activity (e.g., walking to work) to a
more comprehensive view. In health terms it is
particularly important to consider the intensity
(moderate v. vigorous) of the activity, as well as
the overall amount. Different subpopulations
(age, gender, and ethnicity), however,
have differing barriers towards achieving
recommended exercise goals. Together, these
elements create a framework for planners and
designers in order to help them build
environments to create opportunities for physical
activity from parks and open space to sidewalks
and land use, including safety considerations.
Active transportation—walking and cycling—
requires a different set of infrastructure than
the roads and trails needed for motorized
transportation (Committee on Physical Activity
2005).
Planning Information Sheet: Integrating Health into Comprehensive Planning
Environment and Housing: Environmental and
housing issues include a broad range of topics
such as indoor and outdoor housing quality
(building materials, crowding, location of
housing, and presence of toxics), contaminated
and/or potentially contaminated sites – to
name just a few. Beyond air and water quality,
exposure to other pollutants may have negative
impacts on health. Exposure to pollutants can be
unpredictable, but in some cases can be affected
by land-use decisions and building codes.
Especially for children, for example, exposure to
lead paint is a significant concern in many older
urban neighborhoods (Evens and Gard 2005).
Contaminated soils and exposure to hazardous
waste, associated with ongoing or previous
industrial activities, may also be a concern where
residents are put in close contact with brownfield
sites (Randolph 2004; Bullard 1990).
Providing a variety of activities and a range of
transportation options to increase choices for
individual travelers is important for all residents,
but particularly for those groups that are transit
dependent.
The Role of Comprehensive
Planning
As a policy framework, the comprehensive plan
can help to facilitate decisions about health
and the built environment, although it is only
one strategy for improving human health.
While many plans refer to the importance of
public health, public safety or physical activity,
these general concepts are often used to justify
purposes as opposed to providing a substantive
starting point for discussions about how a
community should look and function.
Accessibility: Accessibility planning focuses
on the degree to which people can easily get
to destinations that directly or indirectly are
linked to supporting human health. Planners
can help increase access by ensuring that policies
and implementation strategies encourage a
variety of nearby destinations for residents (e.g.,
employment, health care, grocery stores, etc.),
and that these destinations can be reached by a
variety of transportation modes (e.g. bicycling,
walking, automobile, transit). Accessibility
concerns focus less on automobile users and
more on bicyclists, pedestrians, and transit
riders since these people tend to be underserved.
Universal design is an aspect of accessibility
that is particularly focused on specialized
populations.
When integrating health into comprehensive
planning, there is not a single pattern that
planners and designers must follow. Rather,
there are different ways to incorporate these
themes into existing comprehensive plans and
other typical community-planning efforts. These
options provide flexibility to communities,
allowing them to make decisions based on
community resources and public priorities.
Approaches to Integrating Health
into Your Comprehensive Plan
There are four general approaches to integrating
health into a community’s comprehensive plan.
Ann Forsyth
1. Comprehensive Plan Update
A community’s comprehensive plan update
process is an important opportunity to rethink
the organization and focus on the plan. Through
a comprehensive update, communities have
the opportunity to fully integrate a concept,
such as health, by applying it to each section of
the comprehensive plan. Many communities
conduct a visioning and/or goal-setting process
as part of their plan update. This effort presents
an opportunity to discuss the relationship
between health and the built environment, and
to organize the community around key goals
and opportunities to be pursued. In addition,
the content contained in each of the plan
Comprehensive planning can support non-motorized
transportation options. This bike path is in Amsterdam, The
Netherlands
Design for Health
w w w.designforhealth.net
6
Planning Information Sheet: Integrating Health into Comprehensive Planning
elements can be informed by the connection
between health and the built environment.
Decisions that communities make about land use,
transportation, environment, parks, open space,
and community facilities can all have implications
for health. See www.designforhealth.net for a
variety of ways to incorporate health into key
comprehensive plan elements and ordinances.
