AN ABSTRACT OF THE THESIS OF
advertisement

AN ABSTRACT OF THE THESIS OF
Carol Ann Keller for the degree of Doctor of Philosophy in Pharmacy presented
on May 4, 2000. Title: Development and Testing of a Sustained Release
Acetaminophen Tablet for the Treatment of Chronic Pain in Osteoarthritis
Patients.
Redacted for privacy
Abstract approved:
James W. Ayres
Acetaminophen has been safely used for analgesia for many years.
Literature suggests that a plasma acetaminophen level of 5p.g/ml is necessary to
maintain analgesic relief in humans. Current dosing regiments are inconvenient (every
4-6 hours) and do not maintain this minimum plasma level. Simulations were
conducted to examine various doses and input rates for sustained release formulations
of acetaminophen. Once parameters were selected from the simulations, sample
formulations were prepared and tested using standard dissolution techniques.
Investigations into dose/size relationships, hydroxypropylmethylcellulose (HPMC)
percentage for erosion matrix tablets, compression force, tablet shape, tablet
divisibility, and granulation methods were performed for non-disintegrating
hydrophilic matrix tablets.
Tablets containing 5% and 7.5% HPMC were selected for pharmacokinetic
study in 10 healthy human subjects. Tylenol Extra Strength and Tylenol Extended
Relief tablets were administered as control formulations. Pharmacokinetic fitting of
the kinetic profiles of all four formulations were performed using Win Nonlin. The
formulations were best described by a 1-compartment open model with first order
input and first order elimination. The 5% HPMC sustained release acetaminophen
formulation was selected for Phase II clinical trials.
Patients with osteoarthritis of the knee were recruited for a double blind
crossover study of 5% HPMC sustained release acetaminophen formulations and
immediate release acetaminophen. Patients received two tablets of study medication,
four times a day for 4 weeks. After a seven day wash-out period patients were then
crossed over to the other treatment. Patients were evaluated using a twelve question
questionnaire and the time to walk 50 feet was measured. Thirty patients were
enrolled in the study and seventeen patients completed the study. The sustained
release formulations were statistically superior to the baseline treatments in reducing
pain level, decreasing disability, and improving the duration of pain relief. Additional,
larger scale studies are needed to confirm these findings.
Development and Testing of a Sustained Release Acetaminophen Tablet for the
Treatment of Chronic Pain in Osteoarthritis Patients
by
Carol Ann Keller
A THESIS
Submitted to
Oregon State University
in partial fulfillment of
the requirements for the
degree of
Doctor of Philosophy
Presented May 4, 2000
Commencement June 2000
Doctor of Philosophy in Pharmacy thesis of Carol Ann Keller presented
on May 4, 2000
APPROVED:
Redacted for privacy
Majoy7rofessor, representing
Redacted for privacy
Dean of College of
Redacted for privacy
Dean of G/a)1Ie School
I understand that my thesis will become part of the permanent collection of
Oregon State University libraries. My signature below authorizes release of my
thesis to any reader upon request.
Redacted for privacy
Carol Ann Keller, Author
ACKNOWLEDGEMENTS
This thesis is dedicated to my grandmother, Monico Haywood, from whom I inherited
the stubbornness and perseverance necessary to succeed.
I would also like to thank Dr. Ayres for his continued support and encouragement
throughout this protracted engagement.
I would like to express my appreciation to my mother M. Arcile Boyes and my husband
Curt Keller for the emotional support they provided during what seemed like a never
ending process.
Lastly, I would like to thank Kris Holt, Syed Altaf, Kristi Engstrom, and Christine
Eskander for their technical assistance. I couldn't have done it without you.
TABLE OF CONTENTS
Page
Introduction
Chapter 1:
Fonnulation of a Sustained Release Acetaminophen
Product: From Concept to Production .............................................. 3
Abstract ...................................................................................................................... 4
Introduction ............................................................................................................... 5
Desired Characteristics in a Sustained Release Dosage Form ........................... 6
Pharmacokinetic Simulations ................................................................................. 9
Tablet Formulation and Testing ........................................................................... 36
Conclusions .............................................................................................................. 58
References ................................................................................................................ 59
Chapter 2:
Formulation of a Sustained Release Acetaminophen
Product: Determination of Biopharmaceutic and
Pharmacokinetic Properties ................................................................ 61
Abstract
62
Introduction ............................................................................................................. 64
Tablet Preparation and Testing
65
Subject Recruitment and Clinical Trials ............................................................... 70
Pharmacokinetic Model Fitting ............................................................................ 76
Tylenol Extra Strength
81
Tylenol Extended Relief........................................................................... 96
5% HPMC Sustained Release Product ................................................. 108
7.5% HPMC Sustained Release Product
121
TABLE OF CONTENTS (continued)
Page
Selection of a Release Acetaminophen Product for Phase
TwoClinical Trials ................................................................................................ 133
Conclusions ............................................................................................................ 140
References .............................................................................................................. 142
Chapter 3:
Formulation of a Sustained Release Acetaininophen
Product: Phase II Clinical Trials
143
Abstract .................................................................................................................. 144
Introduction ........................................................................................................... 147
StudyDesign .......................................................................................................... 158
Sample Size Calculation ....................................................................................... 162
Patient Recruitment and Enrollment ................................................................. 165
Pain and Disability Questionnaire ...................................................................... 187
StatisticalAnalysis ................................................................................................. 196
Conclusions ............................................................................................................ 201
References .............................................................................................................. 203
Conclusions ....................................................................................................................... 207
Bibliography ...................................................................................................................... 209
Appendices.................................................................................................................... 214
Appendix
2A
Copy of the Approved Application for Human Trials
to the Oregon State University Committee for the
Protection of Human Subjects ................................................... 214
Appendix
2B
Raw Saliva Concentration vs. Time Data for
Four Test Formulations in 10 Healthy
HumanSubjects ............................................................................ 226
TABLE OF CONTENTS (continued)
Appendix
Appendix
3A
3B
Page
Copy of the Second Application to the OSU
Investigational Research Board for the
Protection of Human Subjects
231
Copy of the Investigational review Board Application
to the Veterans Adninistration Hospital Human
Studies Committees
249
Copy of IND Send to the FDA ................................................. 272
Appendix
3C
Appendix
3D Raw Data From Questionnaires
314
LIST OF FIGURES
Page
Figure
1.1
Comparison of Published Data to Simulated Data for 1000mg of
Immediate Release Acetaminophen ........................................................................ 13
1.2
Simulations of Single Dose, Immediate Release Acetaminophen at
Different Overall Dosages ........................................................................................ 15
1.3A Simulated Plasma Concentrations for 650mg of Acetaminophen
Every6 Hours.17 ....................................................................................................... 17
1.3B Simulated Plasma Concentrations for 650mg of Acetaminophen
Every4 Hours ............................................................................................................. 18
1.3C Simulated Plasma Concentrations for 1000mg of Acetarninophen
Every6 Hours ............................................................................................................. 19
l.3D Simulated Plasma Concentrations for 1000mg of Acetaminophen
Every4 Hours ............................................................................................................ 20
1.4A Simulated Plasma Concentrations for 650mg of Acetaminophen
Every 4 Hours While Awake .................................................................................... 22
1.4B Simulated Plasma Concentrations for 1000mg of Acetaminophen
Every 4 Hours While Awake .................................................................................... 23
1.5
Simulated Plasma Concentrations for Single Dose, Zero-Order
Values ..................................... 25
Acetaminophen Formulations with Different
1.6
Simulated Plasma Concentrations for Multiple Dose, Zero-Order
Acetaminophen......................................................................................................... 27
Values.
Extended Relief Product ........................................................................................... 29
1.7
Published Serum Data for Tylenol Formulations with Different
1.8
Comparison of Published Serum Data for 1300mg of Tylenol
Extended Relief and 1000mg of Tylenol Extra Strength ..................................... 31
1.9
Comparison of Published Serum Data of 1300mg of Tylenol
Extended Relief to Tylenol Extra Strength After Scaling to
K0
1300mg ......................................................................................................................... 32
LIST OF FIGURES (continued)
Figure
Page
1.10 Simulated Plasma Concentrations for 1300mg of Tylenol Extended
ReliefEvery 3Hours ................................................................................................... 33
1.11 Dissolution Profiles for Four Acetaminophen Formulations
Containing25% HPMC ............................................................................................ 41
1.12 Effect of Polymer Concentration on Dissolution of Acetaminophen
Sustained Release Formulations ............................................................................... 45
1.13 Effect of Compression Force on Dissolution of Acetarninophen
Sustained Release Formulations ............................................................................... 47
1.14 Effect of Tablet Shape on Dissolution of Acetaminophen Sustained
ReleaseFormulations ................................................................................................. 50
1.15. Effect of Dosage Form Division on Dissolution of Acetaminophen
Sustained Release Formulations ............................................................................... 52
1.16 Effect of Granulation Method on Dissolution of Acetaminophen
Sustained Release Formulations ............................................................................... 55
2.1
Size and Shape of Tablets From Single Punch
TabletingMachine ...................................................................................................... 66
2.2
JIIPLC Saliva Profile for Subject Taking Acetaminophen Formulation ............. 73
2.3
Model #4: 1 compartment first order input, lag time, and first
orderelimination ........................................................................................................ 76
2.4
Model #12: 2 compartment first order input, micro-constants
as primary parameters, lag time, and first order elimination ................................ 77
2.5
Model #2: 1 compartment W-infusion (zero-order input),
no lag time, first order elimination .......................................................................... 78
2.6
Model #10:2 Compartment IV-Infusion (zero-order input), macroconstants as primary parameters, no lag time, first order elimination ................ 79
2.7
Graph of Tylenol Extra Strength Average Data fitted with a
1-compartment open model with equally weighted data points,
first order input, and first order elimination .......................................................... 85
LIST OF FIGURES (continued)
Figure
2.8
Page
Graph of Tylenol Extra Strength Average Data fitted with a
2-compartment open model with equally weighted data points,
first order input, and first order elimination .......................................................... 87
2.9
Graph of Tylenol Extra Strength Average Data fitted with a
1-compartment open model with data points weighted
I /y,first order input, and first order elimination ................................................... 93
2.10 Graph of Tylenol Extended Relief Average Data fitted
with a 1-compartment open model with equally weighted
data points, first order input, arid first order elimination ..................................... 98
2.11 Graph of Tylenol Extended Relief Average Data fitted with a
2-compartment open model with equally weighted data points,
first order input, and first order elimination ....................................................... 100
2.12 Graph of Tylenol Extended Relief Average Data fitted with a
1-compartment open model with data points weighted
l/y first order input, and first order elimination ................................................. 103
2.13 A: Published Average Plasma Concentrations for a 1000mg dose
of Non-Sustained Release Acetaminophen 500mg tablets compared
to Average Plasma Levels for a 1300mg dose of Sustained Release
Acetaminophen Bi-layered 650mg tablets in twelve Subjects ............................ 107
2.13 B: Data in a. after proportionally adjusting immediate release data to
a total acetaminophen dose of 1300mg ................................................................. 107
2.14 Graph of 5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 1-compartment open model with equally weighted
data points, first order input, and first order elimination ................................... 110
2:15 Graph of 5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 2-compartment open model with equally weighted
data points, first order input, and first order elimination .................................. 112
2.16 Graph of 5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 1-compartment open model with equally weighted
data points, zero order input from 0 to Tmax hours, and first order
elimination ................................................................................................................. 114
LIST OF FIGURES (continued)
Figure
Page
2.17 Graph of 5% J-IPMC Sustained Release Acetaminophen Average
Data fitted with a 2-compartment open model with equally weighted
data points, zero order input from 0 to Tmaxd hours, and first order
elimination ................................................................................................................. 116
2.18 Graph of 7.5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 1-compartment open model with equally weighted
data points, first order input, and first order elimination ................................... 124
2.19 Graph of 7.5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 2compartment open model with equally weighted
data points, first order input, and first order elimination ................................... 126
2.20 Graph of 7.5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 1-compartment open model with equally weighted
data points, zero order input from 0 to Ttnax hours, and first
orderelimination ..................................................................................................... 128
2.21 Graph of 7.5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 2-compartment open model with equally weighted
data points, zero order input from 0 to Tmaxda hours,
and first order elimination ..................................................................................... 130
2.22 Simulated Plasma Acetaminophen Concentrations for
Multiple Dosing of the 5% HPMC Sustained Release Acetarninophen
formulation ................................................................................................................138
2.23 Simulated Plasma Acetaminophen Concentrations for
Multiple Dosing of the 7.5% HPMC sustained Release Acetaminophen
formulation ............................................................................................................... 139
3.1
Diagram of physical changes that take place in an osteoarthritic knee ............ 148
3.2
Acetaminophen structure and metabolic pathways .............................................. 150
LIST OF TABLES
Page
Table
1.1
Summary of Pharmacokinetic Data for Acetaminophen ...................................... 9
1.2
Pharmacokinetic Values Selected for Simulations ................................................. 10
1.3
Dose/Size Formulation Relationships .................................................................... 39
1.4
Pre and Post Compression Weights of Tablets ..................................................... 40
1.5
Recipes for Acetaminophen Formulations Differing in
HPMCConcentration ............................................................................................... 42
1.6
Pre and Post Compression Weights for Tablets Differing
in HPMC Concentration ........................................................................................... 43
1.7
Pre and Post Compressions Weights for Tablets Differing by
CompressionForce .................................................................................................... 46
1.8
Size and Surface Area of Tablets Differing in Shape ............................................ 48
1.9
Percent Yield of Granules in the 14-20 Mesh Range for Three
GranulationMethods ................................................................................................. 56
1.10 Time of Granule Preparation for Three Granulation Methods .......................... 56
1.11 Ease of Scale Up for Three Granulation Methods ................................................ 57
2.1
Weight Variation Tolerances for Uncoated Tablets .............................................. 68
2.2
Summary of Subject Characteristics Including Age, Height,
Weight, and Gender ................................................................................................... 74
2.3
Random Treatment Assignments for the 10 Subjects .......................................... 75
2.4
Summary of pharmacokinetic parameters resulting from fitting Tylenol
Extra Strength® Data with a 1-compartment open model with equally
weighted data points, first order input., and first order elimination .................... 84
2.5
Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extra Strength® Data with a 2-compartment open
model with equally weighted data points, first order input, and first
orderelimination ........................................................................................................ 86
LIST OF TABLES (continued)
Page
Table
2.6
Comparison of Computer Fitted Parameters to Hand Calculated
Parameters ................................................................................................................... 88
2.7
Comparison of Fitted Pharmacokinetic Parameters to
LiteratureValues ......................................................................................................... 89
2.8
Summary of pharrnacokinetic parameters resulting from fitting
Tylenol Extra Strength® data with a 1-compartment open model
with the data points weighed 1/Y, first order input, and
first order elimination ................................................................................................ 92
2.9
Comparison of Estimated Cmax values for the 1-comparirnent
open models with different data points and weighing schemes .......................... 94
2.10 Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extended Relief® Data with a 1-compartment open model with
equally weighted data points, first order input, and first order
elimination ...................................................................................................................97
2.11 Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extended Relief® Data with a 2-compartment open model
with equally weighted data points, first order input, and first order
elimination ...................................................................................................................99
2.12 Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extended Relief® Data with a 1-compartment open model
with the data points weighed 1/Y, first order input, and
first order elimination ............................................................................................. 102
2.13 Summary of pharmacokinetic parameters resulting from fitting 5%
HPMC Sustained Release Acetaminophen with a 1-compartment
open model with equally weighted data points, first order input, and
first order elimination .............................................................................................. 109
2.14 Summary of pharmacokinetic parameters resulting from fitting 5%
HPMC Sustained Release Acetaminophen with a 2-compartment
open model with equally weighted data points, first order input,
andfirst order elimination ..................................................................................... 111
LIST OF TABLES (continued)
Page
Table
2.15 Summary of pharmacokinetic parameters resulting from fitting 5%
FIPMC Sustained Release Acetaminophen with a 1-compartment
open model with equally weighted data points, zero order input
from 0 to Tmax hours, and first order elimination ....................................... 113
2.16 Summary of pharmacokinetic parameters resulting from fitting S%
HPMC Sustained Release Acetaminophen with a 2-compartment
open model with equally weighted data points, zero order input
from 0 to Tmaxd hours, and first order elimination ........................................ 115
2.17 Summary of pharmacokinetic parameters resulting from fitting 7.5%
HPMC Sustained Release Acetaminophen with a i-compartment
open model with equally weighted data points, first order input,
and first order elimination ....................................................................................... 123
2.18 Summary of pharmacokinetic parameters resulting from fitting 7.5%
T-IPMC Sustained Release Acetaminophen with a 2-compartment
open model with equally weighted data points, first order input,
and first order elimination ..................................................................................... 125
2.19 Summary of pharmacokinetic parameters resulting from fitting 7.5%
F[PMC Sustained Release Acetaminophen with a 1-compartment
open model with equally weighted data points, zero order input
from 0 to Tmaxd hours, and first order elimination.
Tmaxwas defined as the time associated with the hightest
saliva concentration for each subject ..................................................................... 127
2.20 Summary of pharmacokinetic parameters resulting from fitting 7.5%
HPMC Sustained Release Acetaminophen with a 2-compartment
open mode! with equally weighted data points, zero order input
from 0 to Tmax hours, and first order elimination. Tmax was
defined as the time associated with the highest saliva concentration
for each subject. Some profiles could not be fit using this model ................... 129
3.1
Literature reports of acetaminophen toxicity and alcohol ................................. 152
3.2
Comparison of dose placement in the SR and
IRtreatment packets ................................................................................................ 158
3.3
Estimated standard deviation used for sample size calculation ........................ 163
LIST OF TABLES (continued)
Table
Page
3.4
Estimated magnitude of difference used for sample size calculation .............. 163
3.5
Estimated sample size for 2x2 crossover design used in study
sample size calculation ............................................................................................. 163
3.6
Estimated powers or probabilities of detection
used in sample size calculation ............................................................................... 164
3.7
Number of Patients Excluded from the Study
Categorized by the Exclusion Criteria................................................................... 167
3.8
Physician Reasons for Declining Enrollment ...................................................... 171
3.9
Patient Reasons for Non-enrollment into the Study ........................................... 172
3.10 Home City of 103 Declined Patients who Stated
"Too far to Drive" as the Reason for not Enrolling in the Study ..................... 173
3.11 Estimated cost of Study ........................................................................................... 176
3.12 Demographics of 30 enrolled Patients .................................................................. 178
3.13 Distribution of enrolled patients by Severity and Radiological
Grading of the Osteoarthritic Disease .................................................................. 179
3.14 Incidence of Side Effects to the Study Medication by Formulations ............... 181
3.15 Number of Tablets Missed by Patients
During the Study Treatments ................................................................................. 183
3.16 Number of Rescue Analgesic Tablets
Needed by Patients during the Study Treatments ............................................... 184
3.17 Measured Saliva Acetaminophen Levels
inStudy Samples .......................................................................................................185
3.18 Average Score on Question I by Treatment Group .......................................... 187
3.19 Average Score on Question 2 by Treatment Group........................................... 188
3.20 Average Score on Question 3 by Treatment Group........................................... 188
LIST OF TABLES (continued)
Table
Page
3.21 Average Score on Question 4 by Treatment Group ........................................... 189
3.22 Average Score on Question 5 by Treatment Group ........................................... 190
3.23 Average Score on Question 6 by Treatment Group ........................................... 190
3.24 Average Score on Question 7 by Treatment Group ........................................... 190
3.25 Average Score on Question 8 by Treatment Group ........................................... 190
3.26 Average Score on Question 9 by Treatment Group ........................................... 191
3.27 Average Score on Question 10 by Treatment Group ......................................... 192
3.28 Average Score on Question 11 by Treatment Group ......................................... 193
3.29 Percentage of Side Effects Occurring by Treatment .......................................... 194
3.30 Average Time to Walk 50 Feet by Treatment ...................................................... 195
3.31 Results of the Signed Rank Test Comparing the Immediate Release
Acetaminophen Treatment to the Sustained Release Treatment ...................... 196
3.32 Results of the Signed Rank Test Comparing the Sustained Release
Acetaminophen Treatment to the Baseline Treatment ...................................... 199
LIST OF APPENDICES
Appendix
2A
Appendix
2B Rw Saliva Concentration vs. Time Data for
Page
Copy of the Approved Application for Human Trials
to the Oregon State University Committee for the
Protection of Human Subjects ................................................... 214
Four Test Formulations in 10 Healthy
HumanSubjects
226
Appendix
3A
Copy of the Second Application to the OSU
Investigational Research Board for the
Protection of Human Subjects ................................................... 231
Appendix
3B
Copy of the Investigational review Board Application
to the Veterans Administration Hospital Human
Studies Committees ...................................................................... 249
Appendix
3C
Copy of IND Send to the FDA ................................................. 272
Appendix
3D Raw Data From Questionnaires ................................................. 314
DEVELOPMENT AND TESTING OF A SUSTAINED RELEASE
ACETAMINOPHEN TABLET FOR THE TREATMENT OF CHRONIC PAIN IN
OSTEOARTHRITIS PATIENTS
INTRODUCTION
Osteoarthritis affects nearly 10 % of the population over age 60 and is second only to
cardiovascular disease in causing severe chronic pain and disability. These patients suffer
from increasing disability and chronic pain. Acetaminophen has been shown to be effective
in relieving the pain caused by osteoarthriiis, but the dosing interval is inconvenient (every 4-
6 hours) and chronic use of high doses of acetaminophen are associate with hepatic toxicity.
These research was designed to use both the pharmacodynamic properties and
pharmacokinetic parameters of acetaminophen to design a sustained release dosage form of
acetaminophen to relieve chronic pain in osteoarthritis and other chronic pain patients.
Chapter 1 describes the design and testing of several sustained release acetaminophen
formulations. Formulations are hydrophilic matrix tablets made with
hydroxypropylmethylcellulose (HPMC) and are tested using standard dissolution techniques.
Investigations into tablet size, tablet shape, HPMC content, amount of drug, and tablet
divisibility were performed. Two promising formulations were then selected for
pharmacokinetic characterization in human subjects.
Chapter 2 describes the pharmacokinetic characterization of the 5% and 7.5% HPMC
formulations of acetaminophen. Tylenol Extra Strength and Tylenol Extended Relief tablets
were used as reference formulations. Each of the formulations was administered to ten
healthy human subjects and saliva concentrations were measure. The saliva data was used to
2
characterize the pharmacokinetic parameters of each formulation. The 5% HPMC sustained
release formulation was selected for testing in the target population.
Chapter 3 describes the double blind, placebo controlled crossover study conducted
comparing four grams of immediate release acetaminophen per day to 2.6 grams of sustained
release acetaminophen per day in patients with osteoarthritis of the knee. Patients with
osteoarthritis were recruited from the Veterans Administration Outpatient clinic.
Performance of the products was tested by a twelve question questionnaire and a timed
walking test. The sustained release acetaminophen formulations was compared to the
immediate release formulation as well as to the baseline treatments to determine efficacy in
these patients.
CHAPTER 1
FORMULATION OF A SUSTAINED RELEASE ACETAMINOPHEN
PRODUCT: FROM CONCEPT TO PRODUCTION
ABSTRACT
Acetaminophen has been safely used for analgesia for many years. Literature
suggests that a plasma acetaminophen level of 5mg/L is necessary to maintain
analgesic relief in humans. Current dosing regimens are inconvenient (every 4-6
hours). Simulations were conducted to examine various doses and input rates for
sustained release formulation of acetaminophen. Once parameters were selected
from the simulations, sample formulations were prepared and tested. Investigations
into dose/size relationships, hydroxypropylmethylcellulose (FIPMC) percentage for
erosion matrix tablets, compression force, tablet shape, tablet divisibility, and
granulation methods were performed for non-disintegrating hydrophilic matrix
tablets. Dose/size ratios for tablets ranging from 500mg to 650mg were investigated
and tablets with 650mg of acetaminophen were selected as being an acceptable size.
Drug release from tablets was inversely related to increasing HPMC percentage.
Compression force of 4,000-10,000 pounds did not affect drug release from tablets.
Drug release from substantially different shaped tablets was related to surface area of
the dosage form as suggested by the Noyes-Whitney equation. Drug release from
tablet halves was not significantly different then from intact tablets. Two wet
granulation methods and one slugging technique were investigated. Methods were
evaluated for percent yield of granules of proper size, time/labor involvement, and
ease of scale-up. A preliminary formulation that met the simulation goals was selected
for further study.
INTRODUCTION
Acetaminophen has been safely used as an effective analgesic and anti-pyretic
medication for many years. While effective, acetaminophen use in chronic pain has
been limited by dose related toxicity and the short half-life of the drug. Current
immediate release dosage forms must be administered every 4-6 hours to maintain
analgesia. The goal of this research was to use new phannacodynamic data in
conjunction with existing pharmacokinetic data to develop sustained release
acetaminophen tablets for use in chronic pain. This chapter describes development
and in vitro testing of a sustained release acetaminophen formulation and provides
insight into rational drug design based on pharmacokinetic parameters.
6
DESIRED CHARACTERISTICS IN A SUSTAINED
RELEASE DOSAGE FORM
The first step in rational drug design is to identify the desired characteristics of
the finished formulation. Goals should be set for the minimum plasma concentration
of drug, dosing interval, overall daily dose, drug release characteristics, and
formulation appearance and palatability. Considerations for this acetaminophen
formulation include:
1.
Published pharmacokinetic data suggests that a plasma acetaminophen level of
3mg/L must be maintained for anti-pyretic activity and a level of 5mgIL must be
maintained for analgesic effect1. The steady state minimum (Ctnin) plasma
concentration goal for this formulation is 5mg/L.
2.
The dosing interval should be once or twice daily for best patient compliance.
Since this formula is being developed for chronic pain and is likely to become an
ongoing medication, patient convenience is a significant factor in clinical treatment
response.
The overall daily dose should be minimized. Current maximum daily dose
recommendations for acetaminophen are 4 grams/day25. Recent studies have
expressed concern that even 4gms/day is too much acetaminophen and can result in
chronic hepatotoxicity. The desired sustained release acetaminophen formulation
would therefore contain less than 4gms/day. The Food and Drug Administration is
currently investignting new recommendations for the maximum overall daily dose of
acetaminophen.
7
Preliminary results suggest a new overall daily dose recommendation of
2.6gm/day of acetaminophen for chronic use67. Goal overall daily dose for the new
formulation should therefore fall at or below 2.6gm/day.
4.
Drug release characteristics from the formulation are in large part a reflection
of the type of dosage form selected. Zero-order release of the medication would be
ideal, however true zero-order release is difficult to achieve. Zero order release
provides the most constant plasma concentrations of medication and allows the
formulator to minimize the overall dose needed. Osmotic pumps are currently the
only true zero order release formulations on the market. Their manufacture requires
complex technology and expensive equipment which are not generally available.
Realizing this limitation, true zero-order release is not a feasible reality for this
product.
Pseudo zero order release can often be obtained with coated beads inside a
capsule. This approached is limited by the amount of volume occupied by the beads
and the amount of dead-space found within the capsule. This approach is not
feasible for an acetaminophen formulation with one capsule because of the high total
dose that must be delivered.
Most sustained release formulations are a blend of first and zero order release
characteristics. Compressed hydrophilic polymer tablets exhibit this type of release.
They are a logical choice for formulators wishing to deliver large doses, as the
compression minimizes any dead space in the formulation. Hydrophilic polymers,
such as hydroxypropylmethylcellulose (HPMC), are readily available in a variety of
molecular weights and purities and require no special manufacturing equipment.
Tt was decided that this type of formulation would be best suited for a sustained
release acetaminophen formulation.
5.
Appearance and palatability are also important especially when dealing with
chronically administered medications. The tablets must be of a size and shape
conducive to swallowing with little or no perceivable taste. As acetaminophen is a
bitter compound, coating of the finished product must be considered.
PHARMACOKINETIC SIMULATIONS
Once a general profile of the desired formulation is obtained, pharmacokinetic
simulations may be performed to ftirther identify desired release characteristics of the
formulation. Table 1.1 is a summary of the some pharmacokinetic data found in the
literature for acetaminophen.
Table 1.1: Summary of Pharmacokinetic Data for Acetaminophen
Parameter
Ref
Ref 2''
Ref 3a1O
Ref 411
Ref 511
S
1.0
1.0
1.0
1.0
1.0
F
0.88
C, (mg/L)
8.0
9.3
6.8
0.7
0.9
tmax
(h)
0.5
t112
(h)
1.8
1.8
1.8
2.0
1.97
k
(h4)
0.385
0.376
0.39
0.346b
0.351b
ka (h1)
3.25
2.20
Vd (L/kg)
0.86
0.95
0.89
1
a.
These references quote data for children of various ages. Several references
state that the pharmacokinetic parameters do not significantly differ for
children over 1 year and adults, once adjusted for weight.
b.
Calculated from the t112 using the formula k = ln 2/ tI!2.
Table 1.2 contains parameter values selected for pharmacokinetic simulations.
They were selected as values which are representative of the literature values.
10
Table 1.2: Pharmacokinetic Values Selected for Simulations
Parameter
t112
kei
(Ii)
(})
Selected Value
1.8
0.385
ka (h4)
3.25
Vd EL/kg)
0.86
F
1.0
S
1.0
Several assumptions were made and some parameters were set based on the
desired dosage form parameters discussed earlier. Simulations were performed using
PSIPLOT assuming both zero order and first order release from the formulation.
This was done with the realization that actual release from the formulation would be
not a single release mechanism but a combination of both. It is also understood that
these simulations represent a starting point for the formulation and are not intended
to predict exact performance of any formulation. Simulations were performed for a
variety of single dose and multiple dose situations using the equations listed below.
Assumptions remaining constant throughout the simulation process are:
Maximum gastric transit time of any given tablet is 12 hours. After this time
the tablets are assumed to have passed out of the gastrointestinal tract and contribute
no further input into the system.
2.
The average adult weight is assumed to be 70kg. This may not be an accurate
representation of the average weight of Americans in the 1990's, but it has historical
precedent as the ideal "Goodman and Gilman" person.12
11
The desired dosing interval (t) is set at 12 hours. Once daily dosing was
3.
briefly investigated, however the dose needed per tablet proved to be prohibitive.
Some simulations of currently available immediate release products were done for
companson purposes.
Equation A: Single Dose, First Order Input13'14
= (S) (F) (D) (k *
(Vd) (wt) @c-kei)
Where
C,
F
= the plasma acetaminophen level at any time t (mg/L)
= the fraction of the dose absorbed
thesaltformofthedrug
S
D
= the dose given (mg)
Vd = the apparent volume of distribution of the drug within the body (L/kJ
wt = weight of patient (kg)
the apparent elimination rate constant
kei
the observed absorption rate constant 1)
k
t
= the time elapsed since administration (h)
1)
Equation B: Single Dose, Zero Order Input13'14
=
(S) (U) (D)
* (1-e')
(t) (Yd) (wt)
K0
is known as the zero-order input rate constant for this equation and is equal to the
total dose of acetaminophen to be delivered divided by the selected value of 'r. For
example, the
K0
for 1500mg of acetaminophen dosed every 12 hours would be equal
to l500mg/12 hours = 125mg/hour.
Multiple dose plots were obtained by addition of the C, contribution of each
individual dose (superposition
method).15
After 12 hours, input from a given dose
12
stopped and any remaining contribution from that dose was allowed to decay
exponentially in the simulation.
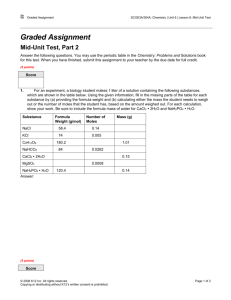
Figure 1.1 is a comparison of a drug concentration vs. time curve from a
simulated 1000mg immediate release dose to published plasma
data16
for the same
dose. Although not identical, the simulation has the same C, (12.lmg/L) and t
(1
hour) as the published data. Unfortunately, the published data are an average of 12
subjects and the standard deviation information for these values was not included in
the publication. Both the simulated curve and the published curve fall below the
target plasma concentration of 5mg/L at slightly over 3.5 hours following
administration of the dose.
13
Figure 1.1: Comparison of Plasma Data to Simulated Data for 1000mg of
Immediate Release Acetaminophen
14
--PUBLIS}IED AVERAGE
12
-9E-SIMULATED DATA
10
0
U
0
U
0
2
4
6
Time (h)
8
10
12
14
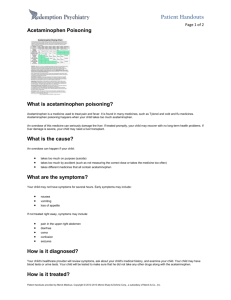
Figure 1.2 is a graph of several simulated immediate release curves that differ
only in the overall dose delivered. All other pharinacokinetic parameters were kept
constant. The 500mg dose barely reaches above the target plasma concentration of
5mg/L, and even drug concentrations from the 2000mg dose falls below 5mg/L soon
after 5 hours. Keep in mind that these simulations are single doses only and that
multiple dosing of the formulations will result in higher (but not necessarily effective)
steady state plasma concentrations of drug. The currently available over the counter
products recommend 650-1000mg every 4-6 hours.
15
Figure 1.2: Simulations of Single Dose, Immediate Release Acetaminophen at
Different Overall Dosages
,15
0
U
U
0
C)
10
10
Time (h)
12
16
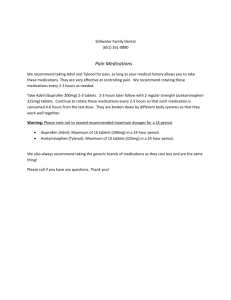
Figures 1.3A-D show simulations for the recommended multiple dosage
regimens. The simulation for 650mg every 6 hours (Figure 1.3A) represents the
lowest recommended dosing regimen. Upon multiple dosing, the plasma drug
concentration is above the target level for only 40% of the dosing interval. The
remaining 60% of the time there is a potential for recurring pain. The product is subtherapeutic for 3.6 hours during each dosing interval or a total of 14.4 hours per day.
By increasing the dosing frequency to 650mg every 4 hours (Figure 1.3B) the product
performs slightly better but still falls below the target plasma concentration for 37%
of the dosing interval. The product is sub-therapeutic 1.5 hours out of each dosing
interval or 8.8 hours a day. It also has the inconvenience of requiring the patient to
take the product 6 times a day! As the dose is increased to 1000mg every 6 hours
(Figure 1.3C) the performance is about the same as the 650mg dose every 4 hours.
The 1000mg every 6 hours dose has the advantage of being slightly more convenient
for the patient because it only needs to be taken 4 times a day rather than 6 times a
day. However, it still falls below the target plasma concentration for 37% of the
dosing interval, and therefore still has the potential for recurring pain during this time.
That's 2.2 hours per dose or 8.8 hours per day. The 1000mg every 4 hours regimen
(Figure 1.3D) is the only dosing regimen to maintain the target plasma concentration
for the entire dosing interval. Unfortunately it must be taken all day and night, and at
6 grams of acetaminophen per day, it has exceeded the maximum recommended daily
dose of acetaminophen2 and may cause hepatotoxicity.
17
Figure 1.3A: Simulated Plasma Concentrations for 650mg of Acetaminophen
Every 6 Hours
10
9
8
7
0
5
V
U
0
3
2
11
0
0
5
10
15
20
25
Thne (I-i)
30
35
40
45
50
18
Figure 1.3B: Simulated Plasma Concentrations for 650mg of Acetaminophen
Every 4 Hours
12
10
I
10
15
20
25
Time (h)
30
35
40
45
50
19
Figure 1.3C: Simulated Plasma Concentrations for 1000mg of Acetaminophen
Every 6 Hours
14
10
16
[2!
2
0
0
5
10
15
25
Thne@)
30
35
40
45
50
20
Figure 1.3D: Simulated Plasma Concentrations For 1000mg of Acetaminophen
Every 4 Hours
16
14
12
0
U
0
U
10
15
25
Time (1-i)
30
35
40
45
50
21
All of the above simulations assume that the dosing regimen is followed
exactly and around the clock. In real life, patients rarely get up during the night to
take medication. A more realistic simulation of patient use is shown in Figures 1.4A-
B. These simulations display expected plasma concentrations when the patients take
650mg or 1000mg every 4 hours while awake. During the "night" the plasma
concentrations decline to near zero. While this may be acceptable for acute pain,
chronic pain suffers awake with little or no pain relief at a time when patients often
notice the pain most.
22
Figure 1.4A: Simulated Plasma Concentrations for 650mg of Acetaminophen
every 4 Hours \Thile Awake
12
10
C
U
0
0
5
10
15
20
25
Time (h)
30
35
40
45
50
23
Figure 1.4B: Simulated Plasma Concentrations for 1000mg of Acetaminophen
Every 4 Hours While Awake
16
14
12
10
V
U
C
U
10
15
3)
25
Time (Ii)
30
35
40
45
50
24
The ideal sustained release formulation would provide a constant level of drug
for the entire dosing interval, thus avoiding the potential for breakthrough pain
between doses or the loss of efficacy during the night As mentioned before, true
zero-order release formulations might provide this type of release. Using the same
pharmacokinetic parameters as were used in the immediate release simulations, several
zero-order release simulations were performed. There are no published data for this
type of acetaminophen formulation, so the accuracy of the simulations cannot be
compared to published data.
Figure 1.5 shows a single dose of 5 different zero-order products. All
variables in the simulations are the same, only
K0
changes. Recall that
K0
is the zero
order input constant and is equal to the total dose/dosing interval. In this figure, two
of the formulations reach the target plasma concentration. Both the 2000 mg dose
(K0
= 166.6mg/hr) and the 1300mg dose (K.
108.3mg/hr) reach or exceed
5mg/L. The 2000mg dose has the advantage of reaching the target about 5.5 hours
sooner than the 1300mg dose. The 1300mg dose has the advantage of allowing
compliance with the new maximum daily dose recommendations of 2.6 grams per
day. Neither product would be acceptable for acute pain because of the lag time (2.5
hours for the 2000mg dose and 8 hours for the 1300mg dose) before reaching the
desired target plasma concentration.
25
Figure 1.5: Simulated Plasma Concentrations for Single Dose, Zero-Order
Acetaminophen Formulations With Different Ko Values
9
-- 500MG
650MG
8
-*-. 1000MG
-*- 1300MG
_i
7
I2000MG
Q5
(3
0
2
4
6
Time (h)
8
10
12
26
Figure 1.6 depicts plasma simulations for the zero order formulations when
dosed every 12 hours. With chronic use and consistent dosing, the 1300mg every 12
hour product maintains a plasma steady state concentration of just slightly above the
target plasma concentration. It also provides a constant plasma concentration
throughout the day and night, potentially providing relief in the morning as well as
when the patient is awake.
27
Figure 1.6: Simulated Plasma Concentrations for Multiple Dose (q 12h), ZeroOrder Acetaininophen Formulations With Different Ko Values
9
8
4-500MG
*-650MG
7
-- 1000MG -* 1300MG
* 2000MG
bID
2
1
0l
0
5
10
15
20
25
Time (h)
30
35
40
45
50
28
During the simulation process, a new commercial product was released onto
the market. Named Tylenol Extended Relief, the product contains 650mg of
acetaminophen in each tablet. One half of that dose (325mg) is a traditional
immediate release formulation. The second half of the dose (325mg) is present in a
hydrophilic matrix for extended release. The two halves are compressed together to
form a bi-layered caplet. The recommended dose is 1300mg every 8 hours. Figure
1.7 is from published plasma data for the product1. The data represent an average of
twelve patients. The product rapidly reaches the target plasma concentration in about
0.5 hours, but after 5.5 hours, it falls below the target.
29
Figure 1.7: Published Serum Data for Tylenol Extended Relief Product
14
12
10
I
10
Thie
)
12
30
To better compare this product to the immediate release product previously
studied, Figures 1.8 through 1.10 were prepared. Figure 1.8 compares the published
data for 1300mg of Tylenol Extended Relief (2 x 650mg tablets) to published data for
I000mg of Tylenol Extra Strength (2 x 500mg tablets). Both curves represent an
average of twelve patients. Patients fasted 8 hours prior to each dose. As expected,
the Tylenol Extended Relief (which contains a larger dose) has a slightly broader and
slightly higher peak. The hydrophilic matrix portion of the tablet slows release just
enough to cause slight broadening and delaying of the C. Reported values for the
average area under the curve (AUC) are 64.3 for the Extended Relief product and 49.5
for the Extra Strength product. Again, this agrees with what is expected given the
difference in dose. Pharmacokinetic theory dictates that the increase in AUC should
be proportional to the increase in dose for drugs that follow linear pharinacokinetics.
In this case the ratio of the AUC for the Extended Relief product to the Extra
Strength product is 64.3/49.5
1.29. The ratio of the dose for the Extended Relief
product to the dose of the Extra Strength product is l300mg/l000mg = 1.3. This
confirms that linear pharmacokinetics are at play in this situation.
31
Figure 1.8: Comparison of Published Serum Data for 1300mg of Tylenol
Extended Relied and 1000mg of Tylenol Extra Strength
14
-4--TYLENOL EXTENDED RELIEF 1300MG
12
-.-TYLENOL EXTRA STRENGTH 1000MG
10
0
I
0
2
10
Time (h)
12
32
Figure 1.9: Comparison of Published Serum Data for 1300mg of Tylenol
Extended Relief to Tylenol Extra Strength After Scaling to 1300mg
16
14
-4--TYLENOL EXTENDED RELIEF 1300MG
12
-*---TYLENOL EXTRA STRENGTH SCALED TO
1300MG
I:
10
Time (h)
12
33
Figure 1.10: Simulated Plasma Concentrations for 1300mg of Tylenol Extended
Relief Every 8 Hours
16
14
12
10
10
15
20
25
Time (h)
30
35
40
45
50
34
Since both products follow linear pharmacokinetics, it is reasonable to scale
the 1000mg curve up to a 1300mg curve by multiplying all plasma values by 1.3. The
comparison of the resulting curve to the 1300mg Tylenol Extended Relief curve can
be seen in Figure 1.9.
Although the Tylenol Extra Strength has a higher C
(l6mg/L as compared
to l3mg/L for Tylenol Extended Relief) the elimination portions of the curves are
essentially identical. This suggests that once adjusted for the difference in dose, the
formulations release drug nearly identically. The hydrophilic portion of the Tylenol
Extended Relief tablets does not substantially alter the release characteristics of the
tablet. The difference in performance of the two products is a result of the difference
in dose.
Figure 1.10 is a simulation of 1300mg of the Tylenol Extended Relief product
dosed every 8 hours as directed by the manufacturer. For 24% of the dosing interval
(almost 2 hours per dose or 6 hours per day) the curve
falls
below the target plasma
concentration in spite of the larger dose administered.
It is interesting to note that the manufacturers elected to
call
the product
"Extended Relief' rather than use a term such as sustained or controlled release. The
Food and Drug Administration describes the term "Extended" as referring to dosage
forms that increase the dosing interval less than 2 limes the dosing interval of the
immediate release product17. It goes on to describe the terms "Sustained" or
"Controlled" as referring to dosage forms that extend the release of the drug greater
then or equal to 2 times the dosing interval of the immediate release product. Since
35
the Tylenol Extended Relief product extends the dosing interval for only 2 hours (4-6
hours to every 8 hours), it is referred to as extended release and not sustained or
controlled release. If successful, the target product of this research would extend the
dosing interval from 4-6 hours to 12 hours, thus earning the title "sustained or
controlled" release.
36
TABLET FORMULATION AND TESTING
Tablet Ingredients:
All chemicals used in the production of tablets were National Formulary
(NF)/United States Pharmacopeia (USP) grade. They include acetaminophen
NF/USP (Spectrum Chemical Mfg. Corp., Gardena, CA) Lot JE321,
polyvinylpyrrolidone K-30 NF/USP (Spectrum Chemical Mfg. Corp., Gardena, CA)
Lot KD186, Magnesium Stearate NF/USP (Spectrum Chemical Mfg. Corp., Gardena,
CA) Lot KC502, and Methocel K100M PREM CR brand of
hydroxypropylmethylcellulose (Dow Chemical Co., Midland, MI) Lot MM92101105K.
Dry ingredients were sifted together and then compressed into tablets.
Tablet Compression:
Tablets were compressed in a Carver press using a caplet shaped punch and
die. The requisite amount of powder was weighed, loaded into the carver press, then
tablets were compressed at 5,000 lbs for 30 seconds. After removal, each tablet was
again weighed and a post-compression weight was recorded.
Dissolution Parameters:
All dissolution testing used the USP Paddle method. Tablets were exposed to
a 2 hour simulated gastric fluid pre-treatment followed by 22 hours exposure to
simulated intestinal fluid. Temperature was maintained at 37 degrees C and paddles
rotated at 60 rpm. Samples were collected with replacement at 20 mm, 40 mm, I h, I
h 20 mm, 1 h 40 mm, and 2 h. After changeover to intestinal fluid, additional samples
37
were taken at 3 h, 4 h, 6 h, 9 h, 12 h, and 24 h. Changeover was accomplished by
filtering each flask using vacuum filtration and returning collected tablets to the new
flask. Sample containers were covered in foil to protect the drug from UV
degradation and stored in the refrigerator until UV analysis. Simulated gastric fluid
and simulated intestinal fluid were prepared using the following recipes:
Simulated Enzyme-Free Gastric Fluid (4 L)
Distilled, deionized water
NaCl
HC1 acid
3.5L
8g
28ml
adjust pH to 1.4 + or 0.1
qs with distilled, deionized water
4.OL
Simulated Enzyme-Free Intestinal Fluid (4 L)
0.2N NaOH (2g/250ml)
760m1
K2HPO3
Distilled, deionized water
27.2g
3.5L
adjust pH to 7.4 + or - 0.1
qs with distilled, deionized water
4.OL
Note: It is important to adjust the pH of the intestinal fluid when it has a total
volume of 3.5L as it often requires significant adjustment to bring it into the correct
pH range.
38
UV Analysis:
Proper dilution of the samples was determined using a Beer's Law calculation.
Beer's Law:
A = (&) (c) (1)
where A = absorbance
= molar absorptivity
c = molar concentration
= path length
For best results the maximum absorbance should be less than or equal to 1. The path
length is a constant 1 cm, and the molar abs orptivity of acetaminophen is listed in the
Merck Index18 as 13,800 L/mol* cm.
The desired dilution concentration can therefore be calculated as:
A=
(E)(c)(l)
I = (13,800 L/mol * cm) (c) (1 cm)
rearranging to obtain
c = 0.000072464 mol/L = 1 lmg/L acetaminophen
Analyzed samples should therefore be diluted to a concentration of less than or equal
to Ilmg/L.
Most dissolutions involve 650mg acetaminophen in 900 ml of dissolution
fluid, or lower concentrations. If completely dissolved, the resulting concentration is
0.7222mg/mi or 722mg/L. For the samples to be in the correct concentration range
for analysis they should be diluted 1:100. Samples were diluted 1:100 with distilled,
deionized water and analyzed on a Hewlett Packard 8452A Diode Array variable
wavelength UV-VIS spectrophotometer set at 244nm.
39
Sample absorbance values are compared to absorbance values produced by
acetaminophen standards of lmg/L, 2mg/L, 4mg/L, 6mg/L, 8mg/L, and lOmg/L
also made in distilled, deionized water.
Data Analysis:
All data were analyzed using the PSI-PLOT spreadsheet and graphics
program.
Investigations into Dose/Tablet Size:
Based on previous work in this laboratory a formulation containing 25%
hydroyxypropylmethylcellulose was chosen as a starting formulation. The dose/size
relationship of the tablets was not known at this time. The percentage of magnesium
stearate, polyvinylpyrrolidone, and HPMC was kept constant throughout the
formulation, and the total dose of acetaminophen was varied from 500mg to 650mg
per tablet.
Four tablets of each formulation were made. The formulas and sizes are
shown below.
Table 1.3: Dose/Size Formulation Relationships
Formula A
Formula B
Formula C
Formula D
181.0mg
199.0mg
217.0mg
236.0mg
Mg Str (1%)
7.2mg
7.9mg
8.7mg
9.4mg
PVP (5%)
36.0mg
40.0mg
43.0mg
47.0mg
APAP (69%)
500.0mg
550.0mg
600.0mg
650.0mg
Tab wt.
724.2mg
796.9mg
868.7mg
942.4mg
Length
Height
19.0mm
19.0mm
19.0mm
19.0mm
3.0mm
4.0mm
5.0mm
6.0mm
HPMC (25%)
40
Table 1.4: Pie and Post Compression Weights of the Tablets
Formulation
A
B
C
D
Tablet
Precompression wt.
(mg)
Postcompression wt.
(mg)
1
725
717
2
724
718
3
724
719
4
725
724
1
798
797
2
797
796
3
798
796
4
797
795
1
869
867
2
868
865
3
870
865
4
870
869
1
944
941
2
942
942
3
942
942
4
943
940
Dissolution was performed on two tablets of each formulation. Results were
compared with two Tylenol Extra Strength tablets (500mg per tablet) and two
Tylenol Extended Relief tablets (650mg per tablet). Figure 1.11 shows dissolution
results for the formulations. The size of all of the tablets is acceptable in terms of
swallowability, but it is noted that all of the sustained release formulations only
released about 70% of the
total
drug in 24 hours. All tablets of the commercial
41
product released 100% of the total dose by the 20 minute sample for the immediate
release product and before the 1 hours sample for the extended relief product.
Incomplete release from the new formulations is probably due to too much HPMC in
the formulation. Other potential causes include too much compaction force and a
HPMC product with too high of a molecular weight. It is obvious that further
investigation into the proper J-IPMC quantity were needed.
Figure 1.11: Dissolution Profiles for Four Acetaminophen Formulations
Containing 25% HPMC
500
450
400
350
300
I
250
200
150
---FORMULATION A --FORMULATION B
100
4J4 -k--FORMULATION C
0
2
4
6
8
10
12
Time (h)
14
-4--FORMULATION
16
18
20
22
24
42
Investigations into HPMC Polymer Concentration:
Results of the previous investigation suggest that 25% HPMC prevented
complete release of drug from the formulation. Formulations were prepared
containing 2.5%, 5%, 7.5%, 100/n, 12.5%, and 15% HPMC. The amount of drug per
tablet was fixed at 650mg and the relative amounts of PVP and magnesium stearate
were maintained at 5% and 1%, respectively. Four tablets of each formulation were
made using the Carver press and pre and post compression weights of each tablet
were recorded. Dissolution was performed on two tablets of each formulation. Two
tablets of Tylenol Extra Strength and two tablets of Tylenol ER were also analyzed
for comparison. The data are as listed in Tables
1.5 and 1.6.
Table 1.5: Recipes for Acetaminophen Formulations Differing by HPMC
Concentration
% HPMC
APAP (mg)
PVP (mg)
HPMC (mg)
(mg)
Total
tab wt.
Mg Str
2.5%
650
35.5
17.8
7.1
710.4
5.0%
650
36.5
36.5
7.3
730.3
7.5%
650
37.6
56.4
7.5
751.5
10.0%
650
38.5
77.4
7.7
773.6
12.5%
650
49.8
99.7
7.9
809.5
15.5%
650
41.1
123.4
8.2
822.7
43
Table 1.6: Pre and Post Compression Weights for Tablets Differing in HPMC
Concentration
%HPMC
2.5%
5.0%
7.5%
10.0%
12.5%
15.0%
Tablet #
I
Precompression wt.
(ing)
Postcompression wt.
(mg)
1
714
702-capped
2
714
711
3
715
711
4
714
708
1
735
729
2
734
729
3
734
712-capped
4
733
725
1
754
751
2
753
752
3
755
747
4
755
749
1
775
770
2
778
771
3
778
768
4
775
772
1
814
808
2
815
811
3
815
807
4
815
812
1
822
819
2
823
820
3
822
819
4
822
818
44
Figure 1.12 shows the effect of HPMC amount on the release of
acetaminophen from tablets. The goal is complete but controlled release of the drug
over a 12 hour period. The formulation that most closely fulfills those requirements is
the 7.5% formulation. It provided about 90% drug release at 12 hours and shows well
controlled release throughout the time period. The 2.5 and 5% formulations provide
complete release by 3.5 and 8 hours respectively. The 10, 12.5 and 15% formulations
do not completely release the acetaminophen even after 24 hours. The 7.5% HPMC
formulation was therefore selected for further testing.
45
Figure 1.12: Effect of Polymer Concentration on Dissolution of Acetaminophen
Sustained Release Formulations
100
90
so
70
a)
a)
60
50
a)
40
L)
30
2.50%
5.00%
20
10
0
2
4
6
8
10
47.50%
* 10.00%
3*-- 1230%
+ 15.00%
12
Time (h)
14
16
18
20
22
24
46
Effect of Compression Force on Acetaminophen Release:
Once a formulation had been selected, the effects of compression force on
release of drug from the tablet were investigated. Sufficient powder was mixed of the
7.5% FIPMC formulation to make 20 tablets. Three tablets each were produced using
30 seconds of compression at 4,000, 5,000, 6,000, 7,000, 8,000, and 10,000 pounds of
pressure. Dissolution testing was performed on 2 tablets of each.
Table L7: Pre and Post Compression Weights for Tablets Differing by
Compressions Force.
Compression
force (Ibs)
5,000
6,000
7,000
8,000
10,000
Tablet #
Precompression wt.
(mg)
Postcompression wt.
(mg)
1
754
750
2
755
753
3
754
749
1
754
752
2
753
751
3
755
752
1
753
749
2
754
751
3
754
752
1
755
754
2
754
753
3
754
752
1
753
749
2
753
750
3
754
750
1
753
750
2
754
751
3
755
753
As shown in Figure 1.13, dissolution profiles from the tablets were virtually
superimposable. The results teach that compression force does not significantly
47
affect drug dissolution between 4,000 and 10,000 pounds force. These results are
consistent with findings of others using HPMC matrix tablets 19
Figure 1.13: Effect of Compression Force on the Dissolution of Acetaminophen
Sustained Release Formulations
100
90
80
70
60
50
40
U
S
4,000lb
5,000lb
è--6,000b
)-7,000lb
30
20
*-.- 8,000lb
-_
10,000lb
10
OU
0
5
10
15
Time (h)
20
25
30
48
Investigations into Tablet Shape:
The overall rate of drug dissolution from a non-disintegrating dosage form
can often be described by the Noyes-Whitney
Equation20.
c. = (D) (A) (K (C,-C)
h
dt
where dc/dt
rate of drug dissolution
D = diffusion rate constant
A
surface area of the particle or dosage forms
K = oil/water partition coefficient
h
C,
C
= thickness of the stagnant layer
= concentration of drug in the stagnant layer
= concentration of drug in the bulk solvent
Of interest to this research is the effect of the shape of the tablet on A, and
therefore on dc/dt. Tablets of the 7.5% HPMC formulation were compressed in
three differing shapes to investigate these effects. Several tablets were made in the
caplet shape that has been used up to this point, several wafers were made using a
slugging die with large tablet faces, and finally, several conventionally shaped round
tablets were produced. Dissolution testing was performed on two tablets of each
shape. Samples were taken with replacement and analyzed using UV
spectrophotometry as previously described. Table 1.8 shows the relative size and
surface areas of the three tablets.
Table 1.8: Size and Surface Area of Tablets Differing in Shape.
Shape
Length
Width
Height
Est. Surface Area
Tablet
14mm
14mm
5mm
528mm2
Caplet
19mm
11mm
5mm
589mm2
Wafer
20mm
20mm
3mm
817mm2
49
Figure 1.14 shows the comparative dissolution profiles of drug from the three
different dosage form shapes. The caplet and conventional tablet shape showed very
little difference in the dissolution rate. This is expected since they have very similar
surface areas. However, the wafer shape showed significantly faster release between 4
and 9 hours. This is not unexpected as the wafer has a much larger surface area. By
the 12 hour dissolution sample, the release profiles from the three shapes have
rejoined each other. Release of acetan-iinophen is essentially complete from all three
shapes by the 12 hour dissolution sample.
50
Figure 1.14: Effect of Tablet Shape on the Dissolution of Acetaminophen
Sustained Release Formulations
100
90
80
70
-ci
6O
5o
---caplct
-4- tablet
20
1-- wafer
10
0
2
4
6
8
10
12
Time (h)
14
76
18
22
24
51
Investigations into Dosage Form Division:
Related to the above investigations, it is common in the realm of clinical
pharmacy for a patient to divide tablets if they feel that the tablets are too difficult to
swallow or if a smaller dose is desired. Dissolution was performed on 7.5% HPMC
tablets. Two flasks contained whole tablets, two flasks contained 2 tablets that had
been divided in half, and two flasks contained only 1/2 tablet each. Samples were
taken with replacement and analyzed using UV spectrophotometry as previously
described.
Figure 1.15 shows the dissolution profiles of each type of division. The figure
is scaled to percent of total drug release to adjust for the difference in dose between
the flasks that contained whole tablets and those that contained only half tablets.
There is no significant difference in the release of the whole tablets, the divided
tablets, or the half tablets once the profiles are scaled for dose. This suggests that the
tablets could be divided in half without significant effect on the overall release of
acetaminophen from the tablets.
52
Figure 1.15: Effect of Dosage Form Division on the Dissolution of
Acetaininophen Sustained Release Formulations
I
90
80
70
V
140
(3
-4--WHOLE CAPLET
---HALF CAPLET
20
-è-2 CAPLET HALVES
10
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
53
Clinically, this would allow dosage reductions to be made in the elderly or in
children without sacrificing the controlled release character of the product.
Investigations into Granulation methods:
The final area of these investigations into tablet formulation involved
granulation methods. Acetaminophen is a very fluffy powder that does not flow well,
and the formulation needed to be granulated to increase flowability. Three different
granulation techniques were investigated.
Slugging Method
The 7.5% formulation powder was loaded into a slugging die and compressed
with 10,000 pounds for 30 seconds. The slugging die was 20mm in diameter and
produced round wafers. The resulting wafers were mechanically broken into granules
and sieved. Granules that passed through a 14 mesh sieve but were retained on a 20
mesh sieve were used. The granules were weighed and compressed into caplets using
the Carver press.
Wet Granulation Method
The APAP, HPMC, and PVP were mixed with 1 ml water per tablet. The
resulting paste was forced through a 10 mesh screen to form granules and allowed to
dry overnight at room temperature. The particles were further mechanically broken
and sieved. Those granules that passed through a 14 mesh sieve but were retained on
a 20 mesh sieve were used. Magnesium Stearate 1% was added to the granules prior
to compression. The granules were weighed and compressed into caplets using the
Carver press.
54
Extrusion Method
PVP was weighed and dissolved in I ml water per tablet The APAP and the
T{PMC were weighed and dry mixed in a separate beaker. The PVP solution was
slowly added to the APAP/HPMC powder to form a stiff paste. The paste was
loaded into a 60 ml plastic syringe and "noodles" of the formulation were extruded
onto plastic wrap. The noodles were allowed to dry at room temperature overnight.
After drying, the noodles were mechanically broken into granules and sieved for size.
Granules that passed through a 14 mesh sieve, but were retained on a 20 mesh sieve
were used. Magnesium stearate 1% was added to the granules prior to compression.
The granules were weighed and compressed into caplets using the Carver press.
Dissolution was performed on two tablets from each formulation and the
profiles were compared to profiles previously obtained for the caplets made from
powder. Comparative profiles are show in Figure 1.16. Several subjective measures
were also used to evaluate the granulations methods. Those measures included
percent yield of granules in the 14-20 mesh range, preparation time, and expected ease
of scale up. Investigator's preference was also a factor in the selection of the final
method.
55
Figure 1.16: Effect of Granulation Method on the Dissolution of
Acetaminophen Sustained Release Formulations
100
90
80
70
-c,
a-,
60
50
-4-WET GRANULATION
-U-EXTRUSION METHOD
20
-*- SLUGGED GRANULES
10
-*-- FREE POWDER
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
56
Table 1.9: Percent Yield of Granules in the 14-20 Mesh Range for Three
Granulation Methods.
Method
Total Wt (g)
Wt of 14-20 mesh
% particle
particles (g)
yield
Slugging
7.515
4.014
53.4
Wet Granulation
7.516
2.654
35.3
Extrusion
7.515
4.681
62.3
Table 1.10: Time of Granule Preparation for Three Granulation Methods.
Method
Making
granules
Slugging
6 hours
Wet Granulation
2
hours
24
Extrusion
2
hours
Drying time
Sizing
granules
Total
time
None
3 hours
9 hours
hours
5 hours
7
hours
24 hours
3 hours
5
hours
Ease of scale up was calculated as follows. Each method was rated
1,2,
or,
3
for both time of preparation and percent granules in the correct size. A rating of 1
was given to the fastest method and the method with the highest yield of granules in
the correct size. Likewise a rating of 3 was given to the most time consuming method
and the method with the lowest yield of granules in the correct size. The two
numbers were multiplied together to yield a subjective scale-up parameter.
57
Table 1.11: Ease of Scale Up for Three Granulation Methods.
Method
Yield Rating
Time Rating
Scale-up
parameter
Slugging
2
3
6
Wet Granulation
3
2
6
Extrusion
1
1
1
The slugging method produces a drug dissolution profile which was most
similar to previous results from the direct compaction of the powder mixture. The
traditional wet granulation method product was the most dissimilar. The extrusion
method was selected for future granulations because of its expected ease of scale-up
and relatively desirable drug dissolution profile. The slugging method was not used
because of its long preparation time. The wet granulation method was not used both
because of its dissimilarity to the desired release profile and due to the poor yield of
properly sized granules from the batch. During the mechanical breaking down of the
granules, particles did not neatly break into smaller granules. The granules were very
hard and had a tendency to pulverize into powder yielding particles too small to use.
It should also be noted that some attempts were made to dry the wet granulations in
the vacuum oven rather than at room temperature. The vacuum introduces air into
the formulation and does not produce granules but rather a fluffy mass that greatly
resembles cooked meringue.
58
CONCLUSIONS
From investigations described in this chapter, two formulations were selected
for further testing. The 5% H1'MC formulation released 100% of the 650mg dose of
acetaminophen by the 9 hour dissolution sample. This has complete release in the 12
hour dosing interval but does not provide controlled release of drug over 12 hours.
The 7.5% HPMC formulation provides controlled release over the entire 12 hour
dosing interval. However, only 90% of the dose is released in the 12 hour interval. It
is expected that future testing in healthy human subjects will show one formulation to
behave better in vivo than the other. Any further speculation at this point would be
inappropriate.
59
REFERENCES
1.
Hossain, M.; Ayres, J.W. J. Pharm S 1992, 81(5), pp.444-448.
2.
Van Tyle, W.K., in "Handbook of Nonprescription Drugs. 9th Edition",
American Pharmaceutical Association, Washington, D.C.,1990, pp.70-71.
3.
Insel, P.A., in "Goodman and Gilman's: The Pharmacological Basis of
Therapeutics. 8th Edition," Pergamon Press, mc, Ehnsford, NY, 1990, pp.656659.
4.
Dipiro, J.T., in "Pharmacotherapy: A Pathophysiologic Approach", Elsevier
Science Publishing Co. New York, NY, 1989, pp.646-648.
5.
Abrarnowicz, M. ed. The Medical Letter: On Drugs and Therapeutics. June 21, 1996,
38(977), pp.55-56.
6.
Loeb, S., in "Physician's Drug Handbook. 5th Edition," Springhouse Co.
Springhouse, PA, 1993, pp.2-3.
7.
Drug Information Fulltext (DIF): Acetaminophen Monograph, Computer
Software. Silver Platter FT 1.11,
1995.
8.
Peterson, R.G.; Rumack, B.H. Pediatrics 1978, 62, 877-879.
9.
Wilson, J.T.; Brown, ltD.; Bocchini, J.A.,Jr.; Kearns, G.L. Ther. Drug Monit.
1985, 7, 2-11.
10.
Walson, P.D.; Galletta, G.; Braden, N.J.; Alexander, L. C/in. Pharmcol. Ther. 1989,
46, 9-17.
11.
Insel, P.A., in "Goodman and Gilman's: The Pharmacological Basis of
Therapeutics. 8thEdition,fl Pergamon Press, Inc. Elmsford, NY, 1990, p. 1655.
12.
Prescott, L.F. Br. J. C/in. Pharmac. 1980, 10, 291S-298S.
13.
Winter, M.E., in "Basic Clinical Pharmacokinetics. Second Edition," Applied
Therapeutics, Inc. Vancouver, WA, 1988, pp.7-99.
14.
Shargel, L.; Yu, A.B.C.,in :Applied Biopharmaceutics and Pharmacokinetics,
Third Edition," Appleton and Lange, Norwalk, CN, 1993, pp.170-175.
60
15.
Shargel, L.; Yu, A.B.C.,in:"Applied l3iopharmaceutics and Pharmacokinetics,
Third Edition," Appleton and Lange, Norwalk, CN, 1993, pp.353-357.
16.
Radebaugh, G.W.; Murtha, J.L.; Glinecke, R. United States Patent No.
4,820,522: "Oral Sustained Release Acetaminophen Formulation and Process,"
Mcneilab, Inc., Spring House, PA, 1989.
17.
Dighe, S.V.; Williams, RL., in:"Guidance Oral Extended (Controlled) Release
Dosage Forms In I/'in Bioequivalence and In Vit7v Dissolution Testing." Food
and Drug Administration, Division of Bioequivalence, Office of Generic Drugs,
Rockville, MD, 1993. pp. 1-13.
18.
in "The Merck Index, Eleventh Edition" p.8
19.
Ebube, N.K.; Hikal, A.H.; Wyandt, G.M.; Beer, D.C.; Miller, L.G.;Jones, A.B.,
Phar. Dev. Tech. 1997, 2(2), pp.161-170.
20.
Shargel, L.; Yu, A.B.C.,in :Applied Biopharmaceutics and Pharmacokinetics,
Third Edition," Appleton and Lange, Norwalk, CN, 1993, p. 138.
61
CHAPTER 2:
FORMULATION OF A SUSTAINED RELEASE
ACETAMINOPHEN PRODUCT: DETERMINATION OF
BIOPHARMACEUTIC AND PHARMACOKINETIC PROPERTIES
62
ABSTRACT
Pharmacokinetic studies were conducted in 10 healthy human subjects who
were given four acetaminophen formulations. The four formulations included two
commercially available products (Tylenol Extra Strength® tablets and Tylenol
Extended Relief® tablets) as reference formulations and two sustained release
acetaminophen formulations containing 5% or 7.5% hydroxypropylmethylcellulose
(HPMC). Subjects ranged in age from 22-54 years of age. Three males and seven
females participated in the study. Trial format was a single dose, four way crossover
trial with 6 day washout periods between doses. Subjects provided 10 saliva samples
during each 24 hours dosing period. Acetaminophen concentrations were measured
using HPLC analysis.
Kinetic profiles were generated for each formulation in each subject using
WinNonlin® kinetic simulation software. Tylenol Extra Strength® data were
compared to hand calculations and to literature values to validate the fitting process.
Both Tylenol Extra Strength® and Tylenol Extended Relief® tablets were fitted to 1
and 2 compartment open models with first order input and first order elimination, by
weighing the data points equally or by l/y. Both products were best described by a 1compartment open model with equally weighted data points, first order input, and
first order elimination.
Each new sustained release acetaminophen product was fitted with
four kinetics models. Each fitting assumed equally weighted data points and first
63
order elimination of the drug. Profiles were fitted to 1 and 2 compartment models
with first order input and 1 and 2 compartment models with zero-order input from 0
to Tmax
hours. Tmax
was defined as the time associated with the highest
measured acetaminophen concentration for that subject. Both the 5% and the 7.5%
HPMC formulations were best described by a 1-compartment open model with
equally weighted data points, first order input, and first order elimination.
The 5% HPMC sustained release acetaminophen formulation was selected for
further study based on five target formulation criteria. Target selection criteria
included acceptable tablet size, shape and palatability, estimated steady state plasma
concentration of 5mg/L, convenient dosing interval, total daily dose, and sustained
release character.
64
INTRODUCTION
Based on the formulation data in Chapter 1, two sustained release
acetaminophen formulations were selected for study in human subjects. The
formulations containing 5% or 7.5% hydroxypropylmethylcellulose (HPMC) showed
most promising in vitro dissolution profiles. The dissolution profile of the 5%
formulation showed complete release of the drug in the target 12 hour period, but the
overly rapid release is complete in about 7 hours. The dissolution profile of the 7.5%
formulation showed slow continuous release over a 12 hour period but incomplete
drug release of only ninety percent. Each formulation shows one of the two desired
characteristics during in vitro testing. The
in t
performance of the two formulations
is unknown. Despite the best formulation efforts, no model exists that accurately
predicts in
tüv
behavior of a HPMC matrix tablet formulation from in utiv data for
acetaminophen or any other drug. So, once all known in vitro data have been
collected, in viz trials must be performed to develop the fmal in vitro/in
tim
correlation
that can be used to refine the product formulation and to select a formulation for
further study.
65
TABLET PREPARATION AND TESTING
Tylenol Extra Strength® and Tylenol Extended Relief® tablets were
purchased at a local retail outlet and were dispensed without alteration as baseline or
reference formulations. Sustained release acetarninophen tablets with 5% or 7.5%
HPMC were made using the formulation techniques described in Chapter 1 with
minor scale-up modifications.
Sufficient materials were prepared to make 50 tablets of each sustained release
formulation. As previously described, the polyvinylpyrrolidone K-30 NF/USP (PVP,
Spectrum Chemical Mfg. Corp., Gardena, CA, Lot KD186) was mixed with imI of
distilled, de-ionized water per tablet (5Omls) until completely hydrated. The HPMC
(Methocel® K100M PREM CR, Dow Chemical Co., Midland, MI, Lot
MM92101105K) and acetarninophen NF/USP (Spectrum Chemical Mfg. Corp.,
Gardena, CA, Lot JE321) were dry mixed in a separate container. The PVP solution
was then added to the HPMC/acetarninophen mixture and mixed to form a stiff
paste. The mixture was loaded into 6Oml luer lock syringes and extruded into thin
noodles onto a surface covered with plastic wrap and allowed to dry at room
temperature for a minimum of twenty-four hours. The extruded noodles were
mechanically broken and sieved to size. Granules that passed through a 14 mesh
screen but were retained on a 60 mesh screen were used for tableting. One percent
(w/w) magnesium stearate NF/USP (Spectrum Chemical Mfg. Corp., Gardena, CA,
Lot KC502) was added to the granules and mixed thoroughly to coat all granules.
66
The granules were loaded into a single punch tableting machine (Chemical and
Pharmaceutical Industry Co., New York, NY, Model TPK-12) for compression.
Resulting tablets displayed convex sides and were 14mm in diameter with a 4mm belly
band (See Figure 2.1). The tablets had a target fill weight of 730mg or 750mg for the
5% and the 7.5% tablets respectively. In contrast to previously produced tablets,
tablets made in the tableting machine were round not caplet shaped. As previously
shown, the shape does not significantly effect the release of acetaminophen from the
tablets.
Figure 2.1: Size and Shape of Tablets from Single Punch Tableting Machine.
Cl
IZMM[
]4
MM]6
MM
67
Tablet Testing:
1. Tablet Hardness
Tablet hardness was measured for each manufactured lot of sustained release
acetaminophen tablets. To test the hardness, a tablet is placed between two anvils on
a Strong-Cobb tester. The plunger of the tester is pumped to add increasing amounts
of hydraulic pressure. Once the tablet fractures, the force reading is obtained from
the hydraulic gauge. The force reading is converted into kilograms by dividing the
reading by a conversion factor of 1.6. Acceptable values must be 4 kilograms of
greater1.
2. Tablet Friability:
Tablet friability was also measured for each manufactured lot of sustained
release acetaminophen tablets. Tablet friability is measured by placing a pre-weighed
tablet sample (5 tablets) inside a Roche Friabilator. The friabilator is then operated
for a set number of revolutions. During operation, the friabilator rotates at 25 rpm
and drops the tablet sample 6 inches with each revolution. After 100 revolutions, the
sample is removed, dusted, and re-weighed. Tablet friability (f) is calculated using the
following formula1.
f= lOOx
Where
(1-
(W0/W))
f
tablet friability
Wo = original weight of the tablet sample
W = weight of the tablet sample after 100
revolutions in the friabilator
68
Acceptable values of f should be less than one. Tablet lots that exhibit capping
during friability testing should be discarded regardless of the calculated f value.
3.
Tablet Weight Variation:
Weight variation of the tablets was tested using
a USP
weight variation
test. During this test, 20 tablets are weighed individually, an average weight calculated,
and the individual weights are compared to the average. Tablets have met acceptable
weight variation if no more than 2 tablets are outside of the percentage limit and no
tablets differ by more than 2 times the percentage limit. The percentage limit
depends on the average weight of the tablet.
In
this case, the average weight of the
tablets is greater then 324mg, therefore the maximum percentage difference allowed is
5% (see Table 2.1)1.
Table 2.1: Weight Variation Tolerances for Uncoated Tablets'.
Average Weight of
Maximum Percentage
Tablets (mg)________ Difference Allowed
130
of less
10
130-324
More then
7.5
324
5
4. Tablet Dissolution:
Dissolution testing was performed on 6 tablets of each lot. USP dissolution
paddle method II was used as previously described in Chapter 1. Dissolution was
considered to be equivalent to previous tests if the percentage of drug released from
the tablet at time t was within 5% of previously measured value at all sample times.