For example, in its transportation element, Eden
Prairie, Minnesota, has a section on bicycle and
pedestrian facilities, along with guidelines related
to roadways, transit and airports. One of the
implementation strategies in the plan states that,
“The City will pursue the continued development
of pedestrian trails and bikeways that meet the
recreational needs of its citizens, and provide
an alternative means of transportation.” (City
of Eden Prairie 2000). Also in Minnesota, Saint
Louis Park’s comprehensive plan illustrates
another approach and opportunity. Section IV
on public facilities has an entire chapter entitled
“Public Health and Safety” (the other chapters
include “Aviation Plan,” “Water Supply Plan,”
“Sewer Plan and Solid Water,” and “Surface
Water Resource Management”). While it tends
to focus more on fire, police, medical emergency,
and public works, the chapter could be expanded
to address other aspects of health (City of Saint
Louis Park 1998).
The City of Saint Paul, Minnesota, already lists
“well-being” among its overarching planning
themes. The City’s comprehensive plan states,
“Well-being for Saint Paul’s citizens depends
on economic growth and life-supporting jobs,
as well as cultural, educational and recreational
opportunities, including community services that
nurture family and individual life” (City of Saint Paul
1999).
King County, Washington, has taken a
proactive approach to integrating health into its
comprehensive plan. By directing development
and higher densities to cities and urban centers,
the County is accomplishing its growthmanagement goals, but also concentrating new
population growth in areas with a mix of land
uses, existing services and facilities, and higher
densities as a means of promoting health. King
County also connects environmental planning to
health, providing actions related to improving air
quality. As a complement to its comprehensive
plan, the County also completed a land-use,
transportation, air quality, and health study to
assess how land-use patterns affect air quality
(County of King 2004).
Many communities include elements related to
public health or human services. These elements
may address a range of health issues, including
mental health, air quality, water quality, and
safety. Palm Beach County, Florida, for example,
includes safety goals related to protection from
environmental hazards, emergency management
and training of health workers (County of Palm
Beach 2001). Spokane, Washington, added a
social-health element to its comprehensive plan.
As noted in the plan, “Healthy communities
embrace a complex set of factors that contribute
to good health: housing choices, clean natural
environments, efficient public transportation,
employment options, job training, quality
education, cultural and recreational opportunities,
room for diversity, accessible health services,
and preventive services” (City of Spokane
2001). Comprehensive plan elements like these
examples could certainly be added or expanded
to address a broader range of health issues.
2. Corrective/Selective Amendments
This approach is a strategic way to update or add
to existing comprehensive plan content, without
revising the entire document. Approaches might
include adding short text amendments, such as
defining health to include a broader range of
issues than are addressed in the current plan.
Drafting supplemental sections or full elements
can be a useful way to address health in a manner
that responds to local concerns. Options include
providing goals and policies for non-motorized
transportation, adding a section on mitigating
impervious surfaces, or adding an air-quality
element.
Design for Health
w w w.designforhealth.net
Air quality is an important health issue that can
be addressed in a community’s comprehensive
plan. Some cities, primarily in the western states
and including Carson, California, include an
element in their comprehensive plans specific
to air quality. The element includes air-quality
data, information on state and federal air-quality
7
Planning Information Sheet: Integrating Health into Comprehensive Planning
standards and goals related to dust generation,
regional air quality, community awareness and
emergency response, and polluting industries
(City of Carson 2004).
4. Separate Health-related Plans
Many communities create separate plans for
topics that go beyond the scope of required
comprehensive plan content and elements (e.g.,
Downtown Plan, Historic Preservation Plan,
Habitat Protection Plan). These plans may be
related to issues unique to the community, focus
on sub-areas in the community or respond
to issues of public concern. These thematic
plans often influence the decisions made in
the overarching comprehensive plan, and in
some cases are adopted as an extension of the
comprehensive plan. Key examples include
downtown plans, historic preservation plans,
habitat protection plans, and neighborhood plans.
3. Revised Codes or Ordinances
This approach is focused more on the
implementation side of comprehensive
planning, such as revising a community’s
zoning ordinances, subdivision regulations,
planned-unit development requirements, design
standards, and other implementation tools.
Here, tools such as pedestrian-overlay zones,
non-motorized-circulation standards, and parkdedication requirements may be used to translate
comprehensive plan policies into action. More
details about plan implementation and examples
of model ordinances are included in additional
information sheets.
In the local context, Eden Prairie, Minnesota, has
adopted a local water management plan. The
plan includes guidelines for development review,
such as: (1) managing storm-water runoff, erosion
and sedimentation; (2) holding runoff rates to
predevelopment conditions; and (3) protecting
wetlands to ensure surface water quality (City of
Eden Prairie 2004). In addition, the “Saint Paul
on the Mississippi Development Framework”
is a separate document that influences planning
through design strategies related to motorizedand non-motorized-transportation networks
and the public realm in the city of Saint Paul,
Minnesota (Saint Paul Riverfront 1997).
Protecting health is one of the key justifications
used for local government land-use,
environmental and other regulations. Arden
Hills, Minnesota, specifically provides such a
justification in the introduction to its zoning
ordinance, listing the “promotion of general
public health, safety, comfort and general welfare
of their inhabitants” among the purposes for
the ordinance (City of Arden Hills 2006). One
regulation that Arden Hills provides, relative
to this statement of purpose, is a requirement
that a water-management plan be submitted for
development of individual sites of 2.5 acres or
greater in wetland and floodplain areas.
Relying on a connection between walkable
environments and health benefits, one technique
that might be used is a pedestrian-oriented
overlay zone. Greensboro, NC, has established
design guidelines and an overlay zone for the
East Market Street area, a major thoroughfare
that runs through the entire city. The design
guidelines and zoning regulations address
façade design, building orientation, parking-lot
landscaping/lighting, site access and safety, and
bicycle and pedestrian connections with the intent
of creating an environment that is more inviting
for pedestrians (City of Greensboro 2002).
Many communities prepare plans specifically
related to bicycle and pedestrian facilities.
One example is the city of Austin, Texas. Its
plan’s overall goals are to: (1) institutionalize
bicycle transportation in all transportation and
recreation planning, design and construction
activities; (2) improve bicycle safety; (3)
increase the level of commuting and utilitarian
bicycling; (4) fund, create and maintain a
functional system of on- and off-street bicycle
facilities; (5) establish and maintain safe
standards and guidelines for bicycle facilities,
programs and projects; and (6) integrate and
coordinate multiple modes of transportation
through provision of bicycle/transit interfaces
(City of Austin 1996).
A community’s selection of an approach will
likely be informed by a number of factors
including: (1) staff and financial resources
available to complete the plan revisions, (2)
Design for Health
w w w.designforhealth.net
8
Planning Information Sheet: Integrating Health into Comprehensive Planning
plans. In addition to requiring sections related
to background information and implementation,
the Metropolitan Council requires that local
comprehensive plans include four key elements:
political and public support for integrating health
into the plan and (3) the date and organization
of the existing plan. Further, a community might
opt to combine several of these approaches,
perhaps providing minor amendments to an
existing comprehensive plan and following up by
drafting relevant ordinance revisions.
• Land Use
• Transportation
• Parks and Open Space
• Water Resources
The Metropolitan Council cites three additional
elements as optional:
Conforming to State Regulations
In selecting an approach to integrating health
in the comprehensive plan, communities
also are influenced by existing guidelines
related to comprehensive plan content. In
some states, planning-enabling legislation
prescribes particular elements or content that
must be included in a community’s plan. In
other locations, planners are simply guided
by traditional approaches to comprehensive
planning that rely on a relatively consistent set
of elements. Even where a relatively traditional
comprehensive planning framework is
established, there remain multiple opportunities
to address a range of health issues.
One example of a traditional comprehensive
planning framework is provided by Minnesota’s
Metropolitan Land Planning Act (Minnesota
Statutes §§ 473.459-.459) and the Metropolitan
Council for plans completed by communities in
the Minneapolis-Saint Paul (Twin Cities) sevencounty metropolitan area. Specific guidance is
provided related to the timing and content of
Design for Health
w w w.designforhealth.net
The Metropolitan Council provides general
guidance related to the content of these elements
in its “Local Planning Handbook” (2005). While
a number of specific requirements are provided,
communities have a great deal of flexibility in
how they address these requirements and the
extent to which they provide additional content.
This flexibility presents a significant opportunity
to address a range of health issues, including
physical activity, water quality, air quality, food
access, safety, social capital, and mental health.
Further, the comprehensive planning process
presents an opportunity to engage the public
in these health issues. Planners can gather
information about public values and priorities
around the issues and help the public to make
the connection between health and the built
environment.