69
5. Tablet Test Results:
Forty-seven usable tablets were obtained from compression of the
acetaminophen 5% FllMC granules and were designated Lot #4. Average weight of
5% tablets was 729±O.3mg. Tablet hardness was measured to be 5.75kg and the
friability was measured to be 0.36%. All tests were within acceptable parameters.
Dissolution tests yielded results that were consistent with previous findings.
Forty-one usable tablets were obtained from compression of the
acetaminophen 7.5% I-IPMC granules and were designated Lot #5. Four tablets were
lost due to capping of the tablets. Average weight of 7.5% tablets was 750±0.15mg.
Tablet hardness was measured to be 7.45kg and the friability was measured to be
0.12%. All tests were within acceptable parameters. Dissolution tests yielded results
that were consistent with previous findings.
SUBJECT RECRUITMENT AND CLINICAL TRIALS
Permission was obtained from the Oregon State University Protection of
Human Subjects Committee to conduct limited trials of the new acetaminophen
formulations in healthy human subjects. A copy of the application may be found in
Appendix 2A. For comparison, Tylenol Extra Strength® and Tylenol Extended
Relief® tablets were also administered to human subjects. The study was a four way
crossover test of four formulations of acetaminophen. Subjects were not blinded to
the formulation identity. The study involved 1 trial day per week for 4 weeks
separated by 6 days without acetaminophen as a washout period.
Volunteers for in vivo trials of the different acetaminophen formulations were
drawn primarily from Oregon State University students and staff. After informed
consent was obtained, each individual was supplied with a dose (two tablets) of a
single formulation of acetaminophen. The tablets were either Tylenol Extra
Strength®, Tylenol Extended Relief®, sustained release acetaminophen 5% HPMC,
or sustained release acetaminophen 7.5% HPMC. Subjects were asked to fast
overnight prior to taking the provided formulation, to avoid any acetaminophen
containing preparations for 7 days prior to the first trial day and during all washout
periods, and to continue to fast 2 hours after the dose was taken to standardize gastric
emptying of the tablets.
During the trial, 12 saliva samples were collected from each subject for each
formulation. For each saliva sample, subjects were asked to refrain from eating or
71
drinking for 5 minutes prior to the sample, to chew a 1 inch square of Paraflim® for
1 minute to stimulate salivation, and to collect a sample in the marked tubes provided.
A baseline sample was taken just prior to administration of the dose. Additional
samples were taken 30 mins,, 1 hr, 1.5 hr, 2.0 hr, 3.0 hr, 4.0 hr, 5.0 hr, 6.0 hr, 9.0 hr,
12.0 hr, and 24 hours after the dose was given for a total of 12 samples. Samples were
collected in 4ml plastic sample tubes and frozen at 4°C soon after collection.
Saliva Analysis:
Each saliva sample was frozen for 24 hours, thawed for 2 hours, and
centrifuged at 14,000 rpm for 20 minutes to remove proteinaceous material from the
sample. The supernatint was decanted and refrozen for at least 24 hours. The
samples were thawed and centrifuged a second time to remove additional protein
before analysis. Samples were analyzed using High Pressure Liquid Chromatography
(HPLC).
Standard solutions of acetaminophen were prepared at concentrations of 0.6,
1.0, 2.0, 4.0, 6.0, 8.0, 10.0, and l6.0tg/m1 in distilled, deionized water. For each
sample l5Otl of either the sample supernatant or acetaminophen standard was added
to a 350I micro-centrifuge tube. A lSOp.l aliquot of 7-3-hydroxyethyl-theophylline
40p.g/ml was added to each sample tube as an internal standard and the sample
vortexed for 30 seconds to ensure complete mixing.
Samples were injected onto the HPLC system using an automatic sampler
(WISP 712; Waters Assoc.). The injection volume was set at 20p.l. Separation of
72
components was obtained using a C18-Reverse Phase Column. The mobile phase of
30% methanol/70% distilled de-ionized water was de-gassed and delivered at
0.8ml/min (M-6000A Solvent Delivery System; Waters Assoc.) and absorbance
monitoring was performed at 254nm (Model 440 Absorbance Detector; Waters
Assoc., AUFS=0.1). Retention times for the internal standard and acetaminophen
were 7 and 12 minutes respectively. Sample run time was 18 minutes and the chart
speed was set at 10cm/hr.
For each sample, a minimum of three peaks appeared. The first was identified
as a peak that contained proteinaceous endogenous compounds that remained after
extraction. The second peak was the internal standard peak and the third peak was
the acetaminophen peak. A fourth commonly seen peak appeared at 16 minutes and
was determined to have the same retention time as caffeine. The peak heights of all
acetaminophen and internal standard peaks were measured. Dividing the
acetaminophen peak height by the height of the internal standard peak normalized
each acetaminophen peak. A standard curve was obtained by performing linear
regression on the plot of normalized peak height ratios versus acetaminophen
concentration. The equation obtained from linear regression was used to convert
normalized peak ratios of sample unknowns into acetaminophen concentrations.
Standard curves were prepared daily with each set of samples. Figure 2.2 shows a
typical HPLC profile.
73
Figure 2.2: HPLC Saliva Profile for Subject taking Acetaminophen
Formulation.
ACETAMINOPHEN
74
Subject Data:
Subjects ranged in age from 22-54 years of age. Three males and seven
females participated in the study. The subjects ranged in height from 59 to 75 inches.
Table 2.2 is a summary of the subject characteristics.
Table 2.2: Summary of Subject Characteristics Includmg Age, Height, Weight,
and Gender.
Subject #
Age (yr)
Height
Sex
(in)
Weight
(kg)
1
25
65
M
59
2
37
75
M
107
3
28
64
F
77
4
29
66
F
57
5
54
67
M
85
6
26
62
F
50
7
25
59
F
59
8
20
67
F
61
9
37
64
F
73
10
22
61
F
100
AVERAGE
30.3
65
3M/7F
72.8
Each of the ten subjects was randomly assigned to one of four treatments.
Each treatment period lasted one day with a six day acetaminophen free period
between treatments. At the end of treatment one, subjects were randomly assigned to
one of the three remaining treatments. This pattern was repeated until all ten subjects
had completed all four treatments. Table 2.3 shows the assignment of treatments for
each of the ten subjects.
75
Table 2.3: Random Treatment Assignments for the 10 Subjects
Subject #
Treatment
Period 1
Treatment
Period 2
Treatment
Period 3
Treatment
Period 4
1
SR 7.5
SR 5.0
ER
JR
2
SR 7.5
SR 5.0
ER
JR
3
SR 7.5
JR
SR 5.0
ER
4
SR 7.5
JR
SR 5.0
ER
5
SR 7.5
SR 5.0
ER
JR
6
JR
ER
SR 5.0
SR 7.5
7
ER
SR 5.0
JR
SR 7.5
8
IR
SR 5.0
SR 7.5
ER
9
ER
JR
SR 7.5
SR 5.0
10
JR
ER
SR 7.5
SR 5.0
Where
ER
= 2 x 650mg Tylenol Extended Relief
JR
= 2 x 500mg Tylenol Extra Strength®
SR 5.0 = 2 x 650mg Sustained Release 5.0% HPMC
SR 7.5 = 2 x 650mg Sustained Release 7.5% HPMC
Saliva samples were analyzed as previously described and the data collected.
Each pharmacokinetic profile for each subject was evaluated using WinNonlin® and
the data recorded.
76
PHARMACOKINETIC MODEL FITTING
WinNonlin Kinetic Fitting:
All data were fit using one of four compiled models supplied with the
program.
Figure 2.3: Model #4: 1 compartment first order input, lag time, and first order
elimination.
KID
CçI) = D*KO1/(V)(KO1K1O) * (EXP (K1O*T[) EXP (KO1*T)
Estimated Parameters:
1. Volume/F
2. KOl = absorption rate
3. KI 0 = elimination rate
4.LT =lagtime
Constants in input:
1. # doses
2. dose I (mg)
3. time of dose 1
Secondary Parameters:
1. AUG = D/(V)(K10)
2. KOl half-life
3. K10 half-life
4. Tmax = time of maximum concentration
= ln(K01/K10)/(KO1-K1O)
5. Cmax = maximum concentration
= Cçrmax)
77
Figure 2.4: Model #12: 2 compartment first order input, micro-constants as
primary parameters, lag time, and first order elimination.
C(f) = A*EXP(-ALPHA*TI) + B*EXP(BETA*TI) + C*EXP(KO1*
Where ALPHA and BETA are roots of the quadratic equation:
r*r + (K12+K21+K1O)*r + K21*K1O = 0
Estimated Parameters:
1. Volume/F
2. KOl = absorption rate
3. Ki 0 = elimination rate
4. K12 = transfer rate, 1 to 2
5. K21 = transfer rate, 2 to I
6.LT
lagtime
Constants in input:
I. # doses
2. dose I (mg)
3. time of dose 1
Secondary parameters:
1. AUG D/(V)(K10)
2. K10 half-life
3. KOl half-life
7. BETA half-life
8. A
9. B
10. Tmax*
4. ALPHA
5. BETA
11. Gmaf
6. ALPHA half-life
*Eslimated for the compliled (internal) library only.
78
Figure 2.5: Model #2: 1 compartment IV-infusion (zero order input), no lag
time, first order elimination.
CONSTANT
1(10
C(1)
= (D/T1)/(V)(K1O) * (EXP(-K1O*TSTAR) - EXP(K1O*TI))
where TI
TSTAR
= time of infusion
= T-TI for T>TI
= 0 for T<TI
Estimated parameters:
1.V
2. K10
Volume
= elimination rate
Constants in input:
1. # doses
2. dose 1 (mg)
3. start time of infusion
4. end time of infusion
Secondary Parameters:
1.AUC =D/(V)(K1O)
2. K10 half-life
3.Cmax =C(fl)
4.CL
5. AUMC
6. MRT
7. Vss
79
Figure 2.6: Model #10: 2 Compartment IV-Infusion (zero-order input),
macroconstants as primary parameters, no lag time, first order elimination.
JiL
CONSTANT I
1 1(10
11(21
1(121
2
C(T)
= A1 (EXP(ALPHA* - EXP(ALPHA*TSTAR))
+ B1 (EXP(-BETA *J) - EXP(BETA*TSTAR))
where TJ
TSTAR
= time of infusion
= T-TI for T>TI
= 0 forT TI
A1
B1
= (D/(TI*V)) * ((K21ALPHA)/((ALPHABETA)*ALPHA))
= (D/çn*v)) *
Estimated Parameters:
1. Volume
2. K21
3. ALPHA
4. BETA
Constants in input:
1. # doses
2. dose 1 (mg)
3. start time of infusion
4. end time of infusion
((K21BETA)/((ALPHABETA)*BETA))
80
Secondary Parameters:
1. K10
2. K12
3. Ki 0 half-life
4. AUG
5. ALPHA half-life
6. BETA half-life
7. A*
8.B*
9. Gmax
10. GI
11. AUMC
12. MRT
13.Vss
*A and B are the zero time intercepts following IV injection.
81
TYLENOL EXTRA STRENGTH
This formulation was included in the experiment as a baseline formulation.
As the pharmacokinetics of immediate release acetaminophen have been extensively
studied, this formulation serves as a double check that the study design and analysis
yield data that are reasonably consistent with results obtained by other scientists.
Measured concentration versus time data for the ten subjects taking the
Tylenol Extra Strength Product are listed in Appendix 2B. Saliva concentrations
from the ten subjects were averaged for each time point and analyzed as an overall
"average" profile for the immediate release formulation. Also, data from each subject
were first fitted with equal weight on each point using both 1-compartment and 2-
compartment open models with first order input and first order elimination. The
fitted data were examined for appropriateness and goodness of fit and the
compartmental model that fitted the majority of individual subjects was selected for
additional study. Special consideration was given to the pharmacokinetic fitting of the
"average" curves, which will be used for overall comparison among products because
it is expected to represent the average pharmacokinetic behavior of the general
population. A compartmental model was selected using the Schwartz Criteria, visual
inspection of the data, and using an F-test.
Approximate hand calculations were also performed for AUC, K, and t172 on
the average data to verify fitting appropriateness. AUC was calculated using the
trapezoidal rule. K was determined using linear regression of the elimination portion
82
of the data curve. The t72 and Vd were calculated using standard pharmacokinetic
formulas. Both Tmax and Cmax were estimated by visual inspection of the graphed
data. These hand calculated values were compared to the computer generated profiles
for both the one and two compartment models.
The computer generated parameters were also compared with literature
values. A general literature search provided a fairly comprehensive list of
pharmacokinetic parameters for acetaminophen. As it is been widely shown that
acetaminophen exhibits linear kinetics at therapeutic dosage ranges, some literature
values were scaled to a 1000mg dose to provide an easier basis for comparison.
Once a compartment model was selected, data were fitted again weighting
the data l/y. The two models were compared using both visual inspection and an Ftest to select the best model. Table 2.4 is a summary of pharmacokinetic parameters
obtained from fitting a one compartment open model with equal weight on all points,
first order input, and first order elimination. Pharmacokinetic parameters obtained
from each fitting include area under the curve (AUG in mgTh/L), time of maximum
concentration çI'max in h), the maximum concentration value (Gmax in mg/L), the
quotient of the apparent volume of distribution (Vd in L) over the fraction of the
dose absorbed (F), the lag lit-ne (Tlag in h), the calculated elimination half-life (ti/2 in
h), and the Schwartz Griteria (SG).
Notes about Pharmacokinetic Data
1.
Vd/F acetaminophen is an extremely well absorbed drug. The drug has
continuous absorption throughout the gastrointestinal tract2. It is therefore expected
83
that the value of F will be very close to one and the Vd/F quotient may be treated as
Vd.
2.
AUG Values should be closely examined as in several individual subjects, the
fitted lines predicted by the models do not return to zero. Erroneous K1O values may
result for these models in these individual subjects. Since AUG is primarily calculated
by this program using the equation D/Vd/K1O, AUG values may be affected. This is
especially true in the case of the Tylenol Extra Strength® and Tylenol Extended
Relief® products. In some individual subjects taking these formulations, the data
return to zero but the fitted lines do not, therefore data from these individual subject
was not used. In the 5% and 7,5% HPMC sustained release products this
phenomenon is of less concern. The fact that the lines predicted by the model does
not return to zero may be an indication that input from the dosage form is still
occurring as the product passes though the gastrointestinal tract.
3.
t112
- calculated by 1n2/K1O. As mentioned above, several fitted models
predict lines with plasma concentrations that do not return to zero. Erroneous K1O
values may result for these models. Profiles exhibiting this condition are marked with
an asterisk (*) and are not included in the average calculations.
84
Table 2.4: Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extra Strength Data with a 1-compartment open model with equally
weighted data points, first order input, and first order elimination.
SUBJ #
AUC
Tmax
Cmax
Vd/F
K10
t11
Units
mgTh/L
H
mg/L
L
1/h
h
1
41.00
1.03
14.96
19.75
0.825
0.84
15.83
2
46.45
0.66
12.30
32.63
0.330
2.10
11.18
3
63.68
1.12
6.81
63.88
0.122
5.64
23.08
4
36.76
1.11
10.03
35.25
0.533
1.30
9.12
5
45.38
1.20
5.02
85.07
0.129
5.35
9.33
6
46.23
0.39
14.47
29.91
0.362
1.91
31.58
7
54.85
0.62
16.09
24.71
0.387
1.79
19.41
8
44.61
0.57
7.51
53.41
0.380
1.82
9.08
9
85.15
1.08
15.54
24.95
0.235
2.94
43.30
10
48.64
0.80
10.99
36.17
0.285
2.43
16.75
AV.
52.82
0.80
10.87
35.42
0.330
2.10
9.50
51.27
0.85
11.37
40.57
0.358
1.93*
SC
DATA
AV. OF
10 SUB
* value calculated using harmonic mean.
= in 2/average K10
This model does an excellent job of fitting most of the subject data. The
three worst fitting examples are for subjects three (SC23.08), six (SC31.58), and
nine (SC43.30). For all three subjects, the fitted model predicts a line that falls
below both the peak value (Cmax) and the elimination curve (Kb). The three best
fitting examples are subjects four (SC9.12), five (SC9.33), and eight (5C9.08).
Figure 2.7 is the graph of the average data for this model, and the fit is quite good.
85
Figure 2.7: Graph of Tylenol Extra Strength Average Data fitted with a 1compartment open model with equally weighted data points, first order input,
and first order elimination.
12
.
___________________
OBSERVED
10
+
I'
I
I
'i
- - PRED1D
%
I
I
I
t
0
ci)
U
0
U
I
'
\ .
10
12
Time (h)
14
16
18
20
22
24
86
Table 2.5: Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extra Strength Data with a 2-compartment open model with equally
weighted data points, first order input, and first order elimination.
SUBJ#
AUC
Tmax
Cmax
Vd/F
K10
t11
Units
mgTh/L
H
mg/L
L
1/h
h
1
34.64
1.02
15.03
20.25
0.714
0.97
18.05
2
46.91
0.66
12.32
2.62
0.331
2.09
45.86
3
95.76
0.90
7.57
31.07
0.168
4.12
6.45
4*
68.08
0.82
11.42
37.15
0.198
3.50
1.75
5*
65.34
0.25
7.75
58.87
0.008
80.7
1.85
6
65.82
0.29
17.08
23.68
0.320
2.16
2.03
7*
64.73
0.53
16.44
25.03
0.309
2.24
18.72
8
31.53
0.70
7.79
26.63
0.597
1.16
3.87
9
133.3
0.53
16.38
27.08
0.138
5.00
12.10
10
80.26
0.42
14.52
30.10
0.207
3.34
3.23
AV.
51.76
0.84
11.08
29.60
0.326
2.12
-5.77
69.74
0.64
12.95
23.06
0.353
1.96**
SC
DATA
AV. OF
7 SUB
* profile fitted with a line that does not converge to zero. AUC, t112, and other
pharmacokinetic parameters are not reasonable values and represent mathematical
artifacts. These data are therefore not included in the analysis of in the average of 10
subjects data.
** value calculated using harmonic mean.
= in 2/average K10
Subjects 4, 5, and 7 were not included in the average of 10 subjects data as
described above. Although the equations generated for these data are an excellent fit
to the experimental data points, the profiles generated are tangent to, not convergent
87
with a zero saliva concentration. This suggests that the drug stays in the body
indefinitely which is not consistent with physical data for an immediate release
formulation. Overall, this model appears to fit the data better than the 1
compartment model because of an overall better fit to the elimination portion of the
curve. However, only 7 of the ten profiles yield reasonable data. Figure 2.8 shows
fitted data for the average data for this model, and the fit is better then for a onecompartment model (compare to Figure 2.7).
Figure 2.8: Graph of Tylenol Extra Strength Average Data fitted with a 2compartment open model with equally weighted data points, first order input,
and first order elimination.
12
#1
OBSERVED
10
I
I
I
it________ __
I
I
t
I
I
---PREDICTED
I
&)
f
4
2
.
0
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
88
Comparison of Fitted Parameters to Hand Cakulated Parameters:
As a double check of the fitting program, parameter estimates were calculated
by hand stripping and compared to fitted data from the program. The average data
curve was selected as a representative profile. Linear regression was performed on
the 4, 5, 6, 9, and 12 hour time points to estimate k. AUC was estimated using the
trapezoidal rule. Values of Vd and
t172=1n2/k01
t112
were calculated using Vd=D/(AUC)(kej)and
respectively. Tmax and Cmax were obtained by visual inspection of the
graphed data.
Table 2.6 Comparison of Computer Fitted Parameters to Hand Calculated
Parameters
Fitting Method AUC
Tmax
Vd/F
K10
t112
L
1/h
H
Units
mgTh/
L
H
Cmax
mg/L
Computer
52.82
0.80
10.87
35.42
0.330
2.10
Computer
2 Comp
Hand Calculated
51.76
0.84
11.08
29.60
0.326
2.12
50.71
1.0
11.04
46.75
0.211
3.28
Computer generated parameters of averaged data for both the one
compartment and the two compartment models were very close to the handcalculated parameters. The larger values of Vd/F and
ti!2
for the hand calculated
parameters may be the result of excluding the 24 hour time point from the linear
regression process. This may have resulted in an under estimation of k and a
corresponding over estimation of Vd/F and ti!2. Overall, the similarity of the values
supports the computer simulations and lends confidence to the program output.
89
Model Selection:
Table 2.7: Comparison of Fitted Pharmacokinetic Parameters to Literature
Values
S/
AUC
Tmax
Cmax
tl/2
Kel
Ka
B
3C
6
B
52
S
64.6
0.67
20.6
S
58.6
1.42
15.8
B
33.3
5
47
S
60.5
16
1.97
1.24
15.5
1.92
0.361
9.757
22.5
3.39
0.454
15.2
B
0.5-1
11.4
1.8
0.385
B
0.7
13.2
1.8
0.376
3.25
9'
B
0.9
9.71
1.8
0.390
2.20
10
S
58.85
1.22
20.8
2.47
0.295
S
58.81
0.97
18.10
2.21
0.314
12'
S
63.0
2.67
0.259
13
5
64.3
0.82
21.0
2.60
0.267
i0
S
52.82
0.8
10.87
2.10
0.329
3.20
110
5
51.76
0.84
11.08
2.12
0.326
2.33
Mean
± SD
55.47
0.96
0.344
7.60
±0.26
16.78
±4.21
2.26
±8.89
±0.52
±0.06
±6.06
Range
33.364.6
0.51.42
9.7122.5
1.8-3.39
0.2590.454
2.2015.2
11k
a. Values adjusted to l000mg. Original data for 450mg3.
b. Values adjusted to l000mg. Original data for 500mg. Fasted subjects4.
c. Values adjusted to i000mg. Original data for 500mg. Fed
subjects4.
d. Values adjusted to 1000mg. Original data for 12mg/kg. Assume 70kg person
840mg.5
e. Values adjusted to 1000mg. Original data for 1500mg. Fitted with 1 compartment
model with first order input and first order elimination6.
90
f. Values adjusted to 1000mg. Original data for 1500mg. Fitted with 2 compartment
model with first order input and first order elimination6.
g. Values adjusted to 1000mg. Original data for 10mg/kg. Assume 70kg person
70kg. data in children age 1.7-6 years7.
h. Values adjusted to 1000mg. Original data for 10mg/kg. Assume 70kg person =
70kg. data in children age 2-7 years8.
i. Values adjusted to 1000mg. Original data for 10mg/kg. Assume 70kg person =
70kg. data in children age 2-11 years9.
j. Multiple dose pharrnacokinetic parameters10.
k. Multiple dose pharmacokinetic
parameters11.
I. Non-compartmental analysis. Multiple dose pharmacokinetic parameters12.
m. Compartmental analysis. Multiple dose pharmacokinetic parameters12.
n. From average data fitted with 1 compartment model with first order input and first
order elimination
o. From average data fitted with 2 compartment model with first order input and first
order elimination
* Average of literature values ± SD
Table 2.7 clearly shows that both the one compartment and the two
compartment fitted models provide parameters that are close to the average and well
within the ranges of previously reported literature values for acetaminophen.
Likewise, the literature data are relatively equally divided in use of one and two
compartment models. Despite the better Schwartz Criteria for the two compartment
model, the two compartment model failed to predict reasonable model parameters
for 3 of the 10 fitted kinetic profiles. Therefore, this author has selected the 1
compartment model for additional analysis.
91
Another interesting item is to note that the literature is also split on its use of
saliva and serum data. Those studies using saliva samples arrived at pharmacokinetic
parameters that were similar to the parameters obtained from studies using serum
samples. Since saliva samples may be collected using a non-invasive sampling
technique and appear to yield similar pharmacokinetic results, it is appropriate to use
them for testing of acetaminophen products.
Since one of the main sources of error in the one compartment model above
was underestimation of data points in the elimination curve, it was decided to fit the
data again weighing the points by a factor of l/y and to consider weighting of
1/y2.
This change in weighing scheme increases the significance of the elimination points in
the fitting process, sometimes resulting in a better estimation of the elimination
portion of the curve. Table 2.8 summarizes the pharmacokinetic parameters resulting
from fitting the data points with a 1-compartmental open model with the data points
weighed l/y, first order input, and first order elimination. Figure 2.9 is the graph of
the fitted data for the average data with first order input, first order elimination, and
data points weighed lly.
92
Table 2.8: Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extra Strength data with a 1-compartment open model with the data
points weighed 1/y,flrst order input, and first order elimination.
SUBJ#
AUC
Tmax
Cmax
lid/F
K
t1,2
Units
Mg*h/L
h
mg/L
L
1/h
h
1
30.74
1.00
15.11
20.59
0.796
0.87
-8.14
2
45.45
0.69
12.33
31.92
0.344
2.01
0.63
3
76.46
1.21
6.27
71.2
0.091
7.55
22.39
4
27.49
1.13
9.72
36.94
0.495
1.40
-10.20
5
24.68
0.74
6.84
55.88
0.362
1.91
0.65
6
52.11
0.42
12.53
35.50
0.270
2.56
26.88
7
55.50
0.62
15.74
25.41
0.355
1.95
-5.97
8
23.50
0.54
7.33
55.12
0.387
1.79
4.35
9
97.04
1.16
14.44
27.91
0.184
3.75
36.41
10
54.67
0.46
10.74
42.23
0.216
3.20
14.70
AV.
44.91
0.81
10.45
37.52
0.297
2.33
13.56
48.76
0.79
11.10
40.27
0.350
1.98*
DATA
AV.
OF 10
SUB
value calculated using harmonic mean.
= in 2/average K10
SC
93
Figure 2.9: Graph of Tylenol Extra Strength Average Data fitted with a 1compartment open model with data points weighted 1/y, first order input, and
first order elimination.
12
.
10
___________________
4
,'
I'
OBSERVED
I________
- - - PREDICTED
I
I
I
I
b.0
0
L)
0
L)
rJ)
.
\
'
.
\
10
12
Time (h)
14
16
18
20
22
24
94
Weighing the data points by l/y during the fitting process appears to have
improved the fit on some of the subject data. The cost of the improved fit during the
elimination portion of the curve is the fit around the peak area and the Cmax values.
Most of the fitted models using the i/y weighing scheme underestimate the Cmax
values. Table 2.9 compares the measured Cmax with the Cmax values estimated by
the 1-compartment open models with the data points weighed 1 and l/y.
Table 2.9: Comparison of Estimated Cmax values for the Tylenol Extra
Strength data fitted with 1-compartment open models with different data
points weighing schemes.
SUBJ #
Exp.
Cmax
Est. Cmax
W1
Exp.-Est.
Cmax for
W1
Est.
Cmax
W1/y
Exp.-Est.
Cmax for
W1/y
1
15.22
14.96
0.26
15.11
0.11
2
12.21
12.30
-0.09
12.33
-0.12
3
7.61
6.81
0.80
6.27
1.34
4
10.61
10.03
0.58
9.72
0.89
5
7.35
5.02
2.33
6.84
0.51
6
15.88
14.47
1.41
12.53
3.35
7
16.45
16.09
0.36
15.74
0.71
8
7.55
7.51
0.04
7.33
0.22
9
16.66
15.54
1.12
14.44
2.22
10
11.59
10.99
0.60
10.74
0.85
AV.
11.04
10.87
0.17
10.45
0.59
DATA
95
The models with data points weighed by l/y underestimated the Cmax value
by an average of 1.025mg/L but, models with the data points weighed by 1
underestimated the Cmax by only O.741mg/L.
Finally, the fit for the average data was compared for the two models. Both
modeling schemes appear to fit the data reasonable well upon visual inspection,
however the model with equally weighted data points has a slightly better fit
(SC9.50) than the model with data points weighted l/y (SC= 13.56). Any further
analysis on these data will be done using a one-compartment open model with equally
weighed data points, first order input and first order elimination.
Since the iiy weighting scheme did not significantly improve the fit of the
model, fitting with 1 /y2 was not performed. The 1 /y2 weighting scheme, while
expected to put even more emphasis on the elimination portion of the curve, would
further exacerbate the poor fit of the model around the peak. This weighting scheme
was therefore not applied to the data..
96
TYLENOL EXTENDED RELIEF
The Tylenol Extended ReieI
product is expected to differ from the Tylenol
Extra Strength Product® because of the manufacturer claims of "extended relief'.
Each tablet is composed of 325mg of immediate release acetaminophen and 325mg
of acetaminophen in a sustaining hydrophilic matrix. The analysis process described
above in the Tylenol Extra Strength section was repeated for the Tylenol Extended
Relief product. The raw acetaminophen saliva data are available in Appendix 2B.
Figure 2.10 shows the Tylenol Extended Relief Product fitted with a one
compartment open model with first order input and first order elimination. All data
points are given equal weight during the fitting.
97
Table 2.10: Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extended Relief Data with a 1-compartment open model with equally
weighted data points, first order input, and first order elimination.
SUBJ#
AUC
Tmax
Cmax
Vd/F
K10
t
Units
Mg*h/L
h
mg/L
L
1/h
h
1
48.59
1.19
14.46
41.50
0.322
2.15
29.39
2
79.33
1.58
12.39
37.37
0.152
4.56
24.73
3
25.62
0.82
8.72
57.45
0.444
1.56
13.28
4
81.06
1.67
12.69
39.75
0.202
3.43
41.38
5
45.50
0.73
9.22
59.01
0.242
2.86
31.46
6
67.58
1.70
12.10
32.29
0.298
2.32
25.46
7
74.89
1.41
15.61
30.65
0.284
2.44
31.67
8
76.64
0.96
16.02
31.22
0.271
2.55
51.38
9
84.69
0.79
14.84
41.17
0.186
3.71
21.58
10
39.15
0.40
12.05
48.00
0.346
2.00
9.53
AV.
67.32
1.34
12.15
37.54
0.302
2.29
6.28
62.30
1.12
12.81
41.84
0.274
2.52*
DATA
AV.
OF 10
SUBJ.
* value calculated using harmonic mean.
x = in 2/average K10
SC
98
Figure 2.10: Graph of Tylenol Extended Relief Average Data fitted with a 1compartment open model with equally weighted data points, first order input,
and first order elimination.
14
OBSERVED
12
It
fi
1
I
10
I
- PREDICTED
I'
I
______________
I
4
k
4
2
0
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
99
Many of the data profiles could not be fit for a 2 compartment model. Table
2.11 lists the fitted parameters for those profiles that the computer was able to fit. All
data points received equal weight during the fitting.
Table 2,11: Summary of pharmacokinetic parameters resulting from fitting
Tylenol Extended Relief Data with a 2-compartment open model with equally
weighted data points, first order input, and first order elimination.
SUBJ#
AUC
Tmax
Cmax
Vd/F
K10
t112
Units
mg*h/L
h
mg/L
L
1/h
h
2
79.99
1.58
12.39
37.27
0.218
3.17
27.13
4
136.3
1.54
16.62
20.16
0.236
2.93
4.55
5
53.26
0.60
10.79
46.09
0.265
2.61
3.90
7*
336.5
1.58
15.70
15.87
0.121
5.69
22.35
8*
119.5
0.95
16.05
31.04
0.175
3.95
25.88
AV.
73.29
1.33
12.28
35.32
0.251
2.76
-2.90
89.85
1.24
13.26
34.50
0.239
2.90**
SC
DATA
AV.
OF 3
SUBJ.___
* profile fitted with a line that does not converge to zero. AUC, t, and other
pharmacokinetic parameters are not reasonable values and represent mathematical
artifacts. These data are therefore not included in the analysis of in the average of 10
subjects data.
** value calculated using harmonic mean.
= ln 2/average K10
100
Figure 2.11: Graph of Tylenol Extended Relief Average Data fitted with a 2compartment open model with equally weighted data points, first order input,
and first order elimination.
14
.
12
OBSERVED
,
4'
I'
14
- - - PREDICTED
I________________
10
13
I
I-
4
\
2
I
0
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
101
Of the five profiles that the computer was able to fit as a two compartment
model, two fitted curves are tangential to, not convergent with a zero concentration
profile. Those profiles did not provide reasonable estimates for some parameters
(AUC) and were excluded from the average of three subjects portion of the data.
Since this model could describe such a small number of profiles, it was discarded as
unsuitable for this formulation.
Again, the profiles were re-fit using a one compartment open model with first
order input and first order elimination with the data points weighted 1/y in an effort
to produce curves that better describe the elimination portion of the pharmacokinetic
curve. Table 2.12 describes the data from this fitting model.
102
Table 2.12: Swnmary of pharmacokinetic parameters resulting from fitting
Tylenol Extended Relief data with a 1-compartment open model with the data
points weighed l/y, first order input, and first order elimination.
Vd/F
K10
t112
h
max
mg/L
L
1/h
H
34.36
1.55
11.55
20.65
0.924
0.75
13.04
2
79.33
1.58
12.39
37.37
0.219
3.16
24.73
3
28.25
0.67
8.52
60.28
0.382
1.81
-17.76
4
67.03
1.70
10.49
48.08
0.202
3.43
33.17
5
36.14
0.65
10.13
50.82
0.355
1.95
6.76
6
66.73
1.71
11.98
32.43
0.301
2.30
16.95
7
123.2
1.55
10.44
53.36
0.098
7.01
44.12
8
94.28
1.23
10.79
50.89
0.353
1.96
42.73
9
76.08
1.04
14.67
38.52
0.222
3.12
-9.27
10
42.17
1.17
11.18
50.08
0.308
2.25
-30.65
AV.
60.61
1.22
13.07
38.02
0.282
2.45
19.93
64.82
1.28
11.21
44.24
0.336
2.06*
SUBJ#
Tmax
Units
AUC
Mg*h/L
1
DATA
AV.
OF 10
SUBJ___
* value calculated using harmonic mean.
= in 2/average K10
SC
103
Figure 2.12: Graph of Tylenol Extended Relief Average Data fitted with a 1compartment open model with data points weighted l/y, first order input, and
first order elimination.
14
OBSERVED
12
I'
---PREDICrED
1
I'
10
b.0
4
+
Jo
4
\
I
,._
0
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
104
When comparing the profile of the data fitted with equal and l/y weight on
the data points, little difference is seen in the tabulated data, but as before, the l/y
weighted data have lower predicted peaks and a more gently sloping elimination
phase. Howevet when looking at the average data results for both fitting methods, it
becomes clear that the equally weighted data (SC6.28) fits better than the l/y
weighted data (SC= 19.93). As with the Tylenol Extra Strength Data, it is felt that the
one compartment open model with first order input, first order elimination, and
equally weighted data points best describes the data.
Since this product is 325mg of immediate release combined with 325mg of
"extended release" formulation it was difficult to know what to expect of the release
profile. It would be reasonable to expect a rapid increase in drug concentration
followed by a well sustained or extended, relatively "flat", drug concentration vs. time
profile. These two profiles would combine to form an overall profile that could be
best described by a multiple input model. In reality, it appears that a one
compartment open model with first order input can easily and accurately describe the
combined release of the two elements. Rather than being unique, results for the
Tylenol Extended Reliei) are nearly identical to results for the Tylenol Extra
Strength® tablets after scaling for the difference in the dose (see Figure 2.13).
The nearly identical pharmacokinetic results for the Tylenol Extra Strength®
and the Tylenol Extended Relief® products suggests that the "Extended Relief'
product behaves as an immediate release product, not as a sustained release product.
The 325mg hydrophilic matrix portion of the Tylenol Extended Relief® product is
not successful in extending the release of the acetaminophen from the product. The
increase in the recommended dosing interval from 4-6 hours (Tylenol Extra
Strength®) to every 8 hours (Tylenol Extended Relief)) appears to be possible not
because of any sustained release character of the formulation, but because of the
increase in the dose. Even the 2 hour extension between doses is suspect since the
drug concentration at 6 hours from
1000mg of the immediate release product is higher than the drug concentration at the
8 hours from the larger dose, extended relief product.
Data provided in United States Patent 4,820,522 compares average plasma
acetaminophen levels for a 1000mg dose of "Non-sustained Release Acetaminophen
500mg tablets in 12 subjects" to a 1300mg dose of "Sustained Release (SR)
Acetaminophen Bi-layered 650mg tablets". Figure 2.13a shows a plot of the data
published for that comparison. Figure 2.13b shows that same plot comparison after
the immediate release (IR) data points were proportionally adjusted to a 1300mg dose.