Green spaces integrated with housing can have a number of
benefits including improved mental health. This example is in
Woodbury, Minnesota
9
Metropolitan Design Center
Nicollet Mall in Minneapolis, Minnesota is an example of an
area planned for pedestrians and transit.
Metropolitan Design Center
• Economic Development
• Intergovernmental Coordination
• Urbanization and Redevelopment Areas
Planning Information Sheet: Integrating Health into Comprehensive Planning
The Metropolitan Council’s Requirements
for Comprehensive Plans: A Brief List of
Health Issues
Using the Matrix in Your Own
Community
By considering the Metropolitan Council’s
plan requirements, communities can identify
numerous opportunities to integrate health
into comprehensive planning. Using a matrix
such as the one on the next page, one can make
clear links between various aspects of health
and traditional planning elements, including
information required by the Metropolitan
Council. Even for communities outside of the
Twin Cities region, the matrix can be a useful
tool to organize efforts to integrate health
into a community’s comprehensive plan. The
matrix includes plan content specified by the
Metropolitan Council and a number of relevant
health issues.
Focusing on the minimum content required
by the Metropolitan Council, the matrix on
the previous page provides a starting point
in communities for discussing opportunities
to integrate health into their comprehensive
plans. Communities might also include other
elements or content in this matrix to reflect
local concerns or typical plan content (e.g.,
community facilities, environmental protection,
urban design). To further tailor the matrix to the
local context, additional health issues or specific
health concerns related to the general categories
provided above also could be included (e.g.,
access to supermarkets for low-income residents,
high asthma rates in neighborhoods adjacent
to highways). Use of this tool as part of the
public participation process can be effective in
increasing awareness of the relationships between
health and the built environment. The public may
be a significant source of information about key
health issues and the feedback gathered during
a participatory process may be useful in drafting
goals and identifying policy options.
The health issues included in the matrix were
introduced earlier and were identified based
on a review of wide-ranging literature on
the relationship between health and the built
environment, drawing from research in the areas
of public health, environmental management,
transportation planning, urban design, and
healthy eating. Frumkin, Frank and Jackson
(2004) use many of these same categories of
health, including air quality, physical activity,
traffic safety, water quality, mental health, and
social capital, relating them to urban sprawl. A
recent American Planning Association “Planning
Advisory Service Report” on integrating planning
and public health, addresses some of these same
issues but also adds obesity and inactivity, crime,
hazardous waste sites, and transported materials
(Morris 2006). The matrix used here (see p. 9)
includes the additional concerns of food access,
pollutants and epidemiological issues, such as
the concentration of diseases within particular
populations or geographic areas.
Design for Health
w w w.designforhealth.net
10
Planning Information Sheet: Integrating Health into Comprehensive Planning
Sample Matrix for Examining the Links between Comprehensive Planning and Health
Water
Quality
Food
Access
Safety
(crime &
traffic)
Access
Env and
Housing
x
x
x
x
x
x
x
x
x
x
x
x
x
Physical
Activity
Social
Capital
Mental
Air
Health Quality
Future land use
x
x
x
x
Housing plan
x
x
x
Resource Protection
x
x
x
Land-use plan
Transportation
Traffic Analysis
Zone (TAZ) allocation
x
x
x
x
Highway & roads
plan
x
x
x
x
Bike &
pedestrian plan
x
x
Special traffic
situation
x
Transit plan for
facilities & services
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
x
Aviation plan
x
Water Resources
x
Wastewater &
sewer plan
x
Surface water
management plan
Water supply plan
x
x
x
x
x
x
Parks & Open Space
Identity, plan, map
& plan for regional
parks and open
space
x
x
x
x
x
x
x
x
x
x
x
Optional Elements
Economic
development
Intergovernmental
coordination
Urbanization &
redevelopment
areas
Design for Health
w w w.designforhealth.net
x
x
x
x
x
x
11
x
x
x
Planning Information Sheet: Integrating Health into Comprehensive Planning
Notes
City of Carson, California. 2004. Carson
general plan. http://ci.carson.ca.us/content/
department/dev_service/generalplan.asp.