At 8 hours, the difference between the plasma concentrations is 2.6.ig/ml and
2.3j.g/ml respectively for the SR and adjusted JR products. Calculating the time it
would take the Tylenol Extended relief product to decline from 2.6 to 2.3p.g/mI can
been accomplished using the equation C
t,
C0
Coet. C is the drug concentration at time
is the original drug concentration, k is the elimination rate constant, and t is the
time in hours it takes for
C0
to decline to C. First, a k for the Tylenol extended relief
product must be calculated using known data points. Published data shows a plasma
concentration of 2.6pg/ml, 8 hours after the dose and a plasma concentration of
106
1.6j.tg/ml, 10 hours after the dose.
Plugging in the equation we have:
1.6 = 2.6e2
from which k can be determined to be
0.2427h1
Using this calculated k, we can now
solve for the time for the plasma concentration to decrease from 2.6tg/ml to
2.3j.tg/ml.
1.3
=
2.6e(02427)t
This equation yields a value for t of 0.50 hours or 30 minutes. This means that the
acetaminophen release is only extended by only 30 minutes. In light of this, this
investigator considers the term "Extended Relief" to be a misnomer as patients could
achieve essentially the same plasma acetaminophen levels by taking 1300mg of generic
immediate release product rather than pay for the poorly formulated and expensive
brand name Tylenol Extended Relief
product.
107
Figure 2.13: a. Published Average Plasma Concentrations for a 1000mg dose of
Non-sustained Release Acetaminophen 500mg tablets compared to Average
Plasma Levels for a 1300mg dose of Sustained Release Acetaminophen Bilayered 650mg tablets in twelve Subjects.
b. Data in a. after proportionally adjusting immediate release data to
a total acetaminophen dose of 1300mg.
18
16
4-- 1300MG TYLENOL EXTENDED RELEIF
14
--1000MG TYLENOL EXTRA STENGTH
12
0
10
6
4
2
0
0
2
4
6
8
10
12
Time (h)
18
16
--1300MG TYLENOL EXTENDED
RELIEF
14
UTYLENOL EXTRA STRENGTH
12
SCALED TO 1300MG
Rio
8
6
dl
0
2
4
6
Time (h)
8
10
12
108
5% HPMC SUSTAINED RELEASE PRODUCT
Release of acetaminophen from matrix tablets is expected to be a
combination of kinetic release profiles. Initially, the profile is expected to show a
small burst of drug release. This small burst is the result of drug being released from
the surface of the tablet during initial wetting of the tablet surface. As the surface
begins to hydrate, diffusion of drug out of the wetted and gelled tablet is expected to
be the dominant kinetic factor. Lastly, drug release from surface erosion of the tablet
will be added to the profile as the tablet is forced through the gastrointestinal tract via
peristaltic contractions of the small and large intestines. The three kinetic profiles are
expected to combine to form a kinetic profile that has a lower and broader peak than
was seen in the immediate release Tylenol Extra Strength® and the Tylenol Extended
Relief profiles. The lower peak is expected to gradually decline back to baseline
resulting in a much smaller apparent k and therefore a longer apparent t1/2 value.
The actual magnitude and proportion of the three kinetic patterns, and therefore the
sum, will determine the overall release profile.
Since the exact release pattern from the sustained release products was
unknown and unpredictable, fitting was attempted to a larger number of
pharmacokinetic models in terms of drug input. Data from each subject were fitted
to four models. All models were open models with equally weighted data points and
first order elimination. Models used included: a one compartment model with first
109
order input, a one compartment model with zero order input from time zero to
Tmax, a two compartment model with first order input, and a two compartment
model with zero order input from time zero to Tmax. Tables 2.13-2.16 display results
of fitting the four models. Figures 2.14-2.17 are graphs of average data for each of
the four models.
Table 2.13: Summary of pharmacokinetic parameters resulting from fitting 5%
HPMC Sustained Release Acetaminophen with a 1-compartment open model
with equally weighted data points, first order input, and first order elimination.
SUBJ#
AUC
Tmax
Cmax
Vd/F
K10
t112
Units
Mg*h/L
h
mg/L
L
1/h
h
1
89.83
3.21
5.63
91.15
0.079
8.73
12.41
2
66.73
3.55
6.86
52.74
0.184
3.75
33.58
3
86.44
3.56
4.61
120.3
0.062
11.1
20.74
4
65.26
3.96
10.5
36.76
0.271
2.55
37.10
5
27.94
2.84
4.69
51.03
0.456
1.52
27.06
6
95.90
2.15
6.89
80.42
0.084
8.22
22.20
7
63.57
3.87
6.42
37.14
0.276
2.51
19.93
8
34.63
3.68
3.96
60.06
0.313
2.21
26.72
9
132.0
4.41
4.83
110.3
0.044
15.5
0.905
10
49.16
2.97
5.64
66.72
0.198
3.49
16.99
AV.
69.18
3.73
5.62
60.84
0.133
5.2
13.50
71.14
3.42
6.00
70.66
0.196
35*
DATA
AV.
OF 10
SUBJ___
value calculated using harmonic mean.
= In 2/average K10
SC
110
Figure 2.14: Graph of 5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 1-compartment open model with equally weighted data
points, first order input, and first order elimination.
7
.
OBSERVED
6
- PREDICTED
( '
I
I
I
5
\
I
I
ii
I
I
b.O
I
I
I.
.'
'
I
I
4
p.4
'1
I
2
I
I
-
0
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
111
Table 2.14: Summaiy of pharmacokinetic parameters resulting from fitting 5%
HPMC Sustained Release Acetaminophen with a 2-compartment open model
with equally weighted data points, first order input, and first order elimination.
The computer was unable to fit many of the profiles using this model.
SUBJ#
AUC
Tmax
Cmax
Vd/F
I(
t112
Units
Mg*h/L
h
mg/L
L
1/h
Ii
4
269.05
4.12
8.91
27.76
0.087
7.96
42.59
6
147.64
2.44
7.24
39.13
0.112
6.16
20.67
8
34.81
3.67
3.96
58.62
0.319
2.17
29.25
AV.
230.21
3.70
5.63
47.22
0.060
11.5
11.65
150.5
3.41
6.70
41.83
0.172
4.02*
DATA
AV.
0F3
SUBJ___
value calculated using harmonic mean.
x = In 2/average K10
SC
112
Figure 2.15: Graph of 5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 2-compartment open model with equally weighted data
points, first order input, and first order elimination. The computer was unable
to fit many of the profiles using this model.
7
OBSERVED
6
- - - PREDICTED
S
I
I
I
5
I
\
I
b.0
0
'
'U
U
03
U
I
I
'.
S
C/D
S
-'
2
-
I-
0
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
113
Table 2.15: Summary of pharmacokinetic parameters resulting from fitting 5%
HPMC Sustained Release Acetaminophen with a 1-compartment open model
with equally weighted data points, zero order input from 0 to Tmaxdata hours,
and first order elimination. Tmax was defined as the time associated with
the highest saliva concentration for each subject.
SUBJ#
AUC
Tmaxa
MRT
Vol.
Cl
t112
Units
Mg*h/L
h
h
L
L/h
h
1
65.11
4
7.10
70.94
9.98
4.92
26.31
2
59.66
4
4.87
53.08
10.89
3.37
24.95
3
73.58
4
12.14
107.24
8.83
8.41
19.78
4
74.71
5.083
4.81
41.90
8.70
3.33
38.53
5
29.48
3
3.73
82.25
22.04
2.58
16.18
6
66.38
3
6.02
59.00
9.79
4.17
33.17
7
55.40
4
4.74
55.61
11.73
3.28
-1.00
8
30.37
5
3.47
74.34
21.40
2.40
12.73
9
124.7
3.083
21.17
110.39
5.21
14.6
15.73
10
47.01
3
5.21
72.05
13.82
3.61
8.36
AV.
59.47
4
6.49
70.96
10.92
4.50
13.03
62.63
3.81
7.32
72.68
12.23
5.06
DATA
AV.
OF 10
SUBJ___
SC
114
Figure 2.16: Graph of 5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 1-compartment open model with equally weighted data
points, zero order input from 0 to Tmax hours, and first order elimination.
Tmax was defined as the time associated with the highest saliva
concentration for each subject.
8
OBSERVED
7
6J
IA
0
I
4)
U
0
U
ci)
2
I
04
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
115
Table 2.16: Summary of pharmacokinetic parameters resulting from fitting 5%
HPMC Sustained Release Acetaminophen with a 2-compartment open model
with equally weighted data points, zero order input from 0 to Tmax hours,
and first order elimination. Tmax. was defined as the time associated with
the highest saliva concentration for each subject. Some profile could not be fit
using this modeL
SUBJ#
AUC
Units
Mg*h/L
1
MRT
Vol.
Cl
t112
h
h
L
L/h
h
105.67
4
16.98
32.26
6.15
3.63
4.74
2
128.08
4
26.13
42.41
5.07
5.79
17.13
3
224.92
4
72.89
73.16
2.88
17.54
17.13
5
22.94
3
1.13
85.48
28.3
2.09
18.07
6
113.77
3
15.62
29.26
5.71
3.55
23.70
7
62.11
4
15.01
55.48
10.4
3.67
1.12
8
28.75
5
2.65
76.57
22.6
2.34
15.05
AV.
86.00
4
13.83
53.81
7.55
4.93
-4.12
98.03
3.85
21.48
56.37
11.6
5.44
Tmaxa
DATA
AV.
OF 8
SUBJ
SC
116
Figure 2.17: Graph of 5% HPMC Sustained Release Acetanunophen Average
Data fitted with a 2-compartment open model with equally weighted data
points, zero order input from 0 to Tmax hours, and first order elimination.
Tmax was defined as the time associated with the highest saliva
concentration for each subject.
OBSERVED
I.'
- PREDICFED
I
/
t
II
0
I
4
\
I
1
4
10
12
Time (h)
14
16
18
20
22
24
117
Discussion of Model fitting for the 5% HPMC Sustained Release Acetaminophen
Formulation:
1 Compartment Models: First Order Input and Zero Order Input:
Both one compartment models fit the data relatively well. Statistically, the
Schwartz Criteria is slightly better for the zero-order input model than for the firstorder input model (13.03 compared to 13.50 respectively). However, the difference is
not significant.
The one area where both 1-compartment models fail is around the peak.
Most of the fitted profiles underestimate the peak concentration by ten percent. One
possible explanation is that the peak concentration values are artificially elevated.
Most subjects began the bioavailibility study between eight and nine am. By the 3-4th
hour into the study most subjects were eating lunch. It has been previously shown
that eating can deplete the saliva production in a subject resulting in artificially
elevated concentrations of drug. It is possible that some if not all of the peak values
may have been affected in this manner. Another possible explanation is that the
input function is complex and cannot accurately be described by a single input
function. While the literature describes multitudes of complex distribution and
elimination functions, relatively less study has been devoted to complex input
functions. It would be interesting to study the contributions of the drug dissolved off
the surface of the tablet, the drug released through diffusion out of the tablet, and the
drug released by erosion of the tablet to the total input process. Molecular
disentaglement theory promises to address these and other issues in HPMC tablets.
118
Another more significant difference between the two input models is the
fitting of the elimination portion of the curve. For most profiles, the model with
zero-order input more closely describes the elimination portion of the curve. The
average curves (shown in figures 2.14 and 2.16) are an exception to that observation,
however it should be noted that the curve predicted for the zero-order input curve
does not appear to return to zero in a reasonable time period. The fact that the
predicted line does not return to zero is not particularly disturbing for a true sustained
release product and may reflect a flaw in the modeling process. During modeling, the
program was instructed to continue zero-order input from time zero to lime Tmaxd
only. If input continued beyond this artificially selected peak time as an apparent slow
first-order process the apparent elimination curve may be deceptive. As the tablet is
retained in the gastrointestinal (Gi) tract until a bowel movement occurs, it is possible
that slow input from the tablet may occur beyond 24 hours. After the tablet is
expelled from the GI tract and input from the tablet ceases, the elimination of drug
from the body would be expected to resemble the elimination curve for the
immediate release product, i.e. rapid elimination and declination to zero. In this case,
there may be insufficient data points in the terminal portion of the elimination curve
to allow the modeling program to perceive the change in apparent slope.
2 Compartment Models: First Order Input and Zero Order Input
As previously seen with the immediate release and the extended release
products, the two compartment models, both zero and first order input, were unable
to fit several of the data sets. In the case of the first-order input model, the computer
119
was able to fit only 3 subjects plus the average data. The zero-order input model
performed slightly better fitting 8 subject profiles plus the average data. In addition,
some sets from both input models that yielded pharmacokinetic parameters that
were not consistent with expectations or hand calculations. Therefore it is assumed
that the relatively simple 2 compartment models tested do not well describe the
release of drug from this dosage form in individual subjects.
Model selection:
Although the zero-order, 2-compartment model fit the average data well,
both of the 2-compartment models failed to fit the individual subject data. They were
therefore discarded as unsuitable. Of the two 1-compartment models, both fit
relatively well. Since neither 1-compartment models fits better than the other, the
simpler of the two models was chosen for further study. The one compartment open
model with first order input and first order elimination will be used to describe the
data for the 5% HPMC sustained release acetaminophen formulation. As discussed
earlier, it is recognized that the input function is not a simple first order function for
this formulation. However, it is concluded that this simple assumption results in
adequate prediction and description of the drug concentration versus time curve for
acetaminophen absorption from the 5% I-IPMC formulation involved.
120
Selection of this model provides the following estimates for pharmacokinetic
parameters for the fit of average data.
Volume/F = 60.84L
KOl
= absorption rate
K1O
LT
AUG
Tmax
Gmax
=
=
=
=
= 1<9 =
O.5292h'
elimination rate
O.1331h1
lag time = O.25h
area under the curse = 69.18jtgh/ml
time to maximum concentration = 3.73h
maximum estimated concentration S.62p.g/ml
Since this dosage form exhibits sustained release character, the possibility that
the rate constant may be interchanged must be investigated. The phenomenon is
termed the flip-flop model and can occur any time that the rate constants are
estimated using oral data.. This phenomenon is possible in this case because the
sustained release character of the tablet may artificially slow the absorption of the
drug resulting in a 1<9 that appears to be smaller than the 1<d This occurs most
commonly with drugs that have a rapid elimination (1<9>K). The only way to be sure
is to compare the orally derived rate constants to intravenously derived rate constants
in the same subjects. This was not possible in this study because acetaminophen is
not available in an intravenous form in the United States. For the remainder of the
analysis it will be assumed that the flip-flop model has occurred since the true t72 for
acetaminophen is reported to be 1-2 hours. The apparent t112 for this formulation
based on the terminal slope of the data is therefore estimated to be 5.2 hours for this
dosage form. The true t
for the drug in this model based on Ka is then is calculated
to be 1.3 hours which is consistent with a flip-flop model effect.
121
7.5% HPMC SUSTAINED RELEASE PRODUCT
Like the 5% HPMC data, the model that would fit the 7.5% data was
unknown. It is expected that these data should exhibit a slower overall release pattern
than the 5% HPMC data because of the higher HPMC content. It has been well
documented in the literature that as the percentage of HPMC in the formulation
increases, drug release from the dosage form decreases. Chapter 1 contains in
vitro
testing demonstrating this concept. Eventually this trend results in incomplete release
of the drug from the dosage form.
In vitro,
the 7.5% HPMC formulation did not
achieve complete release of the acetaininophen from the dosage form in 12 hours.
Its in vit performance is expected to be slightly better. This expectation is based on
the premise that more surface erosion of the matrix will occur in the gastric track
than occurred in the in vitro dissolution. Although the dissolution apparatus
sometimes simulates the tumble of the matrix through the gastric tract, this requires
that tablets remain free-floating within the dissolution chamber. Unfortunately, the
hydrated surface of the tablets often became like a glue, sticking the tablets firmly to
the side of the dissolution flask. This had two basic effects on the dissolution of drug
from the tablet. One, it prevented the tumbling motion of the tablet that might
simulate the motion of the tablet as it passed through the gastrointestinal tract via
peristaltic muscle contractions. Two, the side of the tablet that was attached to the
glass of the dissolution chamber was protected from erosion and changed the overall
surface area of the tablet that was available for diffusion of drug out of the tablet.
122
Note: This concept of changing the release from the tablet matrix by preventing
release from various surfaces of the tablet is a liability in the current study, but has
been successfully used to the advantage of other scientists in the development of the
Geomatrix® system of drug release. In tüv, the sticking of the tablet to the GI
mucosa should not occur, therefore in vivo release from the tablet is expected to be
more rapid and complete than in the in vitrv test.
Data from each subject were fitted to four models. All models were open
models with equally weighted data points and first order elimination. Those models
were a one compartment model with first order input, a one compartment model
with zero order input from time zero to Tmax, a two compartment model with first
order input, and a two compartment model with zero order input from time zero to
Tmax. Tables 2.17-2.20 display results of fitting the four models. Figures 2.18-2.21
display the data and fitted curves for the average data for each of the four models
fitted.
123
Table 2.17: Summary of pharmacokinetic parameters resulting from fitting
7.5% HPMC Sustained Release Acetaminophen with a 1-compartment open
model with equally weighted data points, fIrst order input, and first order
elimination.
SUBJ#
AUC
Tmax
Cmax
Vd/F
K10
t112
Units
MgTh/L
h
mg/L
L
1/h
h
1
17.04
2.73
1.56
292.79
0.130
5.32
-10.96
2
34.52
1.82
3.82
131.06
0.143
4.82
3.72
3
151.2
4.96
1.63
374.67
0.011
60.4
-17.67
4
15.09
4.84
1.92
124.66
0.346
2.00
9.89
5
11.05
1.74
1.88
242.16
0.243
2.85
13.19
6
59.36
4.86
3.51
125.91
0.086
7.97
6.19
7
76.27
3.01
3.21
183.09
0.046
14.9
-18.10
8
60.71
2.49
3.87
149.01
0.071
9.64
0.66
9
35.57
3.61
2.74
159.92
0.114
6.06
17.03
10
59.65
3.62
3.99
115.54
0.094
7.34
19.06
AV.
44.61
3.47
2.58
194.58
0.074
9.25
-14.30
52.04
3.36
2.81
189.88
0.128
5.41*
DATA
AV.OF
10 SUB
* value calculated using harmonic mean.
= in 2/average K10
SC
124
Figure 2.18: Graph of 7.5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 1-compartment open model with equally weighted data
points, first order input, and first order elimination.
OBSERVED
a,, _.
2.5
- - - PREDICTED
b.0
0
I
0.5
10
12
Time (h)
14
16
18
20
22
24
125
Table 2.18: Sunmiary of pharmacokinetic parameters resulting from fitting
7.5% HPMC Sustained Release Acetaminophen with a 2-compartment open
model with equally weighted data points, first order input, and first order
elimination. The computer was unable to fit many of the profiles using this
model.
SUBJ#
AUC
Tmax
Cmax
Vd/F
K10
t
Units
mg*h/L
h
mg/L
L
1/h
H
1
331.48
1.59
2.81
164.81
0.011
58.2
-15.04
2
43.22
1.89
3.94
71.17
0.211
3.28
2.51
5
86.47
1.73
1.89
138.57
0.054
12.7
11.71
10
85.53
3.37
3.81
79.70
0.095
7.27
16.71
AV.
53.53
3.51
2.63
113.00
0.107
6.45
-15.84
115.06
2.14
3.11
113.56
0.092
753*
DATA
AV.
OF 4
SUB
* Value calculated using harmonic mean.
x = in 2/average K10
SC
126
Figure 2.19: Graph of 7.5% HPMC Sustained Release Acetaimnophen Average
Data fitted with a 2-compartment open model with equally weighted data
points, first order input, and first order elimination. The computer was unable
to fit many of the profiles using this modeL
.
2.5
-1
OBSERVED - - - PREDICTED
I
1-
ri
I
p
0
1
t
-
I
0.5
10
12
Time (h)
14
16
18
20
22
24
127
Table 2.19: Summary of phannacokinetic parameters resulting from fitting
7.5% HPMC Sustained Release Acetaminophen with a 1-compartment open
model with equally weighted data points, zero order input from 0 to Tmaxa
hours, and first order elimination. Tmax was defined as the time associated
with the highest saliva concentration for each subject.
SUBJ#
AUC
Tmax
MRT
VoL
Cl
t112
SC
data
Units
mg*h/L
h
h
L
L/h
h
1
14.16
3
5.56
255.38
45.9
3.85
-5.36
2
23.30
3
2.93
81.7
27.9
2.03
23.01
3
82.08
4
40.8
323.39
7.91
28.3
4.16
4
16.84
5.16
6.04
233.20
35.6
4.18
8.67
5
9.62
3
2.63
178.27
67.5
1.83
16.00
6
61.96
4
13.6
142.46
10.5
9.41
-2.20
7
70.50
3
18.3
169.20
9.21
12.7
-0.63
8
66.85
2
16.4
159.89
9.72
11.4
7.76
9
34.64
3
8.96
168.12
18.7
6.21
6.98
10
61.74
4
10.3
108.48
10.5
7.14
24.8
AV.
40.36
3
11.6
187.47
16.1
8.07
-0.32
44.16
3.41
12.5
182.00
24.3
8.71
DATA
AV.
OF 10
SUBJ___
128
Figure 2.20: Graph of 7.5% HPMC Sustained Release Acetaininophen Average
Data fined with a 1-compartment open model with equally weighted data
points, zero order input from 0 to Tmax hours, and first order elimination.
Tmaxa was defined as the time associated with the highest saliva
concentration for each subject.
3.5
A
It
4
I'
3
,
S
t
t
- - - PREDICTED
I
I
.1
2.5
OBSERVED
"
'\
I
b.O
2
*
4
I
Io 1.5
L)
'I
I
ci)
I
-%
i
I
I
I
-%
I
0.5
0
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
129
Table 2.20: Summary of pbarmacokinetic parameters resulting from fitting
7.5% HPMC Sustained Release Acetaminophen with a 2-compartment open
model with equally weighted data points, zero order input from 0 to Tmax
hours, and first order elimination. Tmax was defined as the time associated
with the highest saliva concentration for each subject. Some profiles could not
be fit using this model.
SUBJ#
AUC
Tmaxa MRT
Vol.
Cl
t
units
mg*h/L
h
h
L
L/h
H
1
19.94
3
10.45
116.0
32.58
7.84
-16.3
2
41.19
3
9.67
14.01
15.80
7.81
2.55
5
54.32
3
70.51
85.25
11.96
53.2
11.15
6
67.48
4
15.87
128.9
9.63
11.27
-1.06
9
38.66
3
10.75
47.30
16.80
7.64
7.59
10
93.02
4
21.87
27.23
6.98
16.14
15.78
AV.
49.82
3
16.47
109.7
13.04
11.80
-9.45
52.43
3.33
23.18
69.79
15.62
17.31
DATA
AV.
OF 6
SUBJ___
SC
130
Figure 2.21: Graph of 7.5% HPMC Sustained Release Acetaminophen Average
Data fitted with a 2-compartment open model with equally weighted data
points, zero order input from 0 to Tmax hours, and first order elimination.
was defined as the time associated with the highest saliva
concentration for each subject.
Tmaxa
3.5
I'
I.'
3
OBSERVED
I
,
- - - PREDICTED
'I
I'
I.'
ik
2.5
\
I
0
2
4
1)
U
o i.s
4
U
.
-
I
Cl)
1
-'
0.5
0
0
2
4
6
8
10
12
Time (h)
14
16
18
20
22
24
131
Discussion of Model fitting for the 7.5% I{PMC Sustained Release Acetaminophen
Formulation:
Selection of a model for the 7.5% HPMC sustained release formulation
followed the same criteria and observations as the 5% HPMC sustained release
formulation. As before, both two-compartment models were discarded as unsuitable
because of the inability to fit several individual subject profiles with the model. The
2-compartment model with first order input performed the poorest., fitting only four
subject profiles plus the average curve. The 2-compartment model with zero-order
input performed only slightly better fitting six subject profiles plus the average curve.
The 1-compartment models fit all subject data and the average curves for
both input finctions. The model with first order input still underestimated the peak
in contrast to the zero-order input function that overestimated the peak. Both
profiles describe the data fairly well but the Schwartz Criteria for the first order input
model is significantly better than for the zero-order input model (-14.40 as compared
to -0.32 respectively). The one compartment open model with first order input and
first order elimination will also be used to describe the data for the 7.5% HPMC
sustained release acetaminophen formulation.
Model selection:
Selection of this model provides the following estimates for pharmacokinetic
parameters for averaged data fitted with this model.
132
Volume/F
KOl
K1O
LT
AUG
Tmax
Cmax
194.58m1
absorption rate = Ka = O.75O6O9hl*
O.074867h4*
= elimination rate = K
lag lime = O.06h
area under the curve
44.6lpg h/mi
= time to maximum concentration 3.47h
= maximum estimated concentration = 2.S8g/ml
* See previous discussion of the flip-flop model. Apparent
9.25 hours. Calculated t,'2 for the drug = 0.92 hours.
t72
for this formulation
133
Selection of a Sustained Release Acetaminophen Product for Phase Two
Clinical Trials
Comparison of the in tv bioavailibility of the 5% and the 7.5% HPMC Sustained
Release Acetarninophen Formulations:
By comparing the AUC of the sustained release product to the AUG of an
immediate release product, a relative in vivo estimation of the bioavailibility for the two
sustained release acetaminophen formulations can be made. The Tylenol Extra
Strength® and the Tylenol Extended Reliet® products may be used as reference
formulations.
First, bioavailibility is compared for the two reference formulations. AUG for
the 1000mg dose of immediate release Tylenol Extra Strength Product® was
S2.82.tg/ml (for the data averaged before fitting with a 1-compartment model with
first order input and first order elimination). AUG for the 1300mg dose of the
Tylenol Extended Relief Product® was 67.32p.g/ml (for data averaged before fitting
with a 1-compartment model with first order input and first order elimination).
Assuming that Kel, Vd, and F remain constant, then changes in dose should produce
proportional changes in AUC. Since the same subjects were used to test both
formulations, similar pharmacokinetic parameters should be expected. Differences in
the AUG values should therefore reflect changes in the bioavailibility of the
formulation and not changes in the subject pharmacokinetic parameters.
To compare products, AUG for the Tylenol Extra Strength® product must
be proportionately adjusted for a 1300mg dose. Proportionally, an AUC of
134
68.66p.g/ml would be expected if a 1300mg dose of Tylenol Extra Strength® were
given. This is consistent with the 67.32g/m1 AUG from the Tylenol Extended
Relief® product. From this it can be assumed that an AUC value of approximately
67-ó8.tg/mi represents complete absorption of a 1300mg dose of acetaminophen in
this subject population.
The literature surveyed in Table 2.7 displayed an average AUG of
S5.47±8.89jtg/ml for a 1000mg dose. That average converts to a range of 46.5864.36j.tg/ml. Once adjusted to a 1300mg dose, the average becomes 72.11 pg/rnl with
a range of 6O.SS-83.66p.g/ml. The AUG of the Tylenol Extra Strength® and the
Tylenol Extended Relief® products are well within the range.
In comparison, the fitted values of AUG for the 5% HPMG sustained release
product and the 7.5% HPMG sustained release acetaminophen products are
69.18p.g/ml and 44.ólig h/mi respectively. The AUG for the 5% HPMC falls within
the estimated range suggesting that release of drug from the tablet is essentially
complete. The AUC for the 7.5% HPMC sustained release acetaminophen
formulation is only 44.61 j.tg h/mi suggesting that only 48-74% of the drug is released
from the formulation. This incomplete drug release from the 7.5% HPMC sustained
release formulation does not make this formulation a good candidate for continued
study. Although, true fraction of the dose absorbed values (F) are obtained by
comparing drug absorption in an oral formulation to that in an intravenous dose of
the same drug, relative F values can be obtained by comparing the two HPMC
sustained release formulations to the immediate release formulation known to have a
135
F= 1. Using the average literature AUG value of 72.11 jtg/ml as 100%, relative F
values can be estimated for the 5% HPMC product (F = 0.96) and for the 7.5%
IIPMC product (F1 = 0.61).
Selection of a Sustained Release Acetaminophen based on Target Formulation
Criteria:
Recall that 5 overall target criteria were outlined in chapter one. They were:
1.
Pharmaceutically acceptable size, shape, and palatability.
2.
Sustained release character: zero-order release preferred but
pseudo zero-order release or combination release acceptable.
3.
Minimum plasma concentration at steady state of Sjig/ml.
4.
Overall maximum daily dose of 2.6gm of acetaminophen per day
5.
Convenient dosing interval of once-twice daily
First consider the size and palatability of the tablets. The compressed HPMC
tablets of the 5% and the 7.5% formulations both measure 14mm in diameter and
6mm in height with no perceptible taste. Each dose consists of two tablets. No
difficulties in swallowing the tablets were reported by subjects in this study.
The sustained release character of both HPMC formulations was found to be
a combination release that could be adequately described by a simple one-
compartment open pharmacokinetic model with first order absorption and first order
elimination.
The last three of the development goals are intertwined and depend on
estimates of the behavior of the sustained release acetaminophen formulations upon
136
multiple dosing. The target steady state plasma concentration of 5tg/ml is desired.
Using the in
iit
pharmacokinetic data from the single dose studies, multiple dose
simulations can be performed to evaluate the feasibility of achieving this goal. Since
the model chosen slightly underestimates the concentrations observed at the peak and
during the elimination portion of the curve, multiple dose estimations should also
slightly underestimate steady state concentrations.
The superposition principle was used to predict drug accumulation in plasma
for the sustained release acetaminophen products. Recall that this principle assumes
that early doses of drug do not affect the pharmacokinetics of subsequent drug doses.
It will further assume the desired dosing interval (t) is 12 hours. Overall daily dose
using this dosing regimen is = 1300mg every 12 hours which further complies with
the target goal of total daily acetaminophen dose of less than or equal to 2.6 grams
acetaminophen per day. The C,, is the minimum plasma concentration at steady
state. It can be calculated using the equation
Cssmin = (S)(F)(Dose)
V
Where S
F
V
k
* e'
*
(1-e')
= salt fraction
= fraction of the dose absorbed
Volume of distribution
= elimination rate constant
the dosing interval
S is assumed to be 1 for both formulations, and r is selected to be 12 hours.
Relative F values for 5% and 7.5% HPMC formulations were previously calculated to
be 0.96 and 0.61 respectively.
137
For the 5% HPMC formulation:
= [(1) (0.96) (1300mg) /60.841* [1 /(1_e(°133)(12)]* [e'332j
= (20.51)* (1 .2542)* (0.2027)
= 5.21ig/ml
For the 7.5% HPMC formulation:
= [(1) (0.61) (1300mg) /194.581* [1/(1 _e°°74Z1* [ e°072]
= (4.075)* (1 .6991)*(0.41 14)
= 2.84jtg/mI
While the 5% HPMC formulations meets and slightly exceeds the target
steady state minimum plasma concentration, the 7.5% HPMC formulation falls short
of the goaL Figures 2.22 and 2.23 show simulated multiple dose profiles for the 5%
HPMC and 7.5% HPMC products. Clearly, the incomplete drug release from the
7.5% HPMC sustained release formulation combined with sub-therapeutic estimate of
Css make it a poor candidate for additional study. Conversely, the apparently
complete release of drug from the 5% HPMC sustained release formulation combined
with the favorable estimate of Css make it a logical choice for Phase II clinical trials.
138
Figure 2.22: Simulate Plasma Acetaminophen Concentrations for Multiple
Dosing of the 5% HPMC Sustained Release Acetaminophen formulation.
12
10
ii
I
10
20
30
40
50
Time(h)
60
70
80
90
139
Figure 2.23: Simulate Plasma Acetaminophen Concentrations for Multiple
Dosing of the 73% HPMC Sustained Release Acetaminophen formulation.
5
4.5
4
3.5
0
(I)
1.5
0.5
0
10
20
30
40
50
Time (h)
60
70
80
90
140
CONCLUSIONS
Tylenol Extra Strength® and Tylenol Extended RelieB) produce single dose
in vivo pharmacokinetic profiles that were best described by a one-compartment
open model with equally weighted data points, first order absorption, and first order
elimination. Pharmacokinetic parameters estimated agreed with literature data
reported by other scientists.
Both the 5%and the 7.5% HPMC sustained release acetaminophen
formulations produced in vivo pharmacokinetics that were most consistent with a
one-compartment open model with first order input and first order elimination when
fitting individual subject data. Two-compartment models did not adequately describe
individual subject data and were unsuitable to either formulation. One-compartment
models with zero-order input could be applied to the data but did not provide the
optimum fit.
Comparison of the sustained release formulations to the immediate release
data collected from the literature suggests that the 7.5% HPMC sustained release
acetaminophen formulation released only 48-74% of the total drug from the
formulation. In contrast, the 5% HPMC sustained release acetaminophen product
was found to have released nearly all of the drug contained within the tablet. C was
estimated for both sustained release formulations with ti2 hours. Estimates of C.
for both products yielded a C of 5.59jjg/ml for the 5% formulation and a C of
3.7lp.g/ml for the 7.5% HPMC formulation.
141
Comparing these data to the original target criteria for development of the sustained
release acetaminophen product, the 5% HPMC sustained release acetaminophen
formulation was found to comply with all five target criteria and has been selected to
continue to Phase II clinical trials.
142
REFERENCES
1.
Lachman, L., Lieberman, H., and Kanig, J.: The Theoy and Practice of Industrial
Pharmacy. Lea & Febiger.Philadelphia, PA. 1986. pp. 297-303.
2.
Gilman, A.G., Rail, T.W., Nies, A.S., and Taylor, P., eds: The PharmacolqgicalBasis
of Therapeutics, 8th ed., New York, NY, Macmillan, 1990. pp. 656-659.
3.
Van Bommel, E.M.G., Raghoebar, M., and Tukker, J.J., Biop harm. Drug Dirposit,
12, 355-366 (1991).
4.
Phuapradit, W. and Bolton, S., Drug Dep.
5.
Prescott, L.F., Br. J. C/in. Pharmac. 10, 291S-298S (1980).
6.
Manse!!, L. Ph. D. Thesis, Chapter 3:page 261-262 (1985).
7.
Peterson, R. G. and Rumack, B. H., Pediatrics, 62, 877-879 (1978).
8.
Wilson,J.T., et. aL, Ther. Drug Monit., 4, 147-180 (1982).
9.
Watson, RD., et. al., C/in. PharmacoL Ther., 46, 9-17 (1989).
10.
Hossain, M. and Ayres, J.W.,
11.
Sahajwalla, C.G. and Ayres, J.W., J. Pharm. Sci., 80(9), 855-860 (1991).
12.
Bonn, M.T. and Ayres, J.W., mt. J. Pharm., 54, 199-209 (1989).
mt. J.
& md. Pharm., 17(8), 1097-1107 (1991).
Pharm., 133, 223-235 (1996).
143
CHAPTER 3
FORMULATION OF A SUSTAJNED RELEASE ACETAMINOPHEN
PRODUCT: PHASE II CLINICAL TRIALS
144
ABSTRACT
Phase II clinical trials were conducted to compare a novel sustained release
acetaininophen (SR) formulation to a conventional immediate release (IR)
acetaminophen formulation for treatment of pain due to osteoarthritis in the knee.
Thirty male patients between the ages of 44 and 76 were recruited from the Veterans
Administration (VA) Outpatients clinic in Portland, Oregon. The study was a
randomized, placebo controlled, double blind crossover study. Baseline surveys
were performed on the enrolled patients. A pain and disability question was
administered and the time to walk 50 feet was measured. Saliva samples were also
collected at evaluation periods two and three. Each patient was randomly assigned to
either the SR or JR formulations for the first treatment period. Patients took 2
tablets of study medication 4 times a day for 4 weeks. After 4 weeks, patients
returned for a second evaluation. After a 7 day washout period, patients were then
crossed over to the other formulation for treatment period two. Upon completion of
the second medication period, patients repeated a third final evaluation. Rescue
analgesic tablets (ibuprofen 200mg were provided to patients for use during the
washout period and for pain not relieved by the administered acetaminophen
treatment.
Seventeen patients completed the study. All seventeen were verified as
meeting the minimum compliance standards (missed no more than 10% of total
doses) and rescue analgesic guidelines (no more than 4 tablets/day) during the
145
treatment periods. Saliva acetaminophen concentrations were determined using
standard HPLC techniques. Data from the questionnaires was collated and prepared
for analysis.
Average saliva concentrations were decayed to estimated trough values. The
SR formulation produced an estimated steady state trough concentration of 5.1 lmg?L
and the JR formulation produced a significantly lower level of 1.34mg/L. ANOVA
comparison of the questionnaire results between the JR and SR products showed that
the SR formulation was equally effective as the JR formulation in reducing pain and
improving mobility in patients with osteoarthritis of the knee (a=O.OS). The 2.6
gram/day SR product was equally effective as the 4 gram/day JR product despite the
large difference in dose. Reported side effects were similar for the two formulations
and included drowsiness, headache, nausea, GI upset, and diarrhea.
Subsequent comparison of the SR formulation to the baseline treatment
exhibited more dramatic results. ANOVA evaluations performed on the baseline
treatments and the SR treatments showed statistically significant improvements in the
patients average overall rating of their pain levels, the ability of these patients to stand
without help from another person, and in the duration of pain relief that these
patients received from their treatment medication. Other areas that improved but
were not statistically significant included a decrease in pain after the SR treatment and
an increase in the overall relief that the SR treatment provided to these patients.
Overall, the novel sustained release acetaminophen formulation performed
well. Jt achieved the formulation goal of an estimated minimum steady state
146
acetaminophen goal of 5mg/L. It also reduced the average overall pain rating and
improved the duration of the pain relief in patients compared to the baseline
treatments. Time to walk 50 feet was reduced by 1.65 seconds and patients required
less ass stance in standing while using the SR treatment as compared to the baseline
treatment. These results suggest that the sustained release formulation is equally as
effective as the JR treatment and superior to the baseline treatments in these patients
with osteoarthritis of the knee. These effects occurred while reducing the dose of
acetaminophen to 2.6 grams/day from 4 grams/day. Additional studies with larger
number of patients are needed to verify these results, but initial results are promising.
147
INTRODUCTION
Pharmacodynamic analysis suggests that a plasma acetaminophen
concentration of 5mg/L is necessary to provide analgesic relief to patients1'2. Chapter
I focused on formulation and dissolution studies performed to produce an
acetaminophen product with predetermined in
vitiv
drug release parameters. Chapter
2 involved Phase I clinical trials to establish in zit performance and pharmacokinetic
parameters. Those studies suggested that a new 5% hydroxypropylmethyl-cellulose
(HPMC) sustained release acetaminophen formulation would provide the necessary
in
tivo release to maintain a steady state plasma concentration of 5mg/L with a dose of
l300mg given every 12 hours. This chapter investigates the effectiveness of this
formulation in patients with a chronic pain syndrome. Osteoarthritis patients were
selected as a model disease state.
Osteoarthritis:
Osteoarthritis affects nearly 10% of the population over age 60 and is second
only to cardiovascular disease in causing severe chronic pain and
disability3.
Osteoarthritis occurs when the catabolic functions of chrondrocytes exceed the
anabolic functions. The result is a breakdown of the protective cartilage in the joint
surface. The activated chrondrocytes produce increased amounts of collagenase,
stromelysin, and water, while producing decreased amounts of cartilage matrix,
proteoglycans, chrondrocytes, and bone formation. The resulting anatomic changes
include cartilage erosion, subchondral bone microfractures, bone cysts, thickening of
148
the subchondral bone, osteophytes, and fibrocartilage repair abnormalities4 (see
Figure 3.1).
Figure 3.1: Diagram of physical changes that take place in an osteoarthritic
knee
Osteoarthrltis
Normal
I
Thickened Capsule
Capsule
Cyst Formation
Cartilage
Sclerosis in Bone
Fibrillated Cartilage
Synovium
Osteophytic Upping
Synovial Hypertrophy
ne
Altered Contour
ofBone
Osteoarthritis occurs most commonly in hands, hips, feet, neck, and spine. It
is linked to age, obesity, occupation, and genetic predisposition3'5. Clinically, sufferers
describe loss of function, chronic pain, and increasing disability in the affected joints6.
149
Therapy is therefore aimed at pain relief, increased mobility, and reduction of
disability while minimizing side effects3.
Due to limited time and resources available for the current study, patients with
osteoarthritis of the knees were selected as a target population. Justification of this
choice includes the availability of a published and validated pain/disability
questionnaire for this subtype of the disease, documentation concerning effectiveness
of immediate release acetaminophen in treatment of the disease, quantitative nature of
the walking time measurements, and significant incidence of the disease in the
recruitment population/area.
Study Design:
Investigational Review Board (IRE) applications were approved by the
Human Studies Committees of both Oregon State University and the Portland
branch of the Veterans Administration (VA) Hospital. An Investigational New Drug
Application (IND) was filed with the Federal Food and Drug Administration. Copies
of these documents are found in Appendices 3A, 3B, and 3C respectively. The IRB
board at the VA Hospital expressed concern about acetaminophen toxicity and it's
relationship to hepatic toxicity. The question was addressed by an review of
acetaminophen metabolism and literature concerning acetaminophen induced
hepatotoxicity.
150
History and review of acetaminophen toxicity and alcohol consumption.
Review of Acetaminophen: Structure and Metabolic pathways:
Figure 3.2: Acetaminophen structure and metabolic pathways
ACETAWNOPP
HNOCH,
'>
SULFATE
P44V M1XEOFUNCTON OX.IDAS
so-cocH
PQTtJATW
TQmc
NYERMEDATEB
GLUTATMION
5)
GLUTAThION
o1
T
MACRQMO4.EGULE
t5RCAP1URC
ACU,
Acetaminophen is preferentially conjugated into glucuronide or sulfate and
excreted from the body via renal elimination7'8. Once these pathways are saturated,
the remaining acetaminophen is oxidized by the cytochrome P450 mixed function
oxidases (primarily P450 2E1) to N-acetyl-p-benzoquinoneimine
(NAPQI)9'10.
NAPQI is usually rendered nontoxic by conjugation with glutathione. Once
glutathione stores are exhausted, NAPQI remains in the liver causing hepatic toxicity.
151
In normal patients, approximately 2% of the dose is excreted unchanged in the urine,
95% is conjugated to the sulfate or glucuronide, leaving only 3% of the dose to be
oxidized to NAPQI11. There are several possible causes of glutathione depletion.
The first is chronic depletion over time. The constant drain of the store of
glutathione by chronic administration of acetaminophen (greater than 4 grams/day)
can deplete the glutathione store. A second cause is acute depletion. This occurs
when the amount of acetaminophen taken at a single time exceeds the amount of
glutathione present12. A third cause of glutathione depletion is insufficient dietary
intake. People who do not intake sufficient sources of protein in their diet cannot
produce as much glutathione. Alcoholics are known to possess decreased amounts of
glutathione'3'14. Whether that is a result of poor nutrition or some intrinsic effect of
the ethanol is unclear at this time. Alcoholics are also at increased risk of toxicity
because of the stimulating effect of ethanol on the cytochrome P450 3A system1516.
This system is thought to increase the rate of formation of NAPQI and increase the
risk of hepatic damage.
152
Table 3.1: Literature reports of acetaminophen toxicity and alcohol.
rJ.
U
Z
-
2
..
3
0
U
0
r.4
Emby and
0
Z
n
yrs
g/24h
2
31/F
52/M
3
59/M
Fraser17,
0
U/L
A/C/
10.0
14.0
3,561
13,610
C
C
59
68
16
2
died
died
6,200
1,040
400
C
9.5
67/F
50/W
7.5
5.2
i.2-6.5
mg/dL
s
1977
Barker et.
al.8, 1977
N
1.3
19
12
?
0.6
10
alive
alive
alive
Goldfinger
et.al.24, 1978
1
36/F
9.75
1,960
A
18.6
28.9
alive
McClain et.
al.19, 1980
3
48/M
53/M
43/M
5.0
C
C
C
17.0
8.0
7.0
35
50
16.6
alive
16.5
6,960
9,940
7,720
2.6-3.9
19,710
C
13.0
12
alive
Licht et.
al.20, 1980
1
53/M
LaBrecque
2
36/M
10
died
alive
4.5
3.0
3,300
3,300
C
C
5.9
6.9
....
29/F
....
alive
alive
2
36/F
27/F
6.4
4.0
8,460
4,590
A
C
13.0
8.7
12
21
alive
alive
1
23/F
6.0
4,320
C
10.0
13.1
alive
1
37/F
10.0
14,500
C
8.7
20.0
died
1
41/M
10.0
6,500
C
3.5
6.0
alive
and
Mitros21,
1980
Gerber
etaL22,
1980
Johnson et.
al., 1981
Black et.
al., 1982
Levinson 25,
1983
ETOH key Aacute ingestion, Cchronic ingestion, N=denies ingestion, ?alcohol
ingestion unknown.
153
Table 3.1: Literature reports of acetaminophen toxicity and alcohol (cont.)
z
q
1
7/M
LO
5,178
C
6.4
20.0
alive
1
b5/M
/.0
10.100
C/A
9.6
27.0
alive
Leist et. al.
28,
1985
3
28/M
28/M
40/M
29,700
19,750
2,396
C
C
C
5.1
63
alive
23.9
4.2
27
17
died
alive
Seeffet. al.
6
C
C
C
13.0
24
2.4
16.5
17
21
3.6
0.9
6.6
14
3.6
19,710
10,000
5,640
2,870
26,900
6,888
22
alive
alive
alive
alive
alive
alive
39/M
38/M
5.0
4.4
6,494
13,496
C
C
4.2
21
30
alive
alive
66/M
20.0
6.0
5.0
6.0
5.0
10.0
9,240
3,199
14,920
7,225
3,000
4,052
C
C
C
C
C
C
4.0
2.4
7.4
2.0
7.7
6.0
23
46
15
alive
alive
alive
alive
19
37
died
died
5,759
14,997
C
C
7.2
4.4
Himmelstein
et. aI?, 1984
Fleckenstein27
1985
29,
53/M '.6-3.9
1986
0/M
39/M
58/M
34/F
49/F
Kartsonis et.
aL30, 1986
2
Kumar and
6
65/F
43/F
Rex 31, 1991
55/M
59/M
34/M
Briksson et.
al.13, 1992
2
7.0
6.0
9.0
12.5
3.8
I..0-6.0
....
25/M 5.0-6.0
46/F 3.0-4.0
A
C
C
6.1
...
....
....
....
alive
alive
ETOH key Aacute ingestion, Cchronic ingestion, Ndenies ingestion, ?alcohol
ingestion unknown.
154
Table 3.1: Literature reports of acetaniinophen toxicity and alcohol (cont.)
z
q
Whitcomb
and Block
1
1994
Bonkovsky.2
32,
1
29/F
43/F
40/M
55/F
45/F
29/F
41/F
40/F
47/F
15/F
34/F
5.0-7.0
t.0-6.0
35/M
26/M
51/M
49/M
40/F
27/F
36/F
60/M
67/F
26/F
0-25
10-15
16-24
12-18
12-18
67/M
1.0-3.0
.0
.0-8.0
.0-9.0
p.0-10
.0-6.0
/.0-8.0
L5-5.0
1.0
L0-15
>13
13-16
?
>5.0
10,400
14,520
19,916
6,457
5,727
3,117
30,000
17,585
3,990
9,735
2,060
9,881
7,824
1,318
13,740
10,000
15,720
13,860
2,289
12,740
21,691
....
N
N
C
N
N
C
C
....
....
....
....
....
....
....
....
....
....
alive
alive
alive
alive
alive
....
....
died
....
....
....
....
C
....
....
N
....
....
....
....
....
....
....
....
....
....
alive
alive
alive
alive
alive
alive
alive
alive
....
....
died
....
....
....
....
alive
alive
....
....
died
....
....
....
....
....
....
alive
alive
alive
....
....
alive
N
C
C
A
C
C
C
C
C
C
C
C
N
1995
ETOH key Aacute ingestion, C=chronic ingestion, N=denies ingestion, ?za1cohoI
ingestion unknown.
155
Discussion of literature review on acetaminophen toxicity and alcohol:
Out of the 60 case studies reviewed here only 9 patients (1 5%) showed toxicity
at less than or equal to 4 grams of acetaminophen per day. Eight of the nine patients
were documented alcoholics. There is little evidence that doses of less than or equal
to 4 grams of acetaminophen per day causes toxicity in nonalcoholic patients.
Three other studies not included above are of note in the history of
acetaminophen induced hepatotoxicity. The first is a study done by Rumack et. al. in
1983. They found that administration of 4 grams of acetaminophen daily for 14 days
did not cause elevated hepatic aminotransferase levels or induce hepatic necrosis in a
group of patients with chronic active hepatitis and cirrhosis. This article is extensively
cited and appears in multiple letters to the editors of several journals including
Annuals of Internal Medicine34, Digestive Diseases and Sciences35, and Journal of the
American Medical Association36. The second article is a 1986 look at factors that may
effect mortality in acetaminophen overdose. Read Ct. al's look at 247 patients
concludes that "While there was a trend for the alcoholic patients to deteriorate more
rapidly and to develop higher prothrombin times than the nonalcoholic group, neither
of these differences reached statistical significance (O.2>p>O.lO). Likewise there was
no significant difference in the clinical course or outcome between patients who took
alcohol concomitantly with the paracetamol overdose37." This article is also
extensively cited and appears in the previously mentioned letters to the editors. Lastly,
the 1981 findings of Rumack et. al. in 662 cases of acetaminophen overdose, they
subdivided patients into several groups. These groups consisted of patients with toxic
blood concentrations and patients without toxic blood concentrations. These groups
156
were further divided based on a history of chronic or acute alcohol consumption.
Their findings show that alcohol consumption, both chronic and acute intake had no
significant effect on the maximum prothrombin ratio, maximum serum bilirubin ratio,
or the elevation of the SGOT or SGPT ratio when the acetaminophen blood level was
in the non-toxic range. When the acetaminophen blood level was measured in the
toxic range, statistical differences were seen in maximum prothrombin time and
maximum serum bilirubin ratio between patients who had a history of chronic alcohol
intake and those with no history of chronic alcohol intake38. They also associated
acute alcohol consumption with a hepatic protective effective. A mechanism for this
protective effect is not discussed nor is this effect mentioned in any of the other
papers.
Conclusions concerning acetaminophen and hepatotoxicity:
1. Chronic alcoholics may be at increased risk for developing toxic effects
from acetaminophen when it is taken in doses greater than 4 grams per day. The
mechanism is probably a combination of reduced glutathione production and
cytochrome P450 enzyme induction. Few reports of toxicity occur in patients who are
not alcoholic and consume less than or equal to 4 grams of acetaminophen per day.
2. Few reports of toxicity have occurred in patients taking recommended doses
of the drug (4 grams/day). Of those reports, a majority of those patients were chronic
alcoholics.
Based on those two statements, all efforts will be made to effectively screen
out patients who are at risk of increased toxicity. By eliminating patients with a
documented history of alcohol abuse, the increased risk they may represent is
157
documented history of alcohol abuse, the increased risk they may represent is
eliminated in this study. Recognizing that an accurate history of alcohol consumption
remainder will be evaluated for
may be difficult to obtain from these patients, the
preexisting liver disease using liver enzyme assays performed in the last 6 months,
and patients will be counseled as to the increased risk of side effects and adverse
reactions when alcohol is used in conjunction with any analgesic medication.
Participants will be advised to limit their alcohol intake but will not be resiricted in
their alcohol intake beyond the FDA's recommended two drinks per
day limit
158
The study design was a double blind crossover comparing two treatments of
acetaminophen, each of which were administered as two tablets taken four times a day
for four weeks per treatment. Treatments were separated by a 7 days "washout"
period during which patients did not receive acetaminophen. One treatment consisted
of 1000mg (2x500mg tablets) of an immediate release (IIR) commercially available
product (URL corp. Lot 15448, exp. 7/97). The second treatment consisted of
1 300mg (2x650mg tablets) of the sustained release (SR) product developed as
described in chapter two, alternated with two placebo, identically appearing doses for
a total of four doses per day. The placebo tablets were made to appear identical to the
sustained release tablets. All tablets used in the study were approximately 12mm in
diameter, white in color, and had an imprint of three numbers and three letters.
During the sustained release treatment, doses 1 and 3 contained active medication,
while doses 2 and 4 were the placebo. Total daily dose of acetaminophen for the SR
treatment was 2.6 grams and it was 4.0 grams for the IR treatment.
Table 3.2: Comparison of dose placement in the SR and JR treatment packets.
Treatment
Dose I
Dose 2
Dose 3
Dose 4
Sustained
Release
Drug
Placebo
Drug
Placebo
Immediate
Drug
Drug
Drug
Drug
Release
1000mg
1000mg
1000mg
1000mg
1300mg
1300mg
All medications were pre-packaged into medication cards. The Redi-Pak®
159
medication packaging system (MOCORP INC. Smithtown, NY) consists of clear
plastic bubbles in which each dose of the medication is placed. The card is then
sealed to the backing using a peel and stick mechanism. No heat is involved in the
packaging. After packaging, each card holds 7 x 4
28 doses of medication.
Appropriate labels were placed in the areas that displayed the drug and dosing
regimen. For this study, each card of study medication was also labeled across the top
of the bubbles as Dose 1, Dose 2, Dose 3, and Dose 4. Down the side of the bubbles,
each card was labeled with the days of the week. Packaging was done to increase
compliance with the dosing regimen.
Initial concern was expressed that the Redi-Pak® system might be difficult for
the target population to use. However, patients stated they had no trouble pushing
tablets out of the cards. Several patients even stated that they were easier to use than
standard "child resistant caps". Two patients participating in the study were of
increased concern because they had above the elbow amputations of one arm. During
the first evaluation, these patients pushed tablets out of the cards without problems,
despite their disability.
A rescue analgesic (Advil® brand ibuprofen 200mg tablets lot 95 AG 1019
exp. 4/97) was provided to patients for use during the washout period and for pain
not relieved by acetaminophen treatments. A maximum of 400mg could be taken up
to three times a day. Patients were asked to record any doses of ibuprofen needed in
the provided log. The rescue analgesic was packaged into medication cards that held
160
2 doses of two tablets each. One card of rescue analgesic was included in each
treatment package.
Acetaminophen treatments were also packaged in medication cards that each
held a one weeks supply of medication. Each card held 28 doses of two tablets each.
Groups of four cards of acetaminophen were placed into opaque envelopes with one
card of rescue analgesic according to a randomization list and sealed. Each packet
was labeled with the subject number and the treatment number and was dispensed
without opening. Patients were asked to return all cards once the treatment had been
completed. The coded randomization list was kept confidential from the
recruiter/investigator.
Evaluation of each patient's pain was performed at three intervals throughout
the study. The first evaluation was slightly more extensive than the subsequent
evaluations. During the first evaluation, patients were asked for such demographic
data as age, height, weight, number of joints affected by the osteoarthriiis, length of
time since diagnosis, etc. Patients were also questioned about overall health, allergies,
and other inclusion and exclusion criteria. Once patient eligibility was confirmed,
consent forms were filed and prescriptions written and filled for both the study
treatment and the rescue analgesic. A questionnaire consisting of 12 questions was
administered to patients and time to walk 50 feet measured. The questionnaire was
modified from the Stanford HAQ test39. This test was selected because it had been
previous validated and use on osteoarthritis patients to measure pain and disability°.
Subsequent visits after treatments two and three were identical in nature.
Patients repeated the questionnaire and walking test. Patients were also asked to
161
sjipply a saliva sample for analysis. Saliva samples were immediately frozen for future
analysis. All empty cards of study medication and cards of rescue medication were
collected at the end of each visit. The returned packets remained sealed unlil
completion of the study.
162
SAMPLE SIZE CALCULATION
Literature searches were conducted to locate previous studies that might
contain information that would be useful in estimating the sample size needed for the
study. These studies were examined to provide initial estimates of the type of data
collected, methods of evaluation, and of results and conclusions. Information about
analysis methods, strength, and power of the tests performed on data were also
gathered. Prior to performing a sample size calculation, a study design must be
selected. For this study a randomized double blind 2X2 crossover design was
selected.
Of all the literature examined8, a study by Bradley et al. (1991) was selected
as the study that would provide the most accurate estimates for sample size
calculations. The Bradley study examined 3 different drug treatments and used a
timed walking test and pain questionnaire to evaluate the outcome of drug treatments
in osteoarthritis patients. The study was not a crossover design. This study was
thought to be statistically representative because of it use of acetaminophen in
osteoarthritic patients and because of similar evaluation methods.
Dr. Dave Birkes (Oregon State University, Department of Statistics) was
consulted concerning the sample size calculation. First, a table of Standard
Deviations (SD) of within-subjects differences was calculated from Table 3 of the
Bradley paper.
163
Table 3.3: Estimated standard deviation used for sample size calculation
Acet. 4000
0.74
Ibup. 1200
Ibup. 2400
Average
HAQ pain score
0.82
0.81
50-ft-walk-time
HAQ dis. Score
1.94
0.31
3.71
0.33
0.86
3.32
0.49
2.99
0.38
Then, the magnitude of difference that was desirable to detect was chosen.
Since the purpose was to compare treatments, the magnitude that must be detected
must be at least the mean difference between the treatments.
Table 3.4: Estimated magnitude of difference used for sample size calculation.
Acet. 4000
Ibup. 1200
Ibup. 2400
Average
HAQ pain score
0.33
0.30
0.35
0.33
50-ft-walk-time
0.50
0.50
0.70
0.57
HAQ dis. score
0.08
0.08
0.11
0.09
Next, the means and SD of differences in the proposed study are assumed to
be similar to those listed above. Therefore the sample size needed for a 2X2
crossover design in order to detect the assumed mean differences with 90%
probability would be:
Table 3.5: Estimated sample size for 2x2 crossover design used in study sample
size calculation.
Total sample size n
I-fAQ pain score
50-ft-walk-time
HAQ dis. Score
66
294
186
Lastly, the corresponding powers or probabilities of detection were calculated
for the assumed mean differences.
164
Table 3.6: Estimated powers or probabilities of detection used in sample size
calculation.
HAQ pain score
50-ft-walk-time
HAQ dis. Score
n50
n100
n150
n200
0.81
0.25
0.38
0.98
0.47
0.66
0.99+
0.64
0.99+
0.83
0.76
0.92
A sample size of approximately 50 people was estimated to be appropriate for
the proposed study.
165
PATIENT RECRUITMENT AND ENROLLMENT
Recruitment was performed from the Veterans Administration (VA)
Outpatient clinic in Portland, OR. Medical charts for patients with scheduled
appointments in the general medicine clinic were screened I day prior to the
appointment for study suitability. Charts were reviewed for proper diagnosis
documentation and for inclusion/exclusion criteria.
Inclusion criteria:
1.
Documented diagnosis of osteoarthritis in one or both knees.
2. Age 40-90 inclusive
3.
Permission of Primary Care Provider
Exclusion criteria:
1.
Renal dysfunction elevated BUN or serum creatinine.
2.
Hepatic dysfunction elevated SGOT, SGPT, alkaline phosphatase, or
total serum bilirubin.
3.
Allergy to either acetaminophen or ibuprofen.
4.
Diagnosis of ethanol abuse or consumption of> 3 alcoholic beverages per
day.
5.
Diagnosis of infectious disease HIV, hepatitis B or C, tuberculosis, etc.
6.
Drug interactions phenytoin, carbamazepine, cyclosporine, lithium,
rifampin, chloramphenicol, diflunisal, oral contraceptives, metoclopramide,
or cisapride.
7.
Mental incompetence or diagnosis of dementia.
8.
Trauma to the knees in the last 3 months surgery, acute injury, or intraarticular injections of the joint.
9.
Pregnancy or inability to verify birth control/menopausal status.
10. Inability to walk 50 feet without assistance or assistive devices.
11. Concurrent diagnosis of a disease state that might affect the ability to walk
or might constitute a contra-indication for acetaniinophen or ibuprofen
therapy. Includes, but is not limited to, rheumatoid arthritis, unstable
angina, chronic obstructive pulmonary disease (COPD), congestive heart
failure (CHF), peripheral vascular disease, fibromyalgia, bursitis, active
peptic ulcer disease (within the last 12 months), and chondromalacia.
12. Any documented behavior that might constitute a risk to the investigator
or the patient themselves. Includes, but is not limited to, documented
suicidal ideation, previous attempts to commit suicide, use of illegal or
recreational drugs, and previous history of threatening behavior towards
other medical personnel.
When patients arrived for their appointments, permission of the attending
physician was obtained prior to approaching the patient about enroUment. After the
physician addressed immediate health concerns of the patient, the patient was
approached concerning enrollment into the study. If interested, patients were enrolled.
Patients were counseled to restart their previous analgesic regimens at the conclusion of
the study.
Recruitment lasted for the period between May 20th, 1996 and December
31st, 1997. During that time, a total of 13,483 medical charts of patients scheduled for
visits were screened for possible patient inclusion into the study. A documented
diagnosis of osteoarthritis of the knee was made in 708 patients. This represents
5.25% of the screened patients. Inclusion/Exclusion criteria were then applied to this
population to identify eligible participants.
A total of 349 patients were excluded from the study for failure to meet one or
more inclusion/exclusion criteria. Table 3.1 is a summary of the distribution of those
167
patients. Justification and explanation of each exclusion criteria follows the table.
Table 3.7: Number of Patients Excluded from the Study Categorized by the
Exclusion Criteria
Excluding factor
Level
# patients
Renal Dysfunction
Mild (1.4<Scr<2.0)
Moderate (2.1<Scr<3.0)
Severe (Scr>3.0
33
Alk. Phosphatase> 100
31
SGOT>35
10
Total Bilirubin> 1.0
5
Hepatic Dysfunction
Combined Renal and Hepatic
Dysfunction
Allergy to Drug
Ethanol Abuse
Infectious Disease
Drug Interactions
Mental Status
Recent Trauma to Knees
Birth Control
Assistive Device or Inability to
Walk 50 Feet
Concomitant Diseases
High Risk Patients
Misc. Exclusions
Age
8
4
9
Acetaminophen
Ibuprofen
Greater than 3 Drinks/Day
Hepatitis B
Tuberculosis
Phenytoin
Cyclosporine
Dementia
Mentally Incompetent
Injections or surgery
Unable to verify
Cane or Walker
3
CVA with hemiparesis
1
Cellulitis
I
I
Foot Ulcers
Parkinson's disease
Blindness
Rheumatoid Arthritis
Bursitis
Unstable Angina
Chondromalacia
Peptic Ulcer Disease
Threat w/firearms
Drug seeking behavior
Suicidal Ideation
Dysphagia
Other Clinical Study
Age >90
20
19
2
1
2
1
5
3
18
1
16
1
2
13
1
3
3
4
3
8
1
1
3
19
168
MD Declination
Age<40
See Table 3.7
I
92
Justification and Explanation of Excluded Patients:
1. Renal Dysfunction:
Normal Scr ranges from 0.7 to 1.3 mg/dL with most adults having a Scr of
1 .Omg/dL49. Forty-five patients were excluded for isolated renal insufficiency
(Scr> 1.3). Thirty-three had mild renal dysfunction (1 .4<Scr<2.0), eight had moderate
renal dysfunction (2.1<Scr<3.0), and four had severe renal dysfunction (Scr>3.0).
Another 9 patients were excluded for combined renal and hepatic dysfunction.
Adequate renal function is essential in patients taking ibuprofen (the rescue analgesic),
as the potential for renal toxicity from ibuprofen increases as renal function decreases.
2. Hepatic Dysfunction:
Normal liver enzymes for healthy adults range from alkaline phosphatase
between 50-100 but it can vary dependant on assay method, SGOT between 8-42
IU/L, and total bilirubin between 0.3 and Img/dL49. Forty-six patients were excluded
for elevated alkaline phosphatase (31 patients), SGOT (10 patients), or total bilirubin
(5 patients). Acetaminophen is primarily metabolized in the liver. Adequate hepatic
function is essential to the metabolism of acetaminophen and the removal by
conjugation of hepatotoxins produced during the metabolism of acetarninophen.
Nine additional patients were excluded for combined renal and hepatic
insufficiency.
3.
Allergy to Acetaminophen or Ibuprofen:
Twenty-three patients were excluded for listed allergies to either
acetaminophen (3 patients) or to ibuprofen (20 patients). Allergy listings were taken at
face value and no attempt was made to document true "allergic" reaction versus
adverse drug reaction.
4. Ethanol Abuse:
Nineteen patients were excluded for a documented diagnosis of ethanol abuse
or for the known consumption of 3 or more alcoholic beverages per day. It has been
shown that alcoholic patients or heavy alcohol consuming patients had reduced
amounts of the conjugate needed during acetaminophen metabolism. Consequently,
they are at increased risk of acetaminophen induced hepatotoxicity.
5. Infectious Disease:
169
Three patients were excluded because of infectious disease considerations.
Two patients were carriers of Hepatitis B, while a third was undergoing treatment for
active tuberculosis. Since this study involves collection of saliva samples for analysis
these patients were excluded from the study as possible sources of biohazardous
samples.
6.
Drug Interactions:
Three patients were eliminated for drug interactions. Two patients were taking
phenytoin and 1 was taking cyclosporine. Acetaminophen is highly protein bound and
may compete with these medications for protein binding sites.
7.
Mental Status:
Five patients were excluded for a diagnosis of dementia and three more had
been ruled by the court as mentally incompetent. This study was not designed to
legally accommodate these groups of patients.
8.
Recent Trauma to Knees:
Eighteen patients were excluded for trauma or intra-articular injections in the
knee in the last 3 months.
9.
Birth Control:
Nearly 99% of the patients seen at the VA Outpatient clinic are male. Of the
females screened only one patient was excluded for insufficient birth control methods.
The patient was still pen-menopausal and therefore at risk of possible pregnancy.
10. Assistive Devices or Inability to Walk 50 Feet:
Twenty-two patients were excluded for inability to walk 50 feet without
assistance or assistive devices. Sixteen of those required a cane or walker. One patient
had henii-paresis secondary to a recent CVA, I patient had severe bilateral cellulitis of
the lower extremities, I had diabetic foot ulcers, 1 patient had Parkinson's disease, and
2 patients were legally blind.
11.
Concomitant Diseases:
Twenty-four patients were excluded for concomitant disease states. Thirteen
170
patients also had rheumatoid arthritis in the knees, I patient had bursitis, 3 patients
had unstable angina, 3 patients had chondromalacia, and 4 patients had active peptic
ulcer disease.
12.
High Risk Patients:
Twelve patients were excluded because they represented a danger to
themselves or to the investigator. Three were excluded for threatening medical
personnel with firearms, eight for drug seeking behavior, and 1 for suicidal ideation.
13.
Miscellaneous exclusions:
One patient was excluded for dysphasia that prevented swallowing of the
tablets and 3 patients were excluded because they were actively enrolled in another
clinical study.
The last two categories are listed as "Age" and "MD Declines Enrollment".
These are not part on the exclusion criteria per
Se.
Rather they can be best classified as
"Failures to Comply with the Inclusion Criteria."
14. Age:
Twenty people fell outside the age range. Nineteen of those were greater than
90 years of age and 1 was less than 40 years of age.
15. MD Declines Enrollment:
Permission for enrollment was declined for 92 patients. Thirty-two physicians
did not specify a reason for declining enrollment. Most reasons for declining
enrollment were a direct result of the acute problem that had brought the patient to
the clinic. Table 3.8 outlines all stated reasons for declining enrollment.
Table 3.8: Physician Reasons for Declining Enrollment
171
#Pt
Reason
Recent surgery
eye
1
Recent surgery
urology
1
Recent surgery
ankle
2
Recent surgery plastic surgery
4
Recent surgery
2
cardiac
Cancer
2
Foot ulcer
1
Infection
I
Deep Venous Thrombosis
5
Pancreatitis
1
Transient Ischemic Attack
1
Cerebral Vascular Accident
4
GI Bleed
1
Mental Health Issues
2
Rash
I
Eye Issues
I
Atrial flutter/tachycardia/angina
9
No Ibuprofen
1
Nurse Practitioner
7
Not Primary Care Provider
10
New Patient
3
Not Specified
32
After eliminating the 349 patients that did not satisfy all inclusion/exclusion
criteria, 359 patients remained. Every attempt was made to contact these patients
regarding enrollment in the study. One hundred twenty five of these patients were
172
unable to be contacted because they cancelled their appointments, did not show up
for their appointment at all, or were "missed" because of the interview or enrollment
of another patient. Of those patients approached, two hundred and four of them
declined enrollment in the study for reasons that ranged from "not interested" to "not
having pain at this time". Table 3.9 summarizes the reasons stated for nonenrollment.
Table 3.9: Patient Reasons for Non-enrollment into the Study.
Reason
#Pt
Cancelled Appointment
20
Did Not Show for Appointment
46
Recruiter Missed the Patient
59
Not interested
22
Not enough time
3
Too Many Pills
5
Doesn't want to change Meds
5
Leaving area for trip
2
Too far to Drive
103
Too much pain
25
No pain at this time
39
It should be noted that over half of the 204 patients approached declined
because it was too far for them to drive back to the clinic for follow-up evaluations.
The VA hospital outpatient clinic services a huge area of Oregon and Washington.
Patients are expected to travel several hundred miles for service at the clinic. Table
3.10 is a table of the cities that these 103 patients commute from to go to the clinic.
173
Table 3.10: Home City of 103 Declined Patients who Stated "Too far to Drive"
as the Reason for not Enroffing in the Study
City
# Patients
City
# Patients
Albany, OR
Astoria, OR
Banks, OR
Bend, OR
Boring, OR
Brownsville, OR
Canby, OR
Condon, OR
Corvaffis, OR
Eagle Creek, OR
Eugene, OR
Forest Grove, OR
Garibaldi, OR
Gervais, OR
Idanha, OR
Jefferson, OR
Junction City, OR
Klamath Falls, OR
Keizer, OR
Lapine, OR
Lebanon, OR
Lincoln City, OR
Manzanita, OR
Mcminnville, OR
Monmouth, OR
Newberg, OR
Newport, OR
8
3
Oregon City, OR
Otis, OR
Parkdale, OR
Redmond, OR
Rockaway, OR
Salem, OR
Sandy, OR
Seaside, OR
Silverton, OR
South Beach, OR
Stayton, OR
St. Helens, OR
Sweet Home, OR
The Dallas, OR
Tillamook, OR
Troutdale, OR
Woodburn, OR
Battleground, WA
Camos, WA
Kelso, WA
Longview, WA
Rainer, WA
I
I
I
I
2
Ridgefield, WA
Stevenson, WA
Vancouver, WA
Washougal, WA
Woodland, WA
1
I
2
2
1
1
1
3
1
2
I
I
I
1
I
1
I
1
I
3
I
I
I
2
I
3
22
I
2
1
I
2
1
1
1
5
1
2
1
1
1
2
1
I__________
1
1
Study Management:
An often ignored subject in the medical literature is the huge amounts of time,
effort, and true costs that are put into subject recruitment. Months of effort are often
reduced to a sentence that states "X number of patients were recruited over a XX
month period." Strict documentation must be kept on all patients screened for the
study, all excluded patients, all participating patients, and all patient withdrawals from
the study. The mechanics of this screening and documentation process are
174
tremendously complicated and tedious. Therefore, a small section of this thesis is
dedicated to the mechanics of the actual process.
Getting the Word Out:
The first step is notifying and educating the providers about the existence and
purpose of the study. Large signs were posted around the VA outpatient clinic. The
signs were a succinct listing of the name of the project, the inclusion/exclusion
criteria, and the contact personnel. In addition, short announcements were made
during clinic "grand rounds" for each group of physicians and one page protocol
summaries were passed out for staff reference. Lastly, "study cards", fashioned after
the business cards seen in the corporate world were printed and distributed to each
participating M.D.
Identifying patients:
Patients recruited for this study all had appointments with physicians at the
VA Outpatient Clinic. In preparation for these appointments, medical charts of each
patient were sent to the clinic on the day prior to the appointment. Using the VA
computer system, a list of all patients with appointments for the next day could be
printed for each physician. Once printed, patient online records were examined for a
diagnosis of osteoarthritis, basic patient information (age, weight, address, and phone
number), and laboratory values screened. Promising patient charts could then be
examined. On an average day, 60-80 names were printed on the M.D. lists. Of those,
about 10 could be eliminated on the basis of their age or diagnosis. An additional 40-
175
60 could be eliminated for not having the disease or for lab abnormalities. The
remaining 10-20 charts were reviewed for all inclusion/exclusion criteria. Those
charts belonging to eligible patients were marked with "Patient Identification Forms"
to notify the M.D. of the patient's eligibility for the study. A daily "HIT List" was
prepared. The physician of each targeted patient was approached at the beginning of
rounds and followed up with after the patient had been seen. Many patients also
required the permission of the attending physician as well as that of the resident MD.
Several physicians gave "blanket" authorization to their patients fitting the criteria,
while other refused participation to all their patients.
Patient Paperwork:
Packets were prepared in advance for the patient enrollment. Each enrollment
packet contained a checklist, a consent form, a questionnaire, prescriptions, "Study
cards", and study medication. The initial visit packet was fifteen pages in length.
Smaller packets of only 3 pages were needed for visits 2 and 3. Also, withdrawal
forms, patient progress lists, and completed study checklists were needed for each
patient. All in all, each patient's final file contained up to 30 pages of information that
must be kept organized and confidential. A dedicated, securable filebox was utilized
for the security and organization of all the forms and patient files. Folders containing
copies of all blank forms were kept inside. Each patient was assigned a separate folder
to minimize confusion.