City of Carson, California. 2004. General Plan.
http://ci.carson.ca.us/content/department/
dev_service/generalplan.asp
* The key approaches identified here were
informed by the American Planning Association’s
“Model Smart Growth Land Development
Codes” (Meck et al. 2006). This document
addresses ways to integrate smart-growth
concepts into comprehensive plans. Using these
same approaches, we have identified methods for
integrating health into comprehensive plans.
City of Eden Prairie, Minnesota. 2000. City of
Eden Prairie comprehensive plan update.
http://www.edenprairie.org/vCurrent/upload/
contents/228/Chapters%201-4.pdf and http://
www.edenprairie.org/vCurrent/upload/
contents/228/Chapters 5-11.pdf.
References
Berke, P. R., D. R. Godschalk, E. J. Kaiser, and D.
A. Rodriguez. 2006. Urban land use planning.
Fifth ed. Urbana, IL: Univ. of Illinois Press.
———. 2004. Local water management plan.
http://www.edenprairie.org/vCurrent/upload/
contents/228/Local Water Management Plan.
pdf.
City of Greensboro, North Carolina. 2002. East
Market Street pedestrian scale overlay plan,
design guidelines, and overlay zone development
regulations. http://www.greensboro-nc.gov/
Departments/Planning.
Bullard, R D. 1990. Dumping in Dixie: Race,
class, and environmental quality. Boulder, CO:
Westview Press.
Carpiano, R. 2006. Toward a neighborhood
resource-based theory of social capital for health:
Can Bourdieu and sociology help? Social Science
& Medicine 62 (1): 165-175.
City of Saint Louis Park, Minnesota. 1998.
Saint Louis Park comprehensive plan. http://
www.stlouispark.org/city_hall/community_
development_comp_plan.htm.
Chung, C., and S. L. Myers. 1999. Do the poor
pay more for food? An analysis of grocery store
availability and food price disparities. Journal of
Consumer Affairs 33 (2): 276.
City of Saint Paul, Minnesota. 1999. The Saint
Paul comprehensive plan. http://service.
govdelivery.com/docs/STPAUL/STPAUL_
DeptPED/STPAUL_44/STPAUL_44_20010125_
en.htm.
City of Arden Hills, Minnesota. 2006. Zoning
ordinance. http://www.ci.arden-hills.mn.us/
index.asp?Type=B_LIST&SEC={4FDEE185-D22347C4-BEFC-790771DEB6F2}&DE=.
City of Spokane, Washington. 2001. City of
Spokane comprehensive plan. http://www.
spokaneplanning.org/Documents/BEGIN.PDF.
City of Arden Hills, Minnesota. 1998.
Comprehensive plan. http://www.
ci.arden-hills.mn.us/index.asp?Type=B_
BASIC&SEC=%7B284EC3A9-23F7-4767-BB74557F41615B6D%7D.
Committee on Physical Activity, Health,
Transportation, and Land Use, Transportation.
2005. Does the built environment influence
physical activity? Examining the evidence.
Special Report 282. Washington, DC:
Transportation Research Board, Institute of
Medicine of the National Academies.
City of Austin, Texas. 1996. Austin bicycle plan,
Part 1. http://www.ci.austin.tx.us/bicycle/
plan1.htm.
County of King, Washington. 2004. King County
comprehensive plan. http://www.metrokc.gov/
ddes/compplan/2004/index.htm.
Design for Health
w w w.designforhealth.net
12
Planning Information Sheet: Integrating Health into Comprehensive Planning
County of Palm Beach, Florida. 2001.
Palm Beach County comprehensive plan.
http://www.pbcgov.com/pzb/Planning/
comprehensiveplan/tableofcontent.htm.
Kelly, E. D., and B. Becker. 2000. Community
planning: An introduction to the comprehensive
plan. Washington, DC: Island Press.
Laraia, B., A. M. Siega-Riz, J. Kaufman, and
S. J. Jones. 2004. Proximity of supermarkets is
positively associated with diet quality index for
pregnancy. Preventive Medicine 39: 869-75.
Crewe, K., ed. 2004. Food and planning issue.
Progressive Planning Magazine 148.
Evens, A., and B. J. Gard. 2005. Enforcement of
lead hazard remediation to protect childhood
development. Journal of Law, Medicine and
Ethics 33 (4): 40-45.