176
Time and Estimated cost:
Each day of patient screening used 40-60 pages of paper. The VA clinic was
kind enough to donate the paper and ink for all the printed documents as well as the
use of their computers and printers. All other secretarial supplies were provided outof-pocket by the investigator. All chart review and drug dispensing was preformed by
a licensed pharmacist. Each recruitment day began with 7:00am rounds with the
resident MD's and ended at 5:30pm with the closing of the clinic. This adds up to a
total of 180 working days each 10 hours in length (minus 30 minute lunch daily).
For the sake of example, it is assumed that the investigator would provide all
supplies. Supply charges would include 50 pages paper/day with a misc, supply charge
of $5.00/week. Paper charges = $3.75/144 pages. Let it also be assumed that the
pharmacist performing the chart review and dispensing was reimbursed at normal
market rate ($27.00/br). Also assume that physician and patient participation were
not compensated. This study consisted of 180 working days each 10 hours in length.
Table 3.11: Estimated Cost of Study
Average of 50 pages/day
Misc. office supplies
Pharmacist salary
Estimated total cost
Per Month
For This Study
$26.04
$20.00
$5,400.00
$5,446.04
$234.38
$180.00
$48,600.00
$49,014.38
The estimated cost for the example study is nearly $50,000.00. Actual funding
was significantly less.
177
Recruitment Note:
An additional side note about the recruitment process. It is important for
recruiters to consider the age and social standards of the target population. In this
case, a majority of the patients were raised during a generation where women were
treated much differently than in today's society. These men responded better to a
female recruiter who was wearing "proper dress" i.e. a modest blouse and skirt, or a
one-piece dress. Recruitment attempts made while wearing pants were less successful.
I feel that similar negative reactions would have been obtained with male recruiters
with long hair or with an earring, as both were considered socially unacceptable to this
generation.
This particular population also responded poorly to medical personnel that
were of Asian descent. There were several incidents where patients refused to see
medical interns because their Asiatic appearance triggered flashbacks and made the
patient uncomfortable. This is hardly surprising as many of them are veterans of the
Korean and Vietnam wars and suffer from Post Traumatic Stress Disorder (PTSD). It
is also important to point out that the Veterans could not make a distinction between
the different Asiatic groups. Regardless if the person was Vietnamese, Chinese,
Japanese, or Laotian, the patients were still disturbed. Patient responses varied from
polite requests for a different person to patients hiding under chairs or physically
attacking the perceived threat. Factors such as these must be taken into consideration
when selecting recruiters as they may have a definite impact on patient response to
recruitment.
178
Patient Enrollment:
After all factors were taken into consideration, only thirty patients from the
original 13,483 files examined consented to enrollment in the study. All enrolled
patients were Caucasian males. Table 3.12 is a summary of demographic
characteristics.
Table 3.12: Demographics of 30 enrolled Patients
Characteristic
Average (range)
Age (years)
61.16 (44-76)
Height (inches)
71.16 (67-79)
Weight (pounds)
221.3 (145-268)
Sex
All Male
Race
All Caucasian
Smokers (percent)
40% (12 subjects)
These statistics are consistent with the published data on osteoarthritis of the
knee. The disease is known to increase as the patient ages3'5'6. The prevalence
increases from 4% in patients age 18-24 up to 85% in patients between 75-79 years of
age6. The incidence is also a function of weight and race. Americans and Europeans
have a higher incidence than Chinese or East Indians3'6. Weight is an aggravating
factor in the disease process3. In the 30 enrolled patients, all but 1 were at least 20
pounds over their ideal body weight with 19 subjects being 50 or more pounds above
ideal body weight. The incidence of osteoarthritis is generally greater in females than
in males3. As the population of patients at the VA Hospital is primarily male, no
estimates on female patients were available for comparison.
179
Severity and Grading of Osteoarthritis of the Knee:
All 30 patients had diagnostic radiological reports on file. Those reports that
were not available by computer could be found be accessing the older paper chart of
the patient.
Table 3.13: Distribution of enrolled patients by Severity and Radiological
grading of the Osteoarthntic Disease.
Grade of Osteoarthritic Disease
Number of Patients
Mild
7
Mild
Moderate
3
Moderate
7
Moderate Severe
5
Severe
4
Total Knee Replacement secondary to severe disease
4
Discussions with the radiology department at the VA hospital resulted in the
following guidelines for radiological interpretation42. Films are examined for the
presence of lateral or medial osteophytes, joint space narrowing, sclerosis, and cysts.
Each category is graded on a scale of 0-2, where Oabsent, I questionable, and
2=present. A rating of mild indicates the presence of osteophytes but no joint space
narrowing, sclerosis, or cysts. A rating of moderate indicates moderate multiple
osteophytes, some sclerosis, some cysts, and definite joint space narrowing. A rating
of severe indicates the presence of severe osteophytes, cysts, and sclerosis as well as
severe joint space narrowing. The ratings of mild-moderate and moderate-severe are
used when some, but not all of the criteria of the upper rating has been met, or to
180
indicate progression of the disease. In the case where both knees were affected by
osteoarthritis, the rating of the higher knee was used.
Withdrawal from the Study and Reported Side Effects:
Of the 30 patients who enrolled in the study, 17 completed the study. The
thirteen who withdrew cited a variety of reasons. Two patients withdrew before
taking any tablets. One cited a newly diagnosed rash as the reason and the other
decided that his moving to another city would not allow enough time.
Two patients were lost to follow-up. One elected to obtain medical care from
another facility and the other is missing and presumed dead by local police.
Seven patients withdrew during or after treatment one. Three cited new
diagnosis or acute injury as the reason (subject #19 shoulder injury, subject #30
emergency knee surgery, subject #23 new diagnosis of prostate cancer), one cited
inability to give up previous narcotic medication (subject #26 Vicodin®), one cited
uncontrolled pain (subject #21), and 2 cited intolerable side effects from the treatment
medication. Subject #20 reported drowsiness from the medication while subject #22
reported stomach upset, diarrhea, and insomnia. All are uncommon, but reported side
effects to acetan-iinophen. Four of these seven patients could have experienced
withdrawal due to the treatment. For subjects #26, #21, and #22, treatment 1 was
the immediate release acetaminophen. For subject #20, treatment #1 was the
sustained release acetaminophen formulation.
Two patients withdrew during treatment two. Subject #12 withdrew because
of uncontrolled pain. Lastly, Subject #9 withdrew because he experienced nausea,
181
stomach upset, and heartburn. Side effects for this subject were much worse during
treatment two than during treatment one. Treatment two for both subjects was the
immediate release acetaminophen formulation.
Side effects from the medication were reported by a total of eleven patients
during one or more treatments. Most side effects were reported as occurring for only
a short time. Reports were noted but no attempts were made to develop causal
relationships between these side effects and treatment during the study.
The incidence of these complaints did not vary significantly between the
immediate release and sustained release acetaminophen formulations. Table 3.14 is a
summary of reported side effects in all patients regardless of whether they completed
the study.
Table 3.14: Incidence of Side Effects to Study Medication By Formulation.
Side Effect
Total #
Reports
IR
SR
Drowsiness
5
2
3
Stomach
4
3
1
Upset___________
Nausea
3
1
2
Headache
2
1
1
Diarrhea
2
1
1
Dizziness
1
0
1
Heartburn
1
1
0
Insomnia
1
1
0
182
Verification of Patient Compliance:
After the end of each treatment, each patient returned the treatment cards in a
sealed envelope. Once the study had been completed those envelopes were
opened and the number of remaining tablets counted. Patients with treatment cards
that contained greater than I O% of the doses remaining were disqualified from the
study for non-compliance. Each treatment consisted of 224 total tablets. Patients
could miss up to 11 doses or 22 tablets without disqualification. None of the
seventeen patients that completed the study were disqualified for non-compliance.
The table below shows the number of "missed" doses in the seventeen patients that
completed the study. No patient missed more than 8 tablets or 4 doses of medication
during any given treatment. The average number of tablets missed during treatment
period 1 and treatment period 2 were 1.64 and 1.88 respectively. Several patients
stated that the convenient packaging of the medication had improved their compliance
with both the study mediation and their own regular medications. The packing of the
study apparently medication reminded them to take their other medications.
Table 3.15: Number of Tablets Missed by Patients During the Study
Treatments
183
# Tablets Missed
# Tablets Missed During
Patient #
During Treatment 1
Treatment 2
1
2
0
4
8
8
0
0
4
0
0
0
0
0
0
0
6
0
0
0
4
0
0
0
4
0
2
3
4
5
6
7
8
II
13
14
16
18
24
25
27
28
Average
8
2
0
0
0
0
4
1.64
0
6
1.88
Breakthrough Analgesic Quantification:
For humanitarian reasons, patients were supplied with ibuprofen 200mg (Advil
200mg tablets Lot 95 AG1019, exp. 4/97) tablets as a breakthrough analgesic. This
medication was available to the patients for use if the acetaminophen treatment was
not effective. A maximum of two ibuprofen tablets (400mg) twice a day was
permitted. Most patients did not require the breakthrough analgesia. Some patients
admitted to requiring additional analgesia in the evenings. Many stated that their pain
was adequately controlled during the day because there were busy working. In the
evenings, patients stated that they "stiffened up" and "had nothing else to think
about" other than their pain. One patient stated that the acetaminophen treatment
184
made him feel so much better that he "over did it". He needed rescue analgesia the
nest day. Table 3.16 shows the number of ibuprofen tablets taken by the seventeen
patients who completed the study.
Table 3.16: Number of Rescue Analgesic Tablets Needed by Patients during
the Study Treatments
Patient #
1
2
3
4
5
6
7
8
11
13
14
16
18
24
25
27
28
Average
# Tablets used during
Treatment 1
# Tablets used during
0
0
0
0
14
0
0
2
0
0
0
0
0
0
0
0
2
8
5
0
1.71
Treatment 2
0
10
0
0
0
4
0
0
0
9
0
0
3
5
1.94
Saliva Samples:
Each patient was asked to produce a saliva sample for analysis at three
different points during the study. The first sample was taken during visit I and served
as a baseline sample. The second sample was collected during visit 2 at the end of the
first treatment period. The third and last sample was collected during visit 3 at the end
of the second treatment period. Sample two and three should represent steady state
185
saliva acetarninophen concentrations for their respective treatments. Samples were
frozen after collected and analyzed using the techniques in Chapter 2. Salvia
acetaminophen concentrations in the seventeen patients completing the study are
shown in Table 3. 17. Note: most samples were taken about 4 hours after the second
dose and about 2 hours prior to the third dose of the day. The average values must
therefore by "decayed" to estimate true saliva troughs. Drug decay is influenced by
continued input from the SR dosage form in one case, but not for the JR dosage form
in the other case.
Table 3.17: Measured Saliva Acetaminophen Levels in Study Samples
Patient #
1
2
3
4
5
6
7
8
11
13
14
16
18
24
25
27
28
Average
Saliva APAP
Saliva APAP
concentration after
IR treatment (mg/L)
concentration after SR
treatment (mg/L)
2.5
2.8
2.3
6.7
7.0
6.8
6.8
6.3
6.2
7.4
6.7
5.9
6.4
6.3
6.8
7.9
6.7
6.4
6.4
7.0
6.68
1.7
1.9
2.8
3.7
2.7
1.8
3.0
1.9
2.5
4.1
2.4
2.8
2.6
3.0
2.61
Decaying the average saliva drug concentrations:
186
From the single dose studies in Chapter 2, the l( for the immediate release
product was calculated to be 0.3300 h1 and the Ke for the 5% sustained release
product was calculated to be 0.1331 h1. Using these estimates, the saliva
concentrations of drug can be "decayed" to approximate trough levels using the
equation C = Coet. In this equation recall that C is the concentration at any time t,
Co is the original concentration, IKe is the elimination rate constant, and t is the time in
hours that has elapsed between Co and C.
For the estimated JR trough:
C = 2.61 e
(03300)(2)
= 1.34 mg/L (range 0.87 1.9lmg/L)
For the estimated SR trough:
C = 6.68 e
(o.1331)(2)
= 5.11 mg/L (range 4.75 6.O5mg/L)
Recall from chapter 1 that salvia and serum acetaminophen concentrations are
approximately equa15154. If the IKe from the single dose study is representative of the
multiple dose Ke, then the formulation goal of a minimum acetaminophen plasma
level of 5mg/L has been accomplished.
187
PAIN AND DISABILITY QUESTIONNAIRE
The pain/disability questionnaires consisted of 12 questions plus the walking
test time. It was adapted from the Stanford Health Assessment Questionnaire (HAQ).
Three of the twelve questions concerned pain and pain characteristics, six questions
concerned disability, and three questions concerned the patient's medication and any
side effects from that medication. Raw data for all questions can be found in
Appendix 3D. Data analysis was performed only on the 17 patients completing the
study. Data were examined first for overall changes in average score for all 17
patients, then by treatment group. Those patients receiving the SR treatment as their
first treatment will be designated as treatment group SR-JR (n=8). Likewise those
patients receiving the JR treatment as their first treatment will be designated as
treatment group JR-SR (n=9).
Pain Evaluation
Question 1: How would you rate your overall pain during the last 4 weeks?
Patients were asked to rate their pain as 1 mild, 2moderate, or 3 severe.
Table 3.18: Average Score on Question 1 by Treatment Group
Tx Group
Visit 1
Visit 2
Visit 3
AverageAll
2.205
2.250
2.166
1.735
1.875
1.611
1.558
1.687
1.444
Average SR-JR
Average IR-SR
188
Question 2: How would you describe the change in your pain in the last 4 weeks?
Patients were asked to rate their pain as lbetter, 2=no change, or 3=worse.
These ratings were re-coded as 1 = better, 0 = no change, and I = worse for analysis.
Therefore a negative average change can be interpreted as a reduction the pain or as a
change for the "better". Baseline values were set = 0 as a reference point.
Table 3.19: Average Score on Question 2 by Treatment Group.
Tx Group
Visit 1
Visit 2
Visit 3
Average All
Average SR-JR
Average JR-SR
0.000
0.000
0.000
-0.294
-0.250
-0.333
-0.294
-0.250
-0.555
Question 3: My pain is best described as:
Patients were asked to rate their pain as I periodlic (comes and goes), 2daily
(occurs at least once a day), or 3=constant.
Table 3.20: Average Score on Question 3 by Treatment Group.
I
Tx Group
Average_All
[yrage SR-JR
iAverageJR-SR
Visit 1
Visit 2
Visit 3
2.352
2.125
2.555
2.117
2.125
2.111
2.176
2.250
2.111
All three questions in this section were designed to measure the type and
severity of pain that osteoarthritis patient experience. During the baseline evaluation
(Visit I), it became clear that on average these patients experience daily to constant
pain that is of moderate to severe. Most of these patients have historically treated
their symptoms with "as needed" pain medications. Only a few patients took regularly
189
scheduled pain medications. Questions 1 and 2 show that regardless of the treatment
group the severity of the pain decreased with routine pain medication administration.
In contrast, Question 3 shows that regardless of the pain medication or regimen
prescribed the description of their pain varied little with most patients still describing
their pain as occurring on a daily basis.
Disability:
The next 6 questions in the pain and disability questionnaire were targeted at
the degree of disability that each patient experiences. As before, data analysis was
performed only on the 17 patients completing the study. Data were examined first for
overall changes in average score for all 17 patients, then by treatment group. Those
patients receiving the SR treatment as their first treatment will be designated as
treatment group SR-JR (n=8). Likewise those patients receiving the JR treatment as
their first treatment will be designated as treatment group JR-SR (n=9). Patients were
asked to rate these tasks as I Seldom need help, 2sometimes need help, or 3 often
need help.
The questions were: I need help from another person to do the following:
Question 4: Dress
Table 3.21: Average Score on Question 4 by Treatment Group
TX Group
Average-All
Average SR-JR
Average JR-SR
Visit 1
Visit 2
Visit 3
1.117
1.125
1.111
1.000
1.000
1.000
1.058
1.000
1.111
190
Question 5: Eat
Table 3.22: Average Score on Question 5 by Treatment Group.
TX Group
Visit 1
Visit 2
Visit 3
Average-All
1.000
1.000
1.000
SR-JR
Average JR-SR
1.000
1.000
1.000
1.000
1.000
1.000
Average
Question 6: Stand up
Table 3.23: Average Score on Question 6 by Treatment Group.
Tx Group
Visit 1
Visit 2
Visit 3
Average-All
1.529
1.176
1.117
Average SR-JR
1.500
1.000
1.000
JR-SR
1.555
1.555
1.222
Average
Question 7: Walk
Table 3.24: Average Score on Question 7 by Treatment Group.
Tx Group
Visit 1
Visit 2
Visit 3
Average-All
1.235
1.058
1.176
Average SR-JR
1.375
1.125
1.250
JR-SR
1.111
1.000
1.111
Average
Question 8: Climb Stairs
Table 3.25: Average Score on Question 8 by Treatment Group.
Tx Group
Visit 1 Jisit 2
Visit 3
Average-All
1.588
1.647
1.294
SR-JR
Average JR-SR
1.625
1.750
1.125
1.555
1.555
1.444
Average
191
Question 9: Clean House or do everyday chores
Table 3.26: Average Score on Question 9 by Treatment Group.
Tx Group
Visit 1
Visit 2
Visit 3
AverageAll
1.235
1.250
1.222
1.235
1.125
1.333
1.235
1.125
1.333
Average SR-JR
Average JR-SR
Two things were clear to the investigator about these questions and are related
to observations made in the recruitment section of this paper. Both are personal
observations and cannot be supported or refuted by the data collected. The first
observation was that the presence or absence of a second person during the interview
might have affected the patient's answer to the disability questions. The second
person (usually the patient's spouse) tended to result in the patient reporting less
disability than if the patient was interviewed alone. This is not surprising as the
generation of veterans who participated in this study were raised to "act like a man"
and not admit weakness or disability. Unfortunately, records of other people present
at the interviews were not kept for inclusion in the analysis.
The second observation was that even when alone, the patients tended to
underestimate the effect that the disease has on their abilities. An example is the
answer to question 8 about climbing the stairs. Most patients stated that they seldom
needed help from another person to climb stairs, yet almost all patients requested to
use the elevator when going from the recruitment area of the clinic, downstairs to the
pharmacy one floor below. Several patients were later to admit that they "seldom
needed help from another person" to climb stairs because they just didn't do it at all.
This may be a function of individual pride or a fault in the way that the questions were
192
written. As mentioned previously, the generation from which this population was
drawn was taught as young men not to admit disability. As for the faulty questions,
future recruiters may consider either evaluating the disability themselves or developing
more specific questions for evaluation of disability and not relying on just patient
reported information.
Question 5 did not yield any information relative to this study. In retrospect, it
is easy to see why osteoarthritis of the knee did not have significant impact on the
eating habits of the enrolled patients.
Medication Efficacy and Side Effects
As before, data analysis was performed only on the 17 patients completing the
study. Data were examined first for overall changes in average score for all 17
patients, then by treatment group. Those patients receiving the SR treatment as their
first treatment will be designated as treatment group SR-JR (n8). Likewise those
patients receiving the JR treatment as their first treatment will be designated as
treatment group JR-SR (n9).
Question 10: The pain medication that I have been taking for the last 4 weeks
relieves my pain:
Patients were asked to rate pain relief provided by the medication taken for the
last 4 weeks as I = seldom, 2= sometimes, or 3often.
Table 3.27: Average Score on Question 10 by Treatment Group.
Tx Group
Visit 1
Visit 2
Visit 3
AverageAll
1.705
1.625
1.777
2.235
2.213
2.333
2.441
2.750
2.166
Average SR-JR
Average JR-SR
193
This question was included to help determine if the medication
(acetaminophen) was effective in relieving the pain. The increase in the average rating
could be the result of two separate effects. One may be the result of a decrease in the
pain because of chronic administration of the medication rather than "as needed" use.
The second may be the result of withdrawal of patients for whom the drug did not
work effectively. By the third evaluation, it is possible that only drug "responders"
remained in the study and that all drug "non-responders" had withdrawn from the
study due to lack of efficacy.
Question 11: The pain relief lasts for the entire time between doses:
Patients were asked to rank the duration of pain relief provided by the
medication taken for the last 4 weeks as I = seldom, 2sometimes, or 3often.
Table 3.28: Average Score on Question 11 by Treatment Group.
Tx Group
Visit 1
Visit 2
Visit 3
AverageAll
1.588
1.250
1.888
2.000
1.875
2.111
2.235
2.375
2.111
Average SR-JR
Average JR-SR
The baseline value for this question was 1.588±0.79 (n17). Verbally, this
indicates that patients often have breakthrough pain between doses of their baseline
medication. With regular dosing of the study medication, pain relief duration
increases to 2.000±0.71 (n17). By evaluation 3, the average had increased to
2.235±0.83 (n17). The same arguments can be used for this question as were used
for Question 10. The increase in pain relief could be due to either chronic medication
dosing or withdrawal of medication non-responders.
194
Question 12: In the last four weeks, have you had any side effects or bad reactions to
the medication?
This questions was extensively examined earlier in the paper with all side
effects reported by all enrolled patients examined. For the 17 patients completing the
study the percentage and type of side effects were as follows:
Table 3.29: Percentage of Side Effects Occurring by Treatment
%ptonlR
#ptonSR
%pton
Side Effect
# Pt Ofl JR Tx
Tx
Tx
SR Tx
Drowsiness
Headache
2
5.8%
2.9%
2.9%
2
1
5.8%
2.9%
2.9%
0
1
2.9%
Nausea/GI
1
1
1
upset_____________
Diarrhea
0
Time to Walk 50 Feet:
This test was designed to determine if pain relief could improve the knee's
functional status. Patients were asked to walk a total of 50 feet while being timed.
Patients would walk down a hallway 25 feet, pivot and return the same distance. Time
to walk 50 feet measurements were taken at each evaluation visit. As before, data
analysis was performed only on the 17 patients completing the study. Data were
examined first for overall changes in average score for all 17 patients, then by
treatment group. Those patients receiving the SR treatment as their first treatment
will be designated as treatment group SR-JR (n=8). Likewise those patients receiving
the IR treatment as their first treatment will be designated as treatment group JR-SR
(n 9).
195
Table 3.30: Average Time to Walk 50 Feet by Treatment
Tx Group
Average-All
Average SR-JR
Average JR-SR
Visit 1
Visit 2
Visit 3
17.00
15.70
18.00
15.68
14.88
14.40
15.29
15.31
16.02
196
STATISTICAL ANALYSIS
Comparing the sustained release acetaminophen treatment to the immediate
release acetaniinophen treatment:
The first and primary goal of this investigation was to determine if the
sustained release acetaminophen formulation described in chapters 1 and 2 was as
effective in relieving osteoarthritis pain as the immediate release product. Each
question asked in the pain and disability questionnaire had three discrete answers. It
was therefore decided that the discreteness of the data violated the assumption of
normality. Nonparametric analysis techniques were chosen to analyze the data. The
Signed Rank Test was performed on all questions to address the differences between
the SR and the JR acetaminophen treatments.
Table 3.31: Results of the Signed Rank Test Comparing the Immediate Release
Acetaminophen Treatment to the Sustained Release Treatment.
#PREFER
QUESTION
#PREFER
IR
SR
#TIE
PVALUE*
D
1
5
5
7
2
3
4
4
7
5
2
13
16
5
2
0
0
6
1
0
7
1
1
8
3
5
9
2
0
17
16
15
9
15
10
1
7
9
11
4
6
7
1
0
1.00
1.00
1.00
1.00
1.00
1.00
0.73
1.00
0.07
0.75
* p-values are two-sided and obtained from multiplying the cumulative binomial
probability by two.
197
Interpreting the results of the sustained release acetaniinophen treatment to the
immediate release acetarninophen treatment:
The p-values calculated above showed no difference in the sustained release
acetaminophen treatment and the immediate release treatment in all but one question.
Question 5 did not provided any information to this study. As previously discussed, in
retrospect it is easy to see why osteoarthritis of the knee does not effect the ability of
the patient to eat. In Question 10, patient preferred the immediate release
acetaminophen treatment over the sustained release acetaminophen for the pain relief.
It is possible that patients were expecting pain relief immediately after taking the
tablets. If so, because of the higher peak of the immediate release formulation
patients may have perceived the immediate release acetarninophen as relieving pain
better than the sustained release acetaminophen. All other questions including the
duration of pain relief and effect on disability questions showed that 2.6grams/day of
sustained release acetarninophen was as effective as 4grams/day of immediate release
acetaminophen in this population.
This is an exciting conclusion because, while the two treatments utilize the
same drug, the dose and frequency of administration are significantly less for the
sustained release formulation. Using only 2.6 grams of sustained release
acetaminophen was as effective as using 4 grams of immediate release acetaminophen
per day in reducing disability and improving the duration of pain relief. The lower
amount of drug required could potentially reduce some of the risks of liver toxicity
and other side effects in patients such as these that require chronic pain management
with acetaminophen. The twelve hour dosing frequency that the sustained release
198
product provides improves the convenience of the medication and could increase
compliance with the medication regimen.
Comparing the sustained release acetarriinophen treatment to the baseline treatment:
The previous analysis of the questionnaire showed that the immediate release
acetaminophen treatment was the same as the sustained release acetaminophen
treatment in treating disability and pain relief duration. While important to this study,
it is also necessary to determine if either the immediate release or the sustained release
acetaminophen formulations were effective at all. It is possible that the results simply
indicate that both treatments are equally poor at treating pain and improving disability
in osteoarthritis patients.
To test whether or not the acetarninophen treatments were effective, the
analysis described above must be repeated. This time the sustained release
formulation will be compared to the baseline medication values for each questionnaire
question. The baseline measurements represent a collection of different medications
and treatment regimens that were currently in use by the patients before they were
recruited for the study. Treatment ranged from no medication at all, to intermittent
dosing with anti-inflammatory drugs and immediate release acetarninophen, to
scheduled dosing with anti-inflammatory drugs, to intermittent narcotic analgesic
dosing.
199
Table 3.32: Results of the Signed Rank Test Comparing the Sustained Release
Acetaminophen Treatment to the Baseline Treatment
TIED
QUESTION
#PREFER
1
9
1
7
2
3
8
3
6
8
4
5
4
1
5
2
0
6
6
0
0
14
17
7
2
1
14
8
5
4
8
9
1
0
16
10
9
3
5
11
9
1
7
#PREFER
PVALUE*
BASELINE
SR
11
0.02
0.23
0.39
1.00
0.03
1.00
1.00
1.00
0.15
0.02
* p-values are two-sided and obtained from multiplying the cumulative binomial
probability by two.
Interpreting the results of the sustained release acetaminophen treatment to the
baseline treatment:
For the pain evaluation questions (questions 1-3) the results were
encouraging. All three questions suggested that the sustained release acetaminophen
treatment was a significant improvement over the baseline treatments. Patients rated
their pain as being less severe on the sustained release acetaminophen treatment. The
average pain score dropped from 2.20 (between level 2 = moderate and level 3 =
severe) to 1.65 (between level I = mild to level 2 = moderate). During the four week
treatment, patients described their pain as better and as occurring less often.
For the disability questions, only one of the questions showed a statistical
difference between the sustained release acetaminophen treatment and the baseline
treatments. This was Question 6. Recall this question evaluated how much help the
200
patients required to stand. The average answer after the baseline treatment was 1.53.
After the sustained release treatment the score dropped to 1.12. Although both
treatments fall between "I seldom need help" (level = 1) and "!sometimes need help"
(level =2), the improving score is encouraging. These patients often experience pain
in their knees and have difficulty standing up because of the physical changes
occurring secondary to the disease state. If the sustained release acetaminophen
treatment can relieve at least part of the discomfort associated with the activity of
standing, it can be considered successful.
The most encouraging portion of the analysis was the statistically significant
improvement in the medication efficacy and duration of action questions. In both of
these questions, a statistically larger number of patients felt that the sustained release
acetaminophen treatments both relieved their pain and relieved the pain for a longer
period of time than the baseline treatments.
Although no statistical analysis was performed on the time to walk 50 feet
data, the average time after the sustained release acetaminophen treatment was 1.65
seconds less than the average time after the baseline treatments. Perhaps the
reduction in time is representative of improvement that occurred because of the
reduction in pain and improved duration of action of the sustained release treatment.
201
CONCLUSIONS
Thirty men between the ages of 44 and 76 were recruited for a double blind
crossover study comparing two different acetarninophen formulations. Seventeen
patients completed the study. In those seventeen patients, the estimated trough
acetaminophen concentrations were 1.34mg/L and 5.11mg/L for the immediate
release and sustained release formulations respectively. Estimated plasma
concentrations for the sustained release formulation met and exceeded the target
multiple dose plasma concentration of 5mg/L. Patients were adequately compliant
with the study protocols and used appropriate amounts of the ibuprofen rescue
analgesic. Twelve questions designed to evaluate pain, disability, and medication
efficacy were asked at three different occasions throughout the study. Time to walk
50 feet measurements were also taken at these intervals. Signed Rank tests performed
on these questions in the
two
formulations showed only one statistical difference
between the two treatment groups regardless of the large difference in total daily dose
(2.6grams/day for the SR group vs. 4 grams/day for the JR group. Patients preferred
the immediate release treatment over the sustained release treatment for pain relief.
Additional Signed Rank tests performed on the baseline treatments and the SR
treatments showed statistically significant improvements in the patients average overall
rating of their pain levels, the ability of these patients to stand without help from
another person, and in the duration of pain relief that these patients received from
their treatment medication. Unchanged throughout this study is the fact that these
patients live with moderate to severe pain that occurs at least daily in all of these
202
patients. The SR treatment did manage to slightly reduce the disability due to this pain
and increase the duration of pain relief that these patients experience while reducing
the total acetaminophen dose to 2.6 grams per day. Follow up studies are necessary to
validate these findings due to the small sample size in this study. However,
preliminary results in these patients are promising.
Overall, the SR formulation succeeded in meeting the formulation goals
described in Chapter 1. Improvements in duration of pain relief and steady state
plasma levels of 5mg/L were achieved as a result of careful design and testing of the
preparation. Incorporation of pharmacodynamic information into the pharmaceutical
design process has the potential to change the development techniques of the future.
The current drawback to this technique is the lack of information about the minimum
effective plasma concentrations for most drugs. Whenever available, this information
could be used to prepare target formulations that improve efficacy and reduce side
effects in patients by allowing administration of the minimum effective amount of
medication.
203
REFERENCES
1.
Hossain, M. and Ayres, J.W., J. Pharm. Sci 81, 444-448 (1992).
2.
Hossain, M. and Ayres,J.W., Int.J. Pharm., 133, 223-235 (1996).
3.
DiPiro, J.T., Talbert, R.L., et. a/., eds.: Pharmacotherapy: A Pathop4ysiologicApproach,
2nd ed., Norwalk, Connecticut, Appleton & Lange, 1993. pp.1330-1342.
4.
Pinals, R.S., C/in. Ther., 14, 336-335 (1992).
5.
Felson, D.T., et a/.,Arthritis Rheum., 30, 914-918 (1987).
6.
Al Arfag, A. and Davis, P., Drugs., 41 (2), 193-201 (1991).
7.
Jollow, D.J., Thorgeirsson, S.S., Potter, W.Z., and Mitchell, J.R., Pharmaco/ogy. 12,
251-271 (1974).
8.
Barker, J.D., Dc Carle, D.J., and Anuras, S., Ann. Intern. Med., 87, 299-301
(1977).
9.
Whitcomb, D.C. and Block, G.D.,JAMA. 272 (23), 1845-1850 (Dec 21, 1994).
10.
Strom, B.L., JAMA., 272 (23): 1866-1867 (Dec 21, 1994).
11.
Gennaro, A.R. ed.: Remington's Pharmaceutical Sciences, 17th Edition.
Easton, Pennsylvania, Mack Pub. Co., 1985, pg. 1111.
12.
Gilman, A.G., Rall, T.W., Nies, A.S., and Taylor, P., eds.: The Pharmaco/ogicaly
Basis of Therapeutics, 8th ed., New York, New York, Macmillan, 1990. pp. 656-659.
13.
Eriksson, L.S., et. al., J. mt. Med. 231, 567-570 (1992).
14.
McEvoy, G.K., ed., AHFS Drug Information 90., Bethesda, Maryland., ASHP Inc.,
1990. pp. 1104-1109.
15.
Strubelt, 0.; Obermeier, F., and Siegers, C.P., Acta. Pharmacol. Toxicol. 43, 211218(1 978).
16.
Black, M. and Raucy, J., Ann. Intern. Med. 104 (3), 427-428 (1986).
17.
Emby, D.J. and Fraser, B.N., S. Afr. Med. J. ,51, 208-209 (1977).
204
18.
Goldfinger, R., et. al., Am.J. GastroenteroL ,70, 385-388 (1978).
19.
McClain, C.J., et. aL,JAMA. 244 (3), 251-253
20.
Licht, H., Seeff, L.B., and Zimmerman, H.J., Ann. Intern. Med. 92, 511
Ouly
18, 1980).
(1980).
21.
LaBrecque, D.R. and Mitros, F.A., Gastroentero/ogy., 78 (5), 1310 (1980).
22.
Gerber, M.A., et. a/., Hum. Path. 2 (1), 37-42 (1980).
23.
Johnson, M.W., Friedman, P.A., and Mitch, W.E., Am. J. Gastroentero/.,
76, 530-533 (1981).
24.
Black, M., et. al., Dig. Dis. Sci. 27 (4), 370-374 (1982).
25.
Levinson, M., Hosp. Pract., 18, 48N-48S (1983).
26.
Himmeistein, D.U., Woolhandler, S.J., and Adler, R.D., Am. J. Gasteroentero/. 79
(9), 718-720 (1984).
27.
Fleckenstein, J.L., N. Eng/. J. Med., 313, 48 (1985).
28.
Leist, M.H., Gluskin, L.E., and Payne,J.A.,J. C/in. Gasteroentero/. 7: 55-59 (1985).
29.
Seeff, L.B., et. aL,Ann. Intern. Med. 104, 399-404 (1986).
30.
Kartsonis, A., Reddy, K.R., and Schiff E.R., Ann. Intern. Med. 105, 138-139
(1986).
31.
Kumar, S. and Rex, D.K.,Arch. Intern. Med. 151, 1189-1191 (1991).
32.
Bonkovsky, H.L.,JAMA. 274 (4), 301
33.
Benson, G.D., C/in. Pharmacol. Ther. 33, 95-101 (1983).
34.
Hall, A.H., Kulig, K.W., and Rumack, B.H., Ann. Intern. Med., 105 (4), 624
duly
26, 1995).
(1986).
35.
Hall, A.H., Kulig, K.W., and Rumack, B.H., Dig. Dis. Sci., 32 (5), 558 (1987).
36.
Hall, A.H.; Kulig, K.W., and Rumack, B.H.,JAM/1., 256 (14), 1893 (Oct 10,
1986).
205
37.
Read, R.B., Tredger, J.M., and Williams, R., Hum. Toxicol., 5, 201-206
(1986).
38.
Rumack, B.H., Peterson, R.C., Koch, G.G., and Amara, l.A., Arch. Intern.
Med., 141, 380-385 (Feb 23, 1981).
39.
Ramey, D.R., Raynauld,J. and Fries, J.F., Arthritis Care Res., 5, 119-129 (1992).
40.
Brown,J.H., et. al.,Am.J. Public Health, 74,159-161(1984).
41.
Wolfe, F., et. a/.,J. Rheumatoi 15 (10), 1480-1488 (1988).
42.
Fries,J.F., Spitz, P.W., and Young, D.Y.,J. Rheumatol., 9 (5), 789-793 (1982).
43.
Liang, M.H. and Jette, A.M., Arthritis Rbeum., 24 (1), 80-86 (1981).
44.
Fries,J.F., et. al.,ArthritisRheum., 23(2), 137-145 (1980).
45.
Meehan, R.F., Gertment, P.M., and Mason, J.H., Arthritis Rheum., 23 (2), 146152 (1980).
46.
Bradley,J.D., et. al., N. Engl. J. Med., 325 (2), 87-91 (July11, 1991).
47.
Bradley,J.D., et. al.,j Rheumato/., 19 (12), 1950-1954 (1992).
48.
Amadio, P. and Cummings, D.M., Curr. Ther. Res., 34 (1), 59-66 (1983).
49.
Traub, S.L., ed., Basic Skills in Inteireting Laborato!y Data, 2nd ed.,
Bethesda, Maryland, ASHP Inc., 1996., pp. 213-244.
50.
Personal communication with Dr. ChristopherJ. Salmon MD., Radiologist at
the VA Hospital, Portland, Oregon.
51.
Glynn, J.P., and Bastain, W., J. Pharm. Pharmaco/., 25, 420-421 (1973).
52.
Ahmed, M. and Enever, R.P.,J. C/in. Hosp. Pharm., 6, 27-38 (1981).
53.
Adithan, C. and Thangam,J., Br. J. C/in. Pharmacol., 14, 107-109 (1982).
54.
Bonn, M.T. and Ayres, J.W., Im'. j Pharm., 54, 199-209 (1989).
55.
Montgomery, D.C., Design andAnaLysis of Experiments, 3rd ed., New York, New
York, John Wiley & Sons, 1991, pp. 134-175.
206
56.
Chow, S. and Liu, J., Deszgn and Anaiysis of Bioavailibiliéy and Bioequi valance Studies,
New York, New York, Marcel Dekker Inc., 1992, pp.23-47.
207
CONCLUSIONS
In the past the formulation of tablets has been approached in a haphazardly or
trial-and error approach. The idea of using the desired pharmacodynaniic properties
of the medication to formulate the tablet product has not received the attention that it
deserves. This thesis successfully used the suggested minimum plasma concentrations
for acetaminophen to simulate, design and formulate a sustained release
acetaminophen product. Other information that contributed to the positive outcome
of this thesis included knowledge of patient compliance habits and characteristics of
the target disease.
Although encouraging, the results of the Phase II clinical trial described in this
thesis cannot be considered conclusive without additional trials in a significantly larger
number of patients. In addition, more accurate and quantitative measures of pain and
disability would be desirable in the larger studies to reduce the dependence of the
investigator on subjective, "hearsay" information from the patient. More quantitative
measures of pain and disability would also reduce some of the statistical error in the
analysis.
Future studies are also needed to examine the role of the placebo effect in the
sustained release acetarninophen product. It is possible that once the placebo doses
that were used in this study are eliminated, the product might "lose" some of its
effectiveness because of a perceived difference in effect between the four doses per
day used in this study and the two doses per day that actually contain drug. A
crossover study could be developed that compared immediate release acetaminophen
208
I000mg four times a day, with the sustained release acetatninophen 1300mg twice a
day, with and without placebo controls.
That should expose any placebo effects that
are confounding the data.
Sustained release acetaminophen may also have applications in other chronic
disease states as well. Although primarily an inflammatory disease, rheumatoid
arthritis patients may also benefit from additional pure analgesic medication. Other
chromic pain disorders such as fibromyalgia, trigeniinal neuralgia, chromic back pain,
and chronic fatigue syndrome may also find uses for sustained release acetaminophen.
Lastly, sustained release acetaminophen has the potential to reduce the severity
of acetarninophen overdoses. Most hospitals admit an average of 1-2 patients per
week with some type of accidental or intentional acetaminophen overdose. Products
with slower release give rescuers more time after ingestion to remove the tablets from
the system and to administer the appropriate antidote. New nomograms for overdose
treatment would need to be developed for these new products since the peak drug
release would be delayed when compared to the immediate release products.
Rational drug formulation design has exciting implications in the field of
Biophamaceutics. Drug development often takes years. The use of phamacodynamic
information could result in drug products that are more disease state oriented. Both
patients and drug companies could benefit from additional studies in this area.
209
BIBLIOGRAPHY
Abramowicz, M. ed. The Medical Letter: On Drugs and Therapeutics. June 21, 1996,
38(977), pp.55-56.
Adithan, C. and Thangam,J., Br. J. C/in. Pharmaco/., 14, 107-109 (1982).
Ahmed, M. and Enever, R.P.,J. C/in. Ho.rp. Pharm., 6, 27-38 (1981).
Al Arfag, A. and Davis, P., Drugs., 41 (2), 193-201 (1991).
Amadlio, P. and Cummings, D.M., Curr. Ther. Res., 34 (1), 59-66 (1983).
Barker,J.D., De Cane, Dj., and Anuras, S., Ann. Intern. Med., 87, 299-301 (1977).
Benson, G.D., C/in. Pharmacol. Ther. , 33, 95-101 (1983).
Black, M. and Raucy,J., Ann. Intern. Med. 104 (3), 427-428 (1986).
Black, M., et. al., Dig. Dis. Sci. 27 (4), 370-374 (1982).
Bonkovsky, H.L., JAMA 274 (4), 301 (July 26, 1995).
Bonn, M.T. and Ayres,J.W., mt. J. Pharm., 54, 199-209 (1989).
Bradley,J.D., et. al.,J. Rheumatol., 19 (12), 1950-1954 (1992).
Bradley,J.D., et. al., N. Engl. J. Med., 325 (2), 87-91 (July 11, 1991).
Brown,J.H., et. al., Am.j Public Health, 74, 159-161 (1984).
Chow, S. and Liu, J., Design andAnaLysis of Bioavailibiliy and Bioequiva/ance Studies, New
York, New York, Marcel Dekker Inc.
Dighe, S.V.; Wiffiams, R.L., in: "Guidance Oral Extended (Controlled) Release
Dosage Forms In Vivo Bioequivalence and In Vitro Dissolution Testing." Food
and Drug Administration, Division of Bioequivalence, Office of Generic
Drugs, Rockville, MD, 1993. pp. 1-13.
Dipiro, J.T., in "Pharmacotherapy: A Pathoph5siologic Approach", Elsevier Science
Publishing Co. New York, NY, 1989, pp.646-648.
210
DiPiro, J.T., Talbert, R.L., et. aI., eds.: Pharmacotherapy: A PathpIysiologic Approach, 2nd
ed., Norwalk, Connecticut, Appleton & Lange, 1993. pp.I33O-l342.
Drug Information Fulltext (DIE): Acetaminophen Monograph, Computer Software.
Silver Platter FT 1.11, 1995.
Ebube, N.K.; Hikal, A.H.; Wyandt, C.M.; Beer, D.C.; Miller, L.G.; Jones, A.B., Phar.
Dev. Tech. 1997, 2(2), pp.161-170.
Emby, D.J. and Fraser, B.N., S. Afr. Med. J. ,51, 208-209 (1977).
Eriksson, L.S., et. al., J. mt. Med. 231, 567-570 (1992).
Felson, D.T., etal., Arthtitis Rheum., 30, 914-918 (1987).
Fleckenstein,J.L., N. Engl. J. Med., 313, 48 (1985).
Fries,J.F., et. al.,ArthritisRheum., 23 (2), 137-145 (1980).
Fries,J.F., Spitz, P.W., and Young, D.Y.,J. RheumatoL, 9 (5), 789-793 (1982).
Gennaro, A.R. ed.: Remington's Pharmaceutical Sciences, 17th Edition. Easton,
Pennsylvania, Mack Pub. Co., 1985, pg. 1111.
Gerber, M.A., et. al., Hum. Path. 2 (1), 37-42 (1980).
Gilman, A.G., Rail, T.W., Nies, A.S., and Taylor, P., eds.: The Pharmacologicalv Basis of
Therapeutics, 8th ed., New York, New York, Macmillan, 1990. pp. 656-659.
Glynn,J.P., and Bastain, W.,J. Pharm. Pharmacol., 25, 420-421 (1973).
Goldfinger, R., et. aL, Am. J. GastroenteroL , 70, 385-388 (1978).
Hall, A.H., Kulig, K.W., and Rumack, B.H., Ann. Intern. Med., 105 (4), 624 (1986).
Hall, A.H., Kulig, K.W., and Rumack, B.H., Dig. Dis. Sci., 32 (5), 558 (1987).
Hail, A.H.; Kulig, K.W., and Rumack, B.H.,JAM/1., 256 (14), 1893 (Oct 10, 1986).
Himmeistein, D.U., Woolhandler, S.J., and Adler, R.D., Am. j GasteroenteroL 79 (9),
718-720 (1984).
Hossain, M. and Ayres,J.W., mt. J. Pharm., 133, 223-235 (1996).
211
Hossain, M. and Ayres,J.W.,i Pharm. ScL 81, 444-448 (1992).in "The Merck Index,
Eleventh Edition" p.8
Insel, P.A., in "Goodman and Gilman's: The Pharmacological Basis of Therapeutics.
8t1 Edition," Pergamon Press, mc, Elmsford, NY, 1990, pp.656-659.
Insel, P.A., in "Goodman and Gilman's: The Pharmacological Basis of Therapeutics.
8thEdition, Pergamon Press, Inc. Elmsford, NY, 1990, p. 1655.
Johnson, M.W., Friedman, P.A., and Mitch, W.E., Am. J. Gastroenterol., 76, 530-533
(1981).
Jollow, D.J., Thorgeirsson, S.S., Potter, W.Z., and Mitchell,J.R., Pharmacology. 12, 251271 (1974).
Kartsonis, A., Reddy, K.R., and Schiff, E.R.,Ann. Intern. Med. 105, 138-139 (1986).
Kumar, S. and Rex, D.K.,Arch. Intern. Med. 151, 1189-1191 (1991).
LaBrecque, D.R. and Mitros, F.A., Gastroenterology., 78 (5), 1310 (1980).
Lachman, L., Lieberman, H., and Kanig, J.: The Theoy and Practice of Industrial Pharma'y.
Lea & Febiger.Philadelphia, PA. 1986. pp. 297-303.
Leist, M.H., Gluskin, L.E., and Payne, J.A., J. C/in. Gasteroenterol. 7: 55-59 (1985).
Levinson, M., Hosp. Pract., 18, 48N-485 (1983).
Liang, M.H. andJette, A.M.,ArthritisRheum., 24(1), 80-86 (1981).
Licht, H., Seeff L.B., and Zimmerman, H.J., Ann. Intern. Med. 92, 511 (1980).
Loeb, S., in "P4ysician's Drug Handbook. 5th Edition," Springhouse Co. Springhouse, PA,
1993, pp.2-3.
Mansell, L. Ph. D. Thesis, Chapter 3:page 261-262 (1985).
McClain, C.J., et. al.,JAJVIA. 244 (3), 251-253 (July 18, 1980).
McEvoy, GK., ed., AHFS Drug Information 90., Bethesda, Maryland., ASHP Inc.,
1990. pp. 1104-1109.
Meehan, R.F., Gertment, P.M., and Mason, J.H., Arthritis Rheum., 23 (2), 146-152
(1980).
212
Montgomery, D.C., Deszn andAna'ysis of Experiments, 3rd ed., New York, New York,
John Wiley& Sons, I991, pp. 134-175.
Personal communication with Dr. ChristopherJ. Salmon MD., Radiologist at the VA
Hospital, Portland, Oregon.
Peterson, R. G. and Rumack, B. H., Pediatrics, 62, 877-879 (1978).
Phuapradit, W. and Bolton, S., Drug Dev. &Ind. Pharm., 17(8), 1097-1107 (1991).
Pinals, R.S., C/in. Ther., 14, 336-335 (1992).
Prescott, L.F., Br. J. C/in. Pharmac. 10, 291S-298S (1980).
Radebaugh, G.W.; Murtha, J.L.; Glinecke, R. United States Patent No. 4,820,522:
"Oral Sustained Release Acetaminophen Formulation and Process," Mcneilab,
Inc., Spring House, PA, 1989.
Ramey, D.R., Raynauld,J. and Fries,J.F.,Arthritis Care Res., 5,119-129 (1992).
Read, R.B., Tredger,J.M., and Williams, R., Hum. Toxicol., 5, 201-206 (1986).
Rumack, B.H., Peterson, R.C., Koch, G.G., and Amara, l.A., Arch. Intern. Med., 141,
380-385 (Feb 23, 1981).
Sahajwalla, C.G. and Ayres,J.W.,J. Pharm. Sd., 80(9), 855-860 (1991).
Seeff, L.B., et. al., Ann. Intern. Med. 104, 399-404 (1986).
Shargel, L.; Yu, A.B.C.,in :Applied Biopharmaceutics and Pharmacokinetics, Third
Edition," Appleton and Lange, Norwalk, CN, 1993, p. 138.
Shargel, L.; Yu, A.B.C.,in :Applied Biopharmaceutics and Pharmacokinetics, Third
Edition," Appleton and Lange, Norwalk, CN, 1993, pp.170-175.
Shargel, L.; Yu, A.B.C.,in:"Applied Biopharmaceutics and Pharmacokinetics, Third
Edition," Appleton and Lange, Norwalk, CN, 1993, pp.353-357.
Strom, B.L., JAMA., 272 (23): 1866-1867 (Dec 21, 1994).
Strubelt, 0.; Obermeier, F., and Siegers, C.P., Acta. Pharmacol. Toxico/. 43, 211-218
(1978).
Traub, S.L., ed., Basic Skills in Inte?preting Laboratory Data, 2nd ed., Bethesda, Maryland,
ASHP Inc., 1996., pp. 213-244.
213
Van Bommel, E.M.G., Raghoebar, M., and Tukker, J.J., Biop harm. Drug Disposit, 12,
355-366 (1991).
Van Tyle, W.K., in "Handbook of Nonprescription Drugs. 9th Edition", American
Pharmaceutical Association, Washington, D.C.,1 990, pp.70-7l.
Walson, P.D., et. al., C/in. Pharmaco/. Ther., 46, 9-17 (1989).
Walson, P.D.; Galletta, G.; Braden, N.J.; Alexander, L. C/in. Pharmco/. Ther. 1989, 46, 917.
Whitcomb, D.C. and Block, G.D.,JAMZ4. 272 (23), 1845-1850 (Dec 21, 1994).
Wilson,J.T., et. a/., Ther. DrugMonit., 4, 147-180 (1982).
Wilson, J.T.; Brown, R.D.; Bocchini, J.A.jr.; Kearns, G.L. Ther. Drug Monit. 1985, 7, 211.
Winter, M.E., in !IBasic Clinical Pharmacokinetics. Second Edition," Applied
Therapeutics, Inc. Vancouver, WA, 1988, pp.7-99.
Wolfe, F., et. aI.,J. RheumatoL 15 (10), 1480-1488 (1988).
214
Appendix 2A
Copy of the Approved Application for Human Trials
to the Oregon State University Committee for the
Protection of Human Subjects
215
571.5
Copy of Approved Investigational Research Board Proposal from Oregon State
University.
RESEARCH PROPOSAL INVOLVING HUMAN TEST SUBJECTS
This is a preliminary investigation conducted by Oregon State University College
of Pharmacy Department of Pharmaceutics to evaluate a sustained released formulation
of acetaminophen (Tylenol®). The information collected will be used to establish an in
vivo correlation for the development of a new acetaminophen formulation. An in
vitro
in
vitro
in vivo
correlation will allow the in
vitro
behavior of future formulations to predict in
vivo behavior. New formulations can then be developed with a minimum of human
testing.
Acetaminophen is a widely used, over-the-counter medication for analgesia and
fever. It has been available to the general public for over 30 years. Acetaminophen is
currently given either as an immediate release product (650-1000mg every 4-6 hours) or
as an extended release product (1 300mg every 8 hours). A new sustained release
formulation developed in our laboratory would provide 1300mg every 12 hours. The
sustained release tablets are manufactured using well known procedures and are made
from Food and Drug Administration (FDA) approved ingredients.
Participants will be involved in several one (1) day test periods with a seven (7)
days wash out period between them. Participants will be asked to fast for 2 hours prior
to receiving a dose of acetaminophen. At specified time intervals after dosing,
participants will be asked to chew a one inch square of Parafilm® for 1 minute to
stimulate saliva production and to collect a saliva sample. It has been well documented in
216
the literature that saliva acetaminophen concentrations are directly correlated with blood
acetaminophen concentrations. All operators handling samples will wear gloves in
compliance with federal "universal precaution" recommendations. All operators are
aware of the risks of handling bio-hazardous materials including the potential for
contracting hepatitis and/or the HIV virus.
Justification: Currently available formulations of acetaminophen must be taken
every 4 to 8 hours to maintain adequate drug concentrations in the blood to provide pain
relief. The development of a sustained release formulation would provide extended relief
from pain while minimizing the dose, and thereby the side effects of the drug. Twelve
hour dosing intervals have also been shown to increase the compliance of patients. This
is especially important in patients who require pain relief on a long term basis (arthritis).
Although simulation and calculations may be performed to predict the behavior
of new drug formulations, there are often factors in the body that cannot be foreseen.
The ultimate test of a formulation measures the change in drug concentrations in the
body over the dosing interval. As acetaminophen saliva concentrations can be direcdy
correlated with plasma concentrations, saliva data can be used as a non-invasive method
of evaluating the performance of new acetaminophen formulations.
Figure 1 is a comparison of in
vitro
release rates of 3 acetaminophen formulations.
The diamonds represent the dissolution of 1000mg (2 x 500mg) acetaminophen (Tylenol
Extra Strength®) tablets. The filled circles show a similar curve for 1300mg (2 x 650mg)
acetaminophen extended release (Tylenol ER®) caplets. Note that both of these
products are completely released by 3 hours. The triangles represent the in
vitro
217
dissolution profile of the sustained release formulation developed in our laboratory. Note
that with this product complete release is not obtained until twelve hours.
Side-Effects: Few side effects have been reported with the use of
acetaminophen in therapeutic doses (4 grams a day or less). Reported side effects of
acetaminophen are dose dependant and unlikely, but can include skin rash, hives, itching,
bloody or cloudy urine, difficulty in urination, sudden decrease in urine output,
unexplained sore throat or fever, unusual bleeding or bruising, or unusual tiredness or
weakness (see attached United States Pharmacopeia Drug Information sheet. Other
symptoms may occur in overdose situations but are not expected during this study as the
dosage given is below the maximum daily dose of acetaminophen (4 grams per day).
Exclusions: All test participants will be healthy, normal people with no known
medical problems. Pregnant women will be excluded, even though acetaminophen is the
drug of choice for analgesia in these patients, because of the inadvisability of taking any
medication while pregnant if not absolutely necessary. Test subjects will be excluded
from this study if any of the following are true:
1. They have shown any previous hypersensitivity to acetaminophen or to
acetaminophen combination products.
2. They have renal abnormalities or known renal dysfunction.
3. They have liver abnormalities or known liver dysfunction.
4. They are currently taking any prescription or non-prescription form of
acetaminophen or acetaminophen containing product.
5. They are currently taking any medication that might effect the elimination of
acetaminophen (i.e. phenobarbital, phenytoin)
218
6.
They are or expect to become pregnant during the duration of the study.
7. Persons who have ever had hepatitis B or C, who have tested positive for HTV
or any AIDS virus, who have AIDS, or who are at risk for getting and spreading
any AIDS virus. You are at risk if:
you are a man who has had sex with another man since 1977,
even one time.
you have shared a needle, even one time, to inject drugs
or medication.
you have taken clotting factor concentrates for a bleeding
disorder such as hemophilia.
- you have ever had a positive test for any AIDS virus or
hepatitis B or C or any AIDS antibody.
you have had sex with any person described above.
- you have had sex with a male or female prostitute since
1977.
Test Subjects: Test participants will be 20 healthy, normal volunteers drawn
from the Oregon State University faculty, staff, and student population. Written consent
of each participant will be obtained after verbal and written information is presented by a
registered pharmacist.
Anonymity: All records will be kept confidential. The identity of the research
participants will not be released through either oral or written transmission to any
member not directly involved in the research group. Records from each subject shall be
retained in the project file for three years beyond the end date of the project.
219
MATERIALS AND METHODS
Materials: Acetaminophen NF/USP, lot #JE321 was obtained from Spectrum
Chemical Mfg Corp. Gardena, CA, magnesium stearate NF/USP, lot #KC502 was
obtained from Spectrum Chemical Mfg Corp. Gardena, CA,
hydroxypropylmethylcellulose (Methocel® K100M PREM CR) lot #MM92101 105K was
obtained from Dow Chemical Co. Midland, MI, and polyvinylpyrrolidone NF/USP from
Spectrum Chemical Mfg Corp. Gardena, CA. All water used was distilled de-ionized
water.
Tablets: Each tablet contains 89.0% acetaminophen, 5.O%
hydroxypropylmethylcellulose (HPMC), 5.0% polyvinylpyrrolidone (PVP), and I .0%
magnesium stearate by weight. The PVP is dissolved in 0.5ml of water per tablet. The
HPMC and the acetaminophen are premixed and then slowly added to the PVP solution.
The resulting thick paste is extruded into noodles and dried. The dried noodles can then
be broken into granules. Magnesium stearate is added to the granules and mixed to
thoroughly coat the granules. Tablets are made by placing loading granules into a single
punch tableting machine. Desired tablet weight is 730.0mg.
Subjects: Test participants are normal, healthy volunteers who are not currently
taking any prescription or non-prescription forms of acetarninophen and have previously
fasted for 2 hours or greater prior to the dose. Fasting must continue for two hours after
220
taking the dose. Subjects will not be allowed to eat or drink anything 5 minutes before
each sample.
Design: A cross-over design will be used. Subjects are randomly assigned to one
of the three formulations. After a one week wash out period, a second formulation will
be given. Finally, after a second week long wash out period, the third formulation will be
given.
Sampling: Saliva samples will be collected at times 0.0, 0.5, 1.0, 1.5, 2.0, 3.0, 4.0,
5.0, 6.0, 9.0, 12.0 and 24.0 hours. Each participant will chew a 1 inch square of
Parafilm® for 1 minute during each sample collection to initiate adequate saliva flow.
Saliva produced during the minute of chewing will then be collected for each time point
and frozen for later analysis.
Solutions:
1.
Acetaminophen standards of 0.4, 1.0, 2.0, 4.0, 6.0, 8.0, 10.0, and 16.0 tg/ml in water
will be used. All standards were made by aliquot dilution of a 1000 jg/ml stock
solution.
2.
Internal standard solution of 40 g/ml 7-beta- hydroxyethyl- theophylline.
3.
Mobile phase of 30% methanol and 70% water.
Assay: All saliva samples will be frozen prior to use (-20°c). Aliquots of saliva
will be centrifuged at 14,000 rpm for 2 minutes to pelletize particulates. One hundred
fifty d of supernatant will be then pipetted into a micro centrifuge tube. One hundred
221
fifty t1 of the internal standard (7-beta-hydroxyethyl theophyffine) will be added and the
mixture vortexed for 30 seconds.
Chromatography: Samples will be injected onto the High Pressure Liquid
Chromatograph (HPLC) using an automatic sampler (WISP 712; Waters Assoc.)
Separations of components is obtained by using a Cl 8-Reverse Phase column. The
mobile phase of 30% methanol/70% water will be delivered at a rate of 0.8m1/min (M6000A Solvent Delivery System) and samples will be monitored at 254nm with a model
440 absorbance detector. Injection volume will be set at 20 d.
Quantitation: Standard curves are run daily. Quantitation of the sample curves
is based on peak height ratios using the internal standard peak as the divisor. The
resulting calibration curve is fitted using PSI-PLOT® to a least-squared linear regression
line. The equation is then used to convert peak ratios into corresponding concentrations.
CONSENT FORM
This study is a research project conducted by the Department of Pharmaceutics,
College of Pharmacy, Oregon State University. The purpose of this study is to evaluate a
sustained release formulation of the drug acetaminophen. Acetaminophen (Tylenol®) is
a non-prescription medication that is used to treat mild pain and fever. Currently the
medication must be taken 3-4 times a day. The new formulation that you will take is
designed to release slowly over a 12 hours period.
222
Your participation will involve one (1) day per week for three (3) weeks (3 days
total with a 7 day wash out period between doses). You will be asked not to eat for at
least 2 hours prior to the study and after the dose, and to refrain from eating or drinking
for 5 minutes before each sample time. After dosing, you will be given a time sheet for
recording sample times, tubes in which to collect saliva samples, and 1 inch squares of
Paraflirn®. You must chew the square of Paraflim® for 1 minute during each sample
collection to stimulate saliva production. A total of 12 saliva samples will be collected
over the 24 hour period.
Side Effects: If you have previous taken Tylenol® or Tylenol Extra Strength®
with no untoward effects, you should not experience any difficulty with this product. On
rare occasions, people taking acetaminophen develop a rash or drowsiness. Any possible
side effects or abnormal symptoms that you experience should be reported to the study
investigator immediately.
Exclusions: You are excluded from this study if you are not a normal, healthy
adult free of known liver or kidney damage or if you are pregnant or plan to become
pregnant during the study period. You are also excluded if you have ever shown any
sensitivity to acetaminophen or acetaminophen containing products. Subjects should not
be taking any medications that might effect the elimination of acetaminophen (i.e.
phenobarbital, phenytoin, etc.)
223
Anonymity: All records will be kept confidential. The identity of the research
participants will not be released through either oral or written transmission to any
member outside of the research group.
Confidentiality: I have been informed that because this study involves articles
regulated by the FDA (Food and Drug Administration), the FDA may choose to inspect
records identifying me as a subject in this investigation.
Withdrawal: Participation in this study is voluntary, you may withdraw at any
time. There is no penalty if you withdraw from the study for any reason: exclusion,
competing commitments, drug reaction, loss of interest. No loss of benefits, standing, or
relationship with the research group or Oregon State University will result.
Questions about the research, your rights, or research related injuries should be directed
to James Ayres, Ph. D., at 737-5787, or Carol Keller at 737-5771.
I have read the consent form above and I understand the information presented. I
understand that the University does not provide a research subject with compensation or
medical treatment in the event that the subject is injured as a result of participation in the
research project. My participation is voluntary, and refusal to participate will involve no
penalty or loss or benefits to which I am otherwise entitled, and that I may discontinue
participation at any time without penalty or loss of benefits to which I am otherwise
entitled.
Signature_______________________________________ Date___________________
224
DATA SHEET
Please record the time of each sample collection to the nearest 5 minutes.
Time the dose was taken:_______________
Hours after dose
Time sample was taken
0.0
0.5
1.0
1.5
2.0
3.0
4.0
5.0
6.0
9.0
12.0
24.0
Signature:
Date:
225
SUBJECT DATA SHEET
Data for Subject:____________________ Identifier:
Formulation:
Hours after dose
Actual time
Concentration
0.0
0.5
1.0
1.5
2.0
3.0
4.0
5.0
6.0
9.0
12.0
24.0
Signature:
Date:
226
Appendix 2B:
Raw Saliva Concentration vs. Time Data for Four Test Formulations in
10 Healthy Human Subjects
227
Figure 2B.1: Raw Saliva Concentration Vs Time Data for 10 Subjects Taking
1000mg of Tylenol Extra Strength
TIME (hr)
SUBJECT 1
SUBJECT
2
SUBJECT
3
SUBJECT 4
SUBJECT 5
0.5
5.91
12.21
6.64
1.64
7.35
1.0
15.22
10.95
7.61
10.61
6.41
1.5
11.95
10.13
6.89
9.02
5.11
2.0
10.38
9.57
5.82
6.46
3.0
3.45
6.43
5.11
4.59
3.40
4.0
1.39
4.08
3.39
2.86
2.89
5.0
1.34
2.91
1.72
1.72
6.0
0.49
2.26
4.00
0.89
0.82
9.0
0.13
0.76
3.01
0.35
0.42
12.0
0.05
0.23
2.71
0.17
0.38
24.0
0.01
1.24
0.13
0.25
TIME (hr)
SUBJECT 6
SUBJECT 7
SUBJECT 8
SUBJECT 9
SUBJECT 10
0.5
15.88
16.45
7.55
16.66
1.0
11.78
14.64
6.91
14.74
1.5
9.20
11.74
6.30
13.65
2.0
7.05
11.19
4.34
12.59
7.54
3.0
5.43
7.78
2.22
10.54
6.61
4.0
4.21
3.84
2.12
8.46
4.18
5.0
3.94
3.76
1.87
7.15
3.69
6.0
2.65
1.99
1.41
5.14
3.50
9.0
2.20
1.53
0.60
3.92
1.928
12.0
1.26
0.72
0.42
2.99
1.48
24.0
0.70
0.03
0.37
1.50
0.82
11.59
Line indicates missing data points. Time zero data points were not used in the fitting
because of program constraints.
228
Figure 2B.2: Raw Saliva Concentration Vs Time Data for 10 Subjects Taking
l300mg of Tylenol Extended Relief
TIME (lit)
SUBJECT 1
SUBJECT 2
SUBJECT 3
SUBJECT 4
SUBJECT 5
0.5
1.12
8.199
8.29
1.22
10.76
1.0
8.33
10.23
9.075
13.61
9.47
1.5
14.34
14.04
7.46
2.0
10.06
11.78
4.61
15.16
6.91
3.0
8.01
9.84
3.6
8.89
4.04
4.0
6.56
8.44
2.55
7.33
2.97
5.0
4.54
7.32
1.89
4.54
2.56
6.0
3.49
5.36
1.14
2.6
1.64
9.0
0.54
3.56
0.47
1.84
0.94
12.0
0.31
0.68
0.1
1.25
0.86
24.0
0
037
0.03
1.15
0.37
TIME (hr)
SUBJECT 6
0.5
8.43
8.36
14.64
6.25
1.0
8.82
15.11
14.88
14.7
1.5
13.25
14.85
14.81
13.85
2.0
2.04
14.69
14.63
11.21
9.87
3.0
10.56
12.66
9.83
9.61
7.05
4.0
8.02
6.96
8.29
7.42
3.25
5.0
5.32
6.17
5.45
7.09
3.13
6.0
5.18
4.16
3.12
7.09
2.56
9.0
2.4
2.39
3.44
1.326
12.0
0.61
3.011
0.81
1.12
2.32
0.45
0.02
24.0
SUBJECT 7
SUBJECT 8
8.54
SUBJECT 9
SUBJECT 10
10.67
0.01
Line indicates missing data points. Time zero data points were not used in the fitting
because of program constraints.
229
Figure 2B.3: Raw Saliva Concentration Vs Time Data for 10 Subjects Taking
l300mg of the 5% HPMC Sustained Release Acetaminophen Formulation.
TIME (hr)
SUBJECT 1
0.5
1.45
1.36
0.62
0.47
1.44
1.0
3.36
2.54
1.55
1.53
2.49
1.5
4.45
3.88
2.64
2.63
2.69
2.0
5.03
5.36
2.67
3.14
2.75
3.0
5.52
7.11
5.39
7.96
6.33
4.0
6.69
9.43
5.52
10.41
5.03
5.0
4.97
5.87
3.82
11.32
2.92
6.0
4.37
4.04
3.74
6.05
2.11
9.0
3.52
3.46
3.12
3.99
0.77
12.0
3.34
2.31
2.48
1.76
0.44
24.0
1.39
1.64
2.07
1.46
TIME (hr)
SUBJECT 6
0.5
2.40
1.65
0.31
2.13
2.00
1.0
5.95
3.00
1.75
2.22
2.46
1.5
6.15
3.71
2.34
3.73
4.30
2.0
6.28
4.37
2.69
4.27
5.37
3.0
7.87
6.14
3.13
4.90
6.63
4.0
6.39
8.29
3.69
4.89
5.63
5.0
6.21
5.88
5.56
4.69
4.18
6.0
4.00
4.44
3.96
4.59
3.42
9.0
3.58
0.75
3.89
2.67
12.0
3.31
0.60
3.65
24.0
1.88
0.16
1.93
SUBJECT 2
SUBJECT 7
0.2
SUBJECT 3
SUBJECT 8
SUBJECT 4
SUBJECT 9
SUBJECT 5
SUBJECT 10
0.01
Line indicates missing data points. Time zero data points were not used in the fitting
because of program constraints.
230
Figure 2B.4: Raw Saliva Concentration Vs Time Data for 10 Subjects Taking
1300mg of the 7.5% HPMC Sustained Release Acetaminophen Formulation.
TIME (hr)
SUBJECT 1
0.5
0.74
2.43
0.81
0.13
0.83
1.0
1.02
3.32
1.12
0.22
1.21
1.5
1.23
3.56
1.17
0.34
1.60
2.0
1.60
4.02
1.30
0.53
2.94
3.0
1.82
4.08
1.45
0.76
1.39
4.0
1.33
2.78
1.61
1.53
0.88
5.0
1.30
2.50
1.64
2.66
0.84
6.0
1.26
1.94
1.65
2.03
0.65
9.0
0.69
1.85
1.75
0.86
0.61
12.0
0.51
1.0
1.60
0.00
0.60
24.0
0.40
0.46
1.24
TIME (hr)
SUBJECT 6
0.5
0.40
1.0
1.07
1.5
SUBJECT 2
SUBJECT 3
SUBJECT 4
SUBJECT 5
0.44
SUBJECT 9
SUBJECT 10
0.31
1.03
2.71
1.59
1.14
1.23
2.79
1.22
2.27
2.95
1.53
2.85
2.0
2.42
2.95
4.11
2.01
3.15
3.0
3.57
3.20
3.73
4.11
3.60
4.0
3.97
3.11
3.43
2.70
4.48
5.0
3.41
3.13
2.49
4.10
6.0
3.19
2.68
9.0
2.78
2.49
2.99
1.71
2.89
12.0
2.20
2.21
2.08
1.50
2.74
24.0
1.02
1.11
0.54
0.39
1.18
SUBJECT 7
SUBJECT 8
1.78
Line indicates missing data points. Time zero data points were not used in the fitting
because of program constraints.
231
APPENDIX 3A:
Copy of the Application to the OSU Investigational Research
Board for the Protection of Human Subjects.
232
Comparison of Immediate and Sustained Release Acetaminophen for
Symptomatic Relief of Pain in Osteoarthritis Patients
Significance: This is a phase II clinical trial of a new sustained release
formulation of acetaminophen. Phase I consisted of testing the new formulation in
healthy volunteers and has been completed. Phase II involves limited testing of the new
formulation in patients with the disease state that the drug was designed to treat. In this
case, that includes patients with osteoarthritis of the knee. Preliminary studies suggest
that the chronic pain due to osteoarthritis can be adequately relieved by this new
sustained release acetaminophen dosage form as well or better than the conventional
immediate release acetaminophen formulations.
Acetaminophen is a widely used, over-the-counter medication for analgesia and
fever. It has been available to the general public for over 30 years without a prescription.
Acetaniinophen is currently given either as an immediate release product (650-1000mg
every 4-6 hours) or as an extended release product (1 300mg every 8 hours). A new
sustained release formulation developed in our laboratory would provide 1300mg every
12 hours. The sustained release tablets are manufactured using well known procedures
and are made from Food and Drug Administration (FDA) approved ingredients.
Acetaminophen has been shown to be effective in relieving pain due to osteoarthritis,
however the current dosing interval is inconvenient for patients who require pain relief
on a chronic basis. The new 12 hour formulation would relieve pain while minimizing
the overall daily dose and maximizing convenience.
233
Patients will be enrolled in this study to compare a new long acting formulation of
acetaminophen to the original immediate release form for relief of pain in people with
osteoarthritis. Each participant will be asked to take both medications. The participants
will take one medication for four weeks, have a one week acetaminophen-free period, and
then take the other medication for four weeks. Ibuprofen tablets are provided to the
patients as a rescue analgesic. They may take 400mg of ibuprofen every 6 hours for pain
not relieved by the current treatment and during the acetaminophen-free period. The
order of the medications will be randomly assigned. One medication is the currently
available form of acetaminophen. It is taken as two 500mg tablets every six hours. The
second medication is a new long acting form that only needs to be taken every twelve
hours. Tablets that appear similar to the long acting form but contain no drug (placebos)
are provided for two additional doses. The placebo tablets allow both treatments to
appear to be identical. Neither the investigator nor the participant will know which
medication is being taken.
During the first visit, participants will be asked to answer a questionnaire that will
provide information about themselves (age, weight, height) and the pain that they have.
They will also be asked to walk 50 feet. The time it takes to walk 50 feet will be used to
help measure pain. At this first visit, participants will also receive their first packet of
medication. They will receive four identical cards of medication, one for each week.
Participants will be asked to take two tablets of the study medication four times a day.
After four weeks of the first medication, participants will be asked to return to the
clinic. The questions about pain and the time to walk 50 feet will be repeated.
Participants will be provided with the second packet of medication. Participants will be
234
asked to wait for one week and repeat the four week trial, again taking the medication
four times a day. Participants will also be asked to spit into a small tube so that the level
of drug can be measured in the body.
At the completion of the second four week period, participants will be asked to
return to the clinic for a third and last evaluation. The questions about pain and the
walking test will be repeated. Participants will be asked to spit into a small tube again to
measure the level of the drug in the body.
Justification: Currently available formulations of acetaminophen must be taken
every 6 to 8 hours to maintain adequate drug concentrations in the blood to provide pain
relief. The development of a sustained release formulation would provide extended
relief from pain while minimizing the dose, and thereby the side effects of the drug.
Twelve hour dosing intervals have also been shown to increase the compliance of
patients. This is especially important in patients who require pain relief on a long term
basis (arthritis).