Leyden, K. M. 2003. Social capital and the built
environment: The importance of walkable
neighborhoods. American Journal of Public
Health 93 (9): 1546-1551.
Federal Highway Administration (FHWA). 2005.
VMT growth and improved air quality: How
long can progress continue? http://www.fhwa.
dot.gov/environment/vmt_grwt.htm.
Lund, H. 2002. Pedestrian environments and
sense of community. Journal of Planning
Education and Research 21 (3): 301-12.
Frankish, C. J., L. W. Green, P. A. Ratner, T.
Chomik, and C. Larsen. 1996. Health impact
assessment as a tool for population health
promotion and public policy: A report submitted
to the Health Promotion Development Division
of Public Health Agency of Canada. Vancouver:
Institute of Health Promotion Research,
University. of British Columbia.
Maller, C., M. Townsend, A. Pryor, P. Brown, and
L. St. Leger. 2005. Healthy nature healthy people:
‘Contact with nature’ as an upstream health
promotion intervention for populations. Health
Promotion International 21 (1): 45-54.
Meck, S., M. Morris, K. Bishop, and E. Damian.
2006. Interim PAS report: Model smart land
development regulations. Chicago: American
Planning Association.
Frumkin, H., L. Frank, and R. Jackson. 2004.
Urban sprawl and public health: Designing,
planning, and building for healthy communities.
Washington, DC: Island Press.
Metropolitan Council. 2005. Local planning
handbook.ttp://www.metrocouncil.org/
planning/LPH/handbook.htm.
Handy, S. 2005. Smart growth and the
transportation-land use connection: What does
the research tell use? International Regional
Science Review 28 (2): 1-22.
Morland, K., S. Wing, and A. Diez Riux. 2002. The
contextual effect of the local food environment
on residents’ diets: The atherosclerosis risk in
communities study. American Journal of Public
Health 92 (11): 1761-67.
Ison, E. 2000. Resources for health impact
assessment; Volume 1: The main resource.
London: National Health Service Executive.
http://www.hiagateway.org.uk/media/
hiadocs/VOL_I_Resource_for_HIA_l.pdf.
Morris, M. 2006. Integrating planning and public
health: Tools and strategies to create healthy
places. Planning advisory service report 539/540.
Chicago: American Planning Association.
Kaplan, R., and S. Kaplan. 1989. The experience
of nature: A psychological perspective.
Cambridge, UK:Cambridge Univ. Press.
Nutbeam, D. 1998. Health promotion glossary.
Geneva: Div. of Health Promotion, Education and
Communication (HPR), Health Education and
Health Promotion Unit (HEP), WHO.
Kaufman, J. L., and K. Pothukuchi. 2000. The
food system: A stranger to the planning field.
Journal of the American Planning Association 66
Randolph, J. 2004. Environmental land use
planning and management. Washington, DC:
(2): 113-24.
Design for Health
w w w.designforhealth.net
13
Planning Information Sheet: Integrating Health into Comprehensive Planning
Island Press.
Saint Paul Riverfront Corporation. 1997. Saint
Paul on the Mississippi development framework.
http://www.riverfrontcorporation.com/
framework.asp.
Ulrich, R. S. 1984. View through a window may
infl uence recovery from surgery. Science. (4) 20-1.
Ulrich, R. S., R. F. Simons, B. D. Losito, E.
Fiorito, M.A. Miles, M. Zelson. 1991. Stress
recovery during exposure to natural and
urban environments. Journal of Environmental
Psychology. 11: 201-30.
U.S. Environmental Protection Agency (EPA).
2003. A brief guide to mold, moisture, and your
home. Washington, DC: EPA.
———. 2007. Health and environmental impacts
of ground-level ozone. http://www.epa.gov/
air/ozonepollution/health.html.
Williamson, T. M. 2004. Sprawl, justice, and
citizenship: A philosophical and empirical
inquiry. Ph.D. Diss. Cambridge, MA: Harvard
Univ.
World Health Organization (WHO). 1948.
Preamble to the constitution of the World Health
Organization. Geneva: WHO.
World Health Organization (WHO) Regional
Office for Europe. 1999. HEALTH21: The health
for all policy framework for the WHO European
region. Geneva.
Design for Health
w w w.designforhealth.net
14