Side-Effects: Few side effects have been reported with the use of acetaminophen
in therapeutic doses (4 grams a day or less). Reported side effects of acetaminophen are
dose dependant and unlikely, but can include skin rash, hives, itching, bloody or cloudy
urine, difficulty in urination, sudden decrease in urine output, unexplained sore throat or
fever, unusual bleeding or bruising, or unusual tiredness or weakness (see attached United
States Pharmacopeia Drug Information sheet. Other symptoms may occur in overdose
situations but are not expected during this study as the dosage given is below the
maximum daily dose of acetaminophen (4 grams per day).
235
Benefits: Participants may benefit from their participation in this study in that
the pain due to their osteoarthritis may be reduced or eliminated. It is also possible that
the pain will not be controlled by the use of this medication, and it will then be necessary
to take the ibuprofen provided for additional pain control.
Alternative Treatments: If participants do not choose to participate in this
study, other drugs are available for the treatment of osteoarthritis. They include nonsteroidal-anti-inflammatory medications such as ibuprofen, aspirin, naprosyn and narcotic
pain relievers such as Darvocet N-100®, Vicodin®, and Tylenol #3®.
Exclusion/Inclusion Criteria
Inclusion criteria includes:
Participants in this study should:
1. Be age 40-75, inclusive.
2. Be able to walk 50 feet without assistive devices (canes, walkers, etc.)
3. Have previously diagnosed (l-iistory> 3 months) osteoarthritis of the knee and
a history of pain due to the disease.
Exclusion criteria includes:
1. Trauma to or intra-articular injections in the affected joint(s) in the last three
months.
2. Previous history of sensitivity to acetaminophen or acetaminophen containing
products.
3. Previous history of sensitivity to ibuprofen or ibuprofen containing products.
236
4. Previous history of angina pectoris, congestive heart failure, chronic obstructive
pulmonary disease, peripheral vascular disease, fibromyalgia, bursitis,
inflammatory arthritis, or any other musculoskeletal condition that could cause
concomitant leg pain.
5. Previous history of hepatic insufficiency.
6. Previous history of renal insufficiency.
7. Patients with history of gastric ulceration or who are presently receiving
thrombolytic therapy.
8. Pregnancy.
9. Persons who have ever had hepatitis B or C, who have tested positive for HIV
or any AIDS virus, who have AIDS, or who are at risk for getting and spreading
any AIDS virus. You are at risk if:
- you are a man who has had sex with another man since 1977,
even one time.
you have shared a needle, even one time, to inject drugs
or medication.
you have taken clotting factor concentrates for a bleeding
disorder such as hemophilia.
you have ever had a positive test for any AIDS virus or
hepatitis B or C or any AIDS antibody.
- you have had sex with any person described above.
you have had sex with a male or female prostitute since
1977.
Test Subjects: Participants will be recruited from the Veterans Administration
Hospital in Portland, OR in conjunction with Dr. Theresa Bianco Pharm. D. and Dr.
Minot Cleveland M.D.. Potential patients will be identified by chart review and will be
approached regarding their participation in person.
237
Anonymity: All records will be kept confidential. The identity of the research
participants will not be released to any member not directly involved in the research
group. Each participant will be assigned a subject number and all references to
participants will be by subject number. Subjects will be advised that because the study
involves an investigational new drug, all records are subject to review by the Food and
Drug Administration. Records from each subject will be retained in the project file at the
Veterans Administration Hospital for three years beyond the end date of the project.
Consent Form: A copy of the proposed consent form is included in Appendix
A. This form is in the Veterans Administration Hospital format and is currently being
reviewed by the Investigational Research Board of that institution. Any changes required
to obtained approval at the VA institution will be reported and will be subject to
secondary approval by Oregon State University.
MATERIALS AND METHODS
Manufacture of Sustained Release Tablets:
Ingredients and Excipients: A licensed pharmacist at the pharmaceutics
laboratory at Oregon State University will undertake production of the sustained release
tablets. The following materials will be used in the production of the tablets. They
include acetarninophen NF/USP (Spectrum Chemical MFG. Corp., Gardena, CA) Lot
JE321, polyvinylpyrrolidone K-30 NF/USP (Spectrum Chemical MFG. Corp., Gardena,
CA) Lot KD186 as a tablet binder, magnesium stearate NF/USP (Spectrum Chemical
MPG. Corp., Gardena, CA) Lot KC502 as a tableting lubricant/glidant, and Methocel®
238
Ki OOM PREM CR brand of hydroxypropylmethylcellulose (Dow Chemical Co. Midland,
Mf) Lot MM92101 105K as a sustained release matrix substrate. Avicel® microcrystalline
cellulose NF/USP (FMC Corporation, Philadelphia, PA) Lot X129 is used in place of the
acetaminophen in the placebo tablets. Water used during the granulation process is
distilled and then passed through a de-ionization system.
Cleaning: All surfaces are cleaned prior to each production run. All equipment
and the surrounding area will be cleaned with Alconox®, rinsed with distilled, deionized
water, and swabbed with 95% ethanol. All surfaces will be free of soap residue or films.
The process will be attended at all times.
Manufacturing Process: Each tablet contains 89.0% acetaminophen, 5.O%
hydroxypropylmethylcellulose (HPMC), 5.0% polyvinylpyrro]idone (P\TP), and 1.0%
magnesium stearate by weight. The desired amount of PVP is dissolved in 0.75ml water
per tablet. The HPMC and the acetaminophen are premixed and slowly added to the
PVP solution. The resulting thick paste is extruded into noodles onto a flat, plastic wrap
covered surface and allowed to dry overnight at room temperature. The dried noodles
are mechanically broken up into granules using a mortar and pestle and sieved through a
succession of sieves. Granules that pass through a 14 mesh sieve but are retained on a 60
mesh sieve are used. Granules not within the prescribed range are discarded. Magnesium
stearate is then added to the granules and mixed to thoroughly coat the granules. Tablets
are made from the granules by loading the mixture into a single punch tableting machine
(Chemical and Pharmaceutical Industry Co., New York, NY, Model TPK-12). Ejected
239
tablets are 12mm in diameter with a 4mm belly band and curved faces. One face of the
tablet is scored across the middle and bears the imprint 427 OPD. Desired tablet weight
is 730mg. Each batch produced will be assigned sequential lot numbers.
Placebo tablets are made by replacing the acetaminophen in the tablets with
Avicel®. Granulation of the placebo tablets is not necessary as the Avicel® is already
granular. The four ingredients are dry mixed and loaded into the single punch tableting
machine to produce tablets that are identical to the study medication in appearance and
weight.
Labeling: Finished tablets will be stored at room temperature in amber vials until
packaging. Each vial will bear the following label:
INVESTIGATIONAL DRUG
Acetaminophen Sustained Release Tablets
650mg
Date
Lot
To help assess compliance, the treatment medications will be placed in unit dose
cards. Each card holds a single week's worth of medication. Each treatment will last 4
weeks. All four cards will be dispensed at once. The medication will be placed in REDIPAK® compliance cards and will be labeled for use.
*****************************************************************
OREGON STATE UNIVERSITY
COLLEGE OF PHARMACY
INVESTIGATIONAL ACETAMINOPHEN STUDY
PATIENT NUMBER 1
TREATMENT 1
WEEK 1
** * * * * *********** * ************* ********** ****** **** *** *
DOSE 1
DOSE 2
DOSE 3
DOSE 4
S
U
N
M
0
N
T
U
E
S
w
E
D
T
H
U
R
F
R
I
S
A
T
Patients will be randomly assigned in a crossover fashion to one of two
treatments. Each treatment involves the patient taking 2 tablets four times a day for four
weeks. After a week washout period each patient is crossed over to the second treatment.
For one treatment the dose packets will contain 2 X 500mg immediate release tablets. For
the other treatment the dose packets will contain two doses of the sustained release
formulation (Dose I and Dose 3) and two doses of placebo tablets (Dose 2 and Dose 4).
Neither the patient nor the investigator will know which treatment the patient is currently
taking.
241
Tablet Characterization: Each batch of tablets produced will be evaluated for
hardness and friability. Tablet hardness will be measured using a Strong-Cobb
hardness tester. Tablets with hardness values of less than 4kg will be considered
unacceptable and will be discarded. Friability will be tested using a Roche Friabilator.
Five tablets from each batch will be tested for 100 rotations. Tablet samples that lose
greater than 1% of their weight will be considered to be unacceptable and will be
discarded. Each tablet batch will also be weighed and an average tablet weight
recorded.
Tablet Dissolution: Six tablets from each batch will be evaluated using a USP
dissolution (Paddle Method) test. For the first two hours each tablet will be exposed to
900m1 of enzyme-free simulated gastric fluid (pH = 1.4). Samples will be taken from the
vessels with replacement at 20 minutes, 40 minutes, 1 hour, 1 hour and 20 minutes, 1
hour and 40 minutes, and 2 hours. After two hours the fluid is filtered through No. 1
filter paper and the particles retained. The particles and the filter paper will then be
exposed to 900m1 of enzyme-free simulated intestinal fluid (pH = 7.4) for the remaining
22 hour period. Samples will be taken with replacement at 3 hours, 4 hours, 6 hours, 9
hours, 12 hours, and 24 hours. Samples will be diluted 1:100 with distilled, deionized
water and analyzed at 244nm in a Hewlett Packard variable wavelength UV-VIS
spectrophotometer equipped with a sipper cell. Standard solutions of acetaminophen in
distilled, deionized water will be used to correlate absorbance to concentration. Previous
experience has indicated that interference from polymers and or other excipients that may
be present in the dissolution medium is negligible.
242
Dissolution will also be performed on the commercial acetaminophen products
for comparison purposes. By design, the immediate release commercial formulation
should rapidly dissolve in the gastric fluid. Samples will therefore be taken in gastric fluid
only, unless dissolution is incomplete in the first two hours. Samples will be taken with
replacement at 5 minutes, 10 minutes, 15 minutes, 20 minutes, 25 minutes, 30 minutes, 40
minutes 60 minutes, 75 minutes, 90 minutes, 105 minutes and 120 minutes.
Procedure: After signed consent is obtained and inclusion/exclusion criteria are
met, patients will undergo an initial evaluation. A history and disease characterization will
be performed including height, weight, and age. An initial evaluation of the type and
duration of pain in the patient will be assessed using modified Stanford Health
Assessment Questionnaire (1-[AQ) pain scores (Appendix B) and time to walk 50 feet.
Enrolled patients will be randomly assigned to one of two groups. Each group
will be asked to take two tablets four times a day. Group I will take two 500mg
acetaminophen tablets four times a day. Group 2 will take two 65Omg sustained release
tablets twice a day alternating with 2 identical placebo tablets for the remaining two doses
per day. Doses will be unit dosed to help assess compliance. Patients will be asked to
continue the dosing regimen for four weeks. Compliance will be assessed by tablet count.
Ibuprofen 200mg tablets will be provided to patients as a rescue analgesic. Patients will
be asked to record their usage of the rescue analgesic. A maximum of 400mg of
ibuprofen may be taken every 6 hours. At the end of the four week study period, patients
will be asked to repeat the initial evaluation of their pain. Patients will also be asked to
provide a saliva sample at the time of reassessment just prior to the final dose of the
243
medication to assess compliance and to evaluate the relationship of saliva acetaminophen
concentrations to pain control. After a 7 day washout period, patients will be crossed
over to the second treatment. After a 4 week period, the patients will return for a third
and final evaluation.
Laboratory analysis: Saliva samples will be collected in I Omi plastic sample
tubes and immediately frozen at 4°C until analysis. Samples are then thawed, centrifuged
at 3000 rpm for 10 minutes, and the supernatant refrozen. Samples are re-thawed, recentrifuged, and 1 5O.il of the supernatant is transferred to a microcentrifuge tube. A
I 50d aliquot of 7-beta-hydroxyethyl-theophylline is then added as an internal standard.
The samples are centrifuged a third time and transferred to imi high pressure liquid
chromatography (HPLC) tubes for analysis. Samples will be run in duplicate to verify
acetaminophen concentrations.
Data Analysis: Data collected on pain control will be analyzed using analysis of
variance. Data will be analyzed as a randomized block design with factors included in the
model for treatment order and carryover effects. Correlation between saliva
acetaminophen concentrations and pain control will also be analyzed using an analysis of
variance.
244
Initial Demographic Information
Visit 1
To be administered by the Investigator
Name
Age
Height
Weight
lbs.
kg.
How long have you been diagnosed with osteoarthritis?
Which joint(s) are affected by the osteoarthritis?
Do you usually have pain associated with your illness?___________________
What medication do you normally take to relieve this pain?
Does this product adequately relieve your pain?
Have you taken Tylenol® or Tylenol® containing products in the
last 7 days?
245
Have you ever had any problems or side effects while taking Tylenol® or
Tylenol® containing products? YES
NO
If so, what?
Have you ever had any problems or side effects while taking Advil®, Motrin®, or
ibuprofen containing products? YES NO
If so, what?
What medications have you taken in the past for your
osteoarthritis?
What prescription medications do you currently take?____________________
What non-prescription medication do you take. Include vitamin
preparations.
246
Inclusion/Exclusion Criteria
Do you have a history of:
1. Trauma to the affected joint in the last 3 months
YES NO
2. Corticosteroid injections in the last 3 months
YES NO
3. Angina
YES NO
4. Congestive Heart Failure
YES NO
5. Chronic Obstructive Pulmonary Disease
YES NO
6. Peripheral Vascular Disease
YES NO
7. Fibromyalgia
YES NO
8. Bursitis
YES NO
9. Rheumatoid Arthritis
YES NO
10. Kidney Problems
YES NO
11. Ulcers
YES NO
Pain Evaluation Visit
2
1
3
Subject
Treatment
How would you rate your overall pain during the last 4 weeks?
1
mild
2
mod
3
severe
How would you describe the change in your pain in the last 4 weeks?
1
better
2
no change
3
worse
My pain is best described as:
1
periodic
2
3
daily
constant
247
I need help from another person to do the following things:
Seldom
Sometimes
Often
Dress
1
2
3
Eat
1
2
3
Standup
1
2
3
Walk
1
2
3
Climb stairs
1
2
3
Clean House
1
2
3
The pain medication that I have been taking for the last 4 weeks relieves my pain Seldom
Sometimes
2
1
Often
3
The pain relief lasts for the entire time between doses
Seldom
1
Sometimes
2
Often
3
List any side effects or problems with the medication that you have been taking
for the last 4
Time to walk 50 feet____________________________________________
248
Other Approvals:
1. Investigation New Drug Application was filed December 5, 1995. Approval is
pending. The review and approval process is being hindered by the governmental
shutdown. Unspecified changes have been requested. Details are expected Jan 15, 1996.
2. Investigational Review Board Application with the Veterans Administration Hospital
was filed Dec 23, 1995. Approval is pending. Review is scheduled for the first Wed of
January, but may also be effected by the governmental shutdown.
249
APPENDIX 3B:
Copy of the Investigation Review Board application to the Veterans
Administration Hospital Human Studies Committees
250
Purpose: You have been asked to participate in a research study to determine if a
new long acting formulation of acetaminophen (Tylenol®) can control your osteoarthritis
(joint) pain. You have been asked to participate in this study because you have been
diagnosed with osteoarthritis and have had pain because of this disease. Acetaminophen
has been previously shown to be effective in treating pain due to osteoarthritis but it has
to be taken four times a day. A new longer acting form of the drug would allow it to be
taken only two times a day. This study is important because it will help evaluate new
form of the drug and how well it works. This study will last for 10 weeks and will require
three 1-hour visits.
Procedures: If you agree to participate in this study, we will contact your doctor
to obtain permission. Once permission from your doctor is obtained, you will be asked
to stop taking your usual pain medication for the duration of this study. One week after
stopping your usual pain medication, you will come to the clinics at the Veterans
Administration Hospital. Ibuprofen tablets (200mg) will be provided for pain during this
time. You will be asked to keep track of how many ibuprofen tablets that you use. A
maximum of two ibuprofen tablets three times a day will be allowed. You will be asked
not to take the ibuprofen for 12 hours before each visit.
At the first visit, you will be asked to complete a questionnaire about yourself and
the type of pain that you have. In addition, you will be asked to walk 50 feet to evaluate
how well you can move. You will then be given a study medication packet. For four
weeks, you will be asked to take 2 tablets of your study medication four times a day. You
will be taking either two short-acting acetaminophen tablets (500mg each) four times a
251
day, or two long acting acetaminophen tablets (650mg each) alternating with two
placebo tablets. A placebo is a tablet that contains no active drug. Neither you nor the
investigators will know which study medication you receive. Ibuprofen tablets (200mg)
will be provided for pain not relieved by the study medication. You will be asked to keep
track of how many ibuprofen tablets that you use. A maximum of two ibuprofen tablets
three times a day will be allowed. After the four week period you will be asked to return to
the center and repeat the questionnaire and walking test. In addition, you will be asked to
provide a saliva sample. The saliva samples will tell us how much medication is in the blood
without having to actually draw blood. At this visit, you will be provided with the other type
of medication to take for a second four week period. You must wait a week for the effects
of the first medication to wear off before you begin taking the second medication.
Ibuprofen will be provided for pain relief during the week between medications. Again, at
the end of the four week period you will be asked to repeat the questionnaire and walking
test.
Expected Discomfort or Inconvenience:Care has been taken to make this study
as easy as possible for you. However, you will be expected to make three total visits to
the clinic to pick up your study medication and to fill out your questionnaires. The visits
may represent an inconvenience to some people. In addition, the walking test may cause
some discomfort in those people who are not use to walking that distance. The
discomfort will be short-lived and we expect any discomfort to be relieved by the
medication that is provided.
252
Risks and Discomforts: There may be adverse reactions involved in participating
in this study. The most common reaction is sleepiness. Very rarely, acetaminophen can
result in a rash or hives. This means that you are allergic to the medication. You should
stop taking the medication and immediately inform one of the study investigators. Your
symptoms will be treated and the study will be stopped. Acetaminophen can cause liver
problems, nausea, vomiting, and kidney problems. The doses in this study are much less
than the doses that cause these problems, but if nausea or vomiting develop, you may be
unusually sensitive to the medication and the study will be stopped.
The most common side effect of the ibuprofen is stomach upset. It can also cause a
rash or hives. This means that you are allergic to the medication. You should stop taking
the medication and immediately inform one of the study investigators. Ibuprofen can also
cause ulcers, bleeding problems, and kidney problems, especially if taken in doses higher
than recommended. The risk of adverse reactions with either acetaminophen or ibuprofen
is increased by the use of alcohol.
Benefits: You may benefit from your participation in this study in that the pain
due to your osteoarthritis may be reduced or eliminated. It is also possible that your pain
will not be controlled by the use of this medication, and it will then be necessary to take
the ibuprofen that has been provided for additional pain control.
Alternative Treatments: If you do not choose to participate in this study, other
drugs are available for the treatment of osteoarthritis. They include non-steroidal-anti-
253
inflammatory medication like ibuprofen, aspirin, naproxen, and narcotic pain relievers
such as Vicodin® and Tylenol #3®.
Exclusions: You should not participate in this study if you have shown previous
side effects from Tylenol® or other acetaminophen containing combinations. You should
not participate in this study if you have shown previous side effects to Motrin®, Advil®,
or other forms of ibuprofen. You should not participate in this study if you have had
recent (last 3 months) trauma to the affected joint or injections into the joint. Pregnant
women will not be allowed to participate in this study. Although the medication will not
harm the child, it is not a good idea to be taking any unneeded medication if you are
pregnant. You should be able to walk 50 feet without assistance or assistive devices
(canes, walkers, etc.) You should not take the study medication if you have liver or kidney
disease. You should not participate in this study if you have had an active ulcer in the last
12 months or if you consume greater than 2 alcohol containing beverages per day. You
will not be allowed to participate if you have a documented history of alcoholism because
you are at increased risk for adverse side effects.
Withdrawal from the Study: Your participation in this study is voluntary, and
you may withdraw from this study at any time without prejudice to yourself or to any
future medical care with this institution or with the Department of Veterans Affairs(VA).
You may be removed from the study without your consent if your doctor decides
that this is in your best interest, or if you fail to follow the study schedule (such as not taking
254
your assigned medication).
Follow-up visits may still be recommended after your
withdrawal.
Costs and Compensation: The investigators will pay any medication costs
involved in this study. You will not be charged for your participation in this study. Your
participation in this study is free of charge. You will receive no money for participating in
this study.
Liability: Every reasonable effort to prevent any injury that could result from this
study will be taken. In the event of physical injury resulting from the study, medical care
and treatment will be available at this institution. For eligible veterans, compensation
damages may be payable under 38 Usc 251 or, in some circumstances, under Federal
Tort Claims Act. For non-eligible veterans and non-veterans, compensation would be
limited to situations where negligence occurred and would be controlled by the
provisions of the Federal Tort Claims Act.
For clarification of these laws, contact
District Counsel at (503)326-2441. You have not waived any legal rights or released the
hospital or its agents from liability for negligence by signing this form.
Any patient participating in a
study
at the Department of Veterans Affairs Medical
Center, Portland Oregon is encouraged to contact Dr. Dennis Mazur, Chairman,
Subcommittee on Human Subjects, to discuss any issues related to their research
participation.
extension 6620.
Dr. Mazur can be reached through the Research Service (503) 220-8262
255
Your signature below indicates that you understand that the Department of
Veterans Affairs Medical Center, your investigators, and the sponsors of this research study
bear no responsibility for any costs you may incur at other hospitals, clinics, or care
institutions related to this study or to any of your medical conditions.
Signature:
Date:
Confidentiality: The results of your participation in this study may be used for
publication or for scientific purposes, but your identity will not be disclosed unless you
give separate, specific consent to this, or unless required by law. I have been informed
that because this study involves articles regulated by the FDA (Food and Drug
Administration), the FDA may choose to inspect records identifying me as a subject in
this investigation.
Other: Registered Pharmacists Theresa Bianco, Pharm. D. (273-5398), and Carol
Keller, R. Ph. (737-7776) have offered to answer any questions that you may have.You
will receive a copy of this consent form. Your signature below indicates that you have
read the foregoing and agree to participate in the study.
256
OREGON STATE UNIVERSITY
INVESTIGATIONAL ACETAMINOPHEN PROTOCOL SUMMARY
Objective: The specific aim of this study is to compare the effectiveness of a new
sustained release formulation of acetaminophen with currently available acetaminophen
products for the relief of pain due to osteoarthritis.
Research Plan: This study is a randomized, double blind, placebo controlled
cross-over study. The study population will consist of patients with previously diagnosed
osteoarthritis of the knee.
Methodology: After signed consent is obtained and inclusion/exclusion criteria are
met, patients will undergo an initial evaluation. A history and disease characterization will be
performed including height, weight, and age. An initial evaluation of the type and duration
of pain in the patient will be assessed after a one week washout period using modified
Stanford Health Assessment Questionnaire (HAQ) pain scores and time to walk 50 feet.
Enrolled patients will be randomly assigned to one of two groups. Each group will be asked
to take two tablets four times a day. Group I will take two 500mg acetaminophen tablets
four times a day. Group 2 will take two 650mg sustained release tablets twice a day with 2
identical placebo tablets for the remaining two doses. Doses will be individually packaged to
help assess compliance. Patients will be asked to continue the dosing regimen for four
weeks.
Compliance will be assessed by tablet count. Ibuprofen 200mg tablets will be
provided to patients as a rescue analgesic. Patients will be asked to record their usage of the
rescue analgesic. A maximum of 400mg of ibuprofen two times a day may be taken. At the
257
end of the four week study period, patients will be asked to repeat the initial evaluation of
their pain. Patients will also be asked to provide a saliva sample at the time of reassessment
just prior to the final dose of the medication to assess compliance and to evaluate the
relationship of saliva acetaminophen concentrations to pain control. After a 7 day washout
period, patients will then be crossed over to the other treatment for an additional 4 weeks.
Reassessment will be repeated after the second four-week period.
Laboratory Analysis: Saliva samples will be collected in 4m1 plastic sample tubes
and immediately frozen at 4°c until analysis. Samples are then thawed, centrifuged at 3000
rpm for 10 minutes, and the supernatant refrozen. Samples are re-thawed, re-centrifuged,
and 1501d of the supernatant is transferred to a microcentrifuge tube. A l50d aliquot of 7beta-hydroxyethyl-theophylline 4Oug/ml is added as an internal standard. Samples will be
analyzed in duplicate
using high pressure liquid
acetaminophen concentrations.
Results to Date: None.
chromatography to determine
258
EVALUATION OF A CONTROLLED RELEASE ACETAMINOPHEN
TABLET FOR ANALGESIA IN OSTEOARTHRITIS PATIENTS
A PILOT STUDY
Principal Investigators
Theresa M. Bianco, Pharm. D.
Carol A. Keller, R. Ph.
Introduction: An estimated 40.5 million adults in the United States suffer from
some form of osteoarthritis (OA)1. With a steadily aging population, that number is
expected to increase in the coming years. The disease is age associated and the
prevalence ranges from 4% in people age 18-24 years old to 85% in patients 75-79 years
old.1'2
The incidence of OA is higher in women and in some racial
types.1'3
The specific
aim of this study is to assess the effectiveness of a novel sustained release formulation of
acetaminophen in relieving pain in these patients.
The symptoms of osteoarthritis vary with the duration of the disease and the
number of joints that are involved. The predominant symptom is a localized deep,
aching pain in the affected joint(s). Early in the course of the disease, the pain is present
when the affected joint is first used and is relieved when the joint is at rest or when
weight is removed from the joint. As the disease progresses, the pain can become present
with minimal movement and at rest. In addition to pain, patients may experience loss of
range-of-motion (ROM), stiffness, and physical deformities.1
No cure exists for OA. Treatment is aimed at reducing pain, maintaining
mobility, and minimizing disability.4 Historically, OA has been treated much like
rheumatoid arthritis, with non-steroidal-anti-inflammatory medications
(NSAIDS).57
Although effective, these medications present several problems in the elderly population
with OA. The NSAIDS cause significant gastric distress and ulceration, increase
259
prothrombin time, and have uricosuric activity.5 Recently, it has been shown that since
OA does not involve an inflammatory component, that pure analgesic medication, such
as acetaminophen, are equally effective as NSAIDS in the relief of the pain and stiffness
these patients experience without some of the side
effects.5'812
Acetaminophen has been safely used for over 30 years as an over-the-counter
analgesic. In therapeutic doses of less than 4 grams per day, it does not cause gastric
distress, changes in prothrombin times, or uricosuric activity. The major problem with
using acetaminophen for chronic pain relief has been the fact that traditional immediate
release formulation must be taken every 4-6 hours to maintain analgesic effect. The
immediate release preparations do not provide lasting relief for these patients and the
potential exists for patients to take excessive doses in an effort to maintain analgesia for a
longer period of time. Chronic ingestion of greater then 4 grams per day primarily
manifests as hepatic necrosis that is characterized by nausea, vomiting, and abdominal
pain that can progress to methemoglobinemia, vascular collapse, hepatic coma and death
if left untreated.1'1316 In addition, chronic abuse can also result in renal papillary necrosis
and interstitial nephritis. Oliguria, hematuria, and renal insufficiency can result if left
untreated.13'16'17
There is a great need for a longer lasting product that would maintain
sufficient blood levels of the drug for analgesia, while minimizing the overall daily dose
and maximizing convenience to the patient. Studies have shown the efficacy of
immediate release acetaniinophen in osteoarthritis
patients.1820'11
This study was designed
to evaluate a novel sustained release formulation of acetaminophen for chronic pain relief
in osteoarthritis patients.
260
Results to Date: Preliminary pharmacokinetic calculations were performed using
published parameters.21 The pharmacokinetics goal is to maintain Cp> 5.Omg/L for the
full 12 hours. Initial in vitro evaluation of the drug product were completed and release
factors were optimized. Pharmacokinetic
in vivo
evaluation is currently underway and the
release characteristics of the formulation will be finalized based on the correlation
developed between the in vitro and in
vivo
results.
Initial formulation studies in human subjects were conducted at Oregon State
University. Ten healthy volunteers were given four acetaminophen formulations in a
single dose study. The four formulation consisted of Tylenol Extra strength tablets
(2x500mg), Tylenol Extended Release tablets (2x650mg), and two sustained release
formulations containing 7.5 and 5.0% of the controffing matrix (2x650mg). The four
formulations were administered in a four way crossover fashion with at least 7 days
separating each single dose study. Subjects were asked to fast overnight before taking the
dose and refrain from eating for two hours after the dose. Saliva samples were collected
in 4m1 plastic test tubes at 0.5, 1.0,1.5, 2.0, 3.0, 4.0, 5.0, 6.0, 9.0, 12.0, and 24.0 hours after
the dose. To collect each sample, subjects were asked to chew an one inch square of
Parafilm to stimulate saliva and to collect all saliva produced in a one minute period of
chewing. Collected saliva samples were frozen and stored until analysis.
Samples were analyzed using high pressure liquid chromatography. Samples were
centrifuged at 3,000 rpm for 20 minutes and the supernatant decanted to remove
extraneous proteins. The supernatant was refrozen for at least 24 hours after being
decanted. Samples were then re-thawed and re-centrifuged at 3.000 rpm for 15 minutes
prior to final sample preparation. An sample aliquot of l5Oiil in mixed with a l50fl
261
aliquot of 7-beta-hydroxyethyl theophyffine vortexed to ensure mixing. The 7-beta
hydroxyethyl theophy]]ine solution (4Otg/ml) is added as an internal standard. External
standard solutions of acetaminophen ranging from 0.4-1 6m/mi were run with each set
of samples. Absorbance was monitored at 254nm, the mobile phase consisted of 20:80
MeQH/water solution infused at 0.8m1/min.
Data was analyzed using peak height ratios between the acetaminophen and the 7beta hydroxyethyl theophyl]ine. The enclosed graph is the average saliva concentrations
in the 10 subjects over twenty four hours for the four formulations. The graph
demonstrates by twelve hour after the dose, both the Tylenol Extra Strength and the
Tylenol Extended Release have decayed to a level of about lmg/L in the saliva. In
contrast, the 5% sustained release formulation still maintains a saliva concentration of
about 2.5mg/L. The 7.5% sustained release formulation was eliminated because of low
bioavailibility. Upon multiple dosing, the 5% sustained release tablets appear to meet the
5mg/L target saliva concentration.
Research Design:
Goal: To evaluate the effectiveness of a novel sustained release preparation of
acetaminophen in the relief of pain in osteoarthritis patients.
Study Design: This is a randomized, double blind, placebo controlled study in a
crossover design.
Subject Recruitment: Subjects will be recruited from the outpatient clinics.
Patients who meet preliminary criteria will be approached concerning their interest in
262
participating in the study. If interested, permission of the primary care physician will be
obtained before informed consent is signed.
Inclusion criteria: Patients with chronic mechanical-type knee pain and
previous diagnosis of osteoarthritis of the knee. Age is 40-75 years inclusive. Lack of
trauma to the affected joint(s) or intra-articular corticosteroid injections in the last three
months.
Exclusion criteria: Previous history of sensitivity to acetaminophen or
acetaminophen containing products. Previous history of sensitivity to ibuprofen. History
of trauma or intra-articular corticosteroid injections in the affected joint(s) in the last 3
months. Patients with any other medical condition which would limit ability to walk 50
feet including but not limited to, angina pectoris, congestive heart failure, chronic
obstructive pulmonary disease, peripheral vascular disease, fibromyalgia, bursitis,
inflammatory arthritis, or other musculoskeletal conditions of the leg which could cause
concomitant leg pain. Patients must be able to walk 50 feet without assistance or assistive
devices. Patients with liver disease, renal insufficiencies, gastric ulceration, or any medical
condition in which non-steroidal anti-inflammatory medications would be contraindicated
will also be excluded from this study. Patients who have previously not responded to
acetaminophen therapy will also be excluded. Pregnant women will not be allowed to
participate in the study. Pregnancy testing on the study population will be done on all
women of child bearing age who do not have documented history of hysterectomy,
sterility, or menopause. Patient with a documented history of alcoholism or who
consume greater than two alcohol containing beverages per day will also be excluded.
263
Sample Size Justification: Sample size calculations were performed using data
published by Bradley et a111. Bradley compared two treatments for osteoarthritis in a
parallel design using a modified HAQ test and time to walk 50 feet. Using his published
data, within-subject estimates of treatment differences and standard deviations were
calculated. After adjusting for the crossover design and setting c' = 0.1 and power = 80%
a sample size of 40 was calculated.
Methods and Procedures: After signed consent is obtained and
inclusion/exclusion criteria are met, patients will undergo an initial evaluation. A history
and disease characterization will be performed including height, weight, and age. Patients
will be asked to stop their current analgesic medication one week prior to the initial
evaluation. Ibuprofen 200mg tablets will be provided to patients throughout the study as
a rescue analgesic. Patients will be asked to record their usage of the rescue analgesic and
to refrain from taking the ibuprofen for 12 hours prior to each walking test. A maximum
of 400mg of ibuprofen may be taken three times a day. An initial evaluation of the type
and duration of pain in the patient will be assessed using modified Stanford Health
Assessment Questionnaire (HAQ) pain scores (Appendix A) and time to walk 50 feet.
Enrolled patients will randomly assigned to one of two groups. Each group will
be asked to take two tablets four times a day. Group I will take two 500mg
acetarninophen tablets four times a day. Group 2 will take two 650mg sustained release
tablets twice a day alternating with 2 identical placebo tablets for the remaining two doses
per day. The tablets will be packaged in unit of use bubble packing to assist patients in
taking the appropriate formulation and to help assess compliance. Patients will be asked
to continue the dosing regimen for four weeks. Compliance will be assessed by tablet
264
count. At the end of the four week study period, patients will be asked to repeat the
initial evaluation of their pain. Patients will also be asked to provide a saliva sample at the
time of reassessment just prior to the final dose of the medication to assess compliance
and to evaluate the relationship of saliva acetaminophen concentrations to pain
control.21'23
After a 7 day washout period, patients will be crossed over to the second
treatment. After a 4 week period, the patients will return for a third and final evaluation.
Laboratory analysis: Saliva samples will be collected in 4m1 plastic sample tubes
and immediately frozen at 4°C until analysis. Samples are then thawed, centrifuged at
3000 rpm for 10 minutes, and the supernatant refrozen. Samples are re-thawed, recentrifuged, and 1 50d of the supernatant is transferred to a microcentrifuge tube. A
1 501al aliquot of 7-beta-hydroxyethyl-theophyffine is then added as an internal standard.
The samples are centrifuged a third time and transferred to Imi high pressure liquid
chromatography (HPLC) tubes for analysis. Samples will be run in duplicate to verify
acetaminophen concentrations.
Data Analysis: Data collected on pain control will be analyzed using analysis of
variance. Data will be analyzed as a randomized block design with factors included in the
model for treatment order and carryover effects. Other factors will be included in the
model if found to be significant (i.e. age, sex, use of breakthrough analgesic). Correlation
between saliva acetaminophen concentrations and pain control will also be analyzed using
an analysis of variance.
265
Initial Demographic Information
Visit 1
To be administered by the Investigator
Name
Age
Sex
Height
Weight
lbs.
kg.
How long have you been diagnosed with osteoarthritis?
Which joint(s) are affected by the osteoarthritis?
Do you usually have pain associated with your illness?
What medication do you normally take to relieve this pain?
Does this product adequately relieve your pain?
Have you taken Tylenol® or Tylenol® containing products (as shown in the
attached list) in the last 7 days?
Have you ever had any problems or side effects while taking Tylenol® or
Tylenol® containing products? YES
NO
266
If so, what?
Have you ever had any problems or side effects while taking Advil®, Motrin®,
Nuprin®, or ibuprofen containing products? YES NO
If so, what?
What medications have you taken in the past for your
osteoarthritis?
What prescription medications do you currently take?_____________________
What nonprescription medication do you take. Include vitamin
preparations.
Inclusion/Exclusion Criteria
Do you have a history of:
1. Trauma to the affected joint in the last 3 months
YES NO
2. Corticosteroid injections in the last 3 months
YES NO
3. Angina
YES NO
267
4. Congestive Heart Failure
YES NO
5. Chronic Obstructive Pulmonary Disease
YES NO
6. Peripheral Vascular Disease
YES NO
7. Fibromyalgia
YES NO
8. Bursitis
YES NO
9. Rheumatoid Arthritis
YES NO
10. Kidney Problems
YES NO
11. Ulcers
YES NO
12. Alcoholism
YES NO
13. How often do you drink alcoholic
beverages?
268
Pain Evaluation Visit
Subject
Treatment
2
1
3
How would you rate your overall pain during the last 4 weeks?
2
1
mild
3
mod
severe
How would you describe the change in your pain in the last 4 weeks?
1
2
better
no change
3
worse
My pain is best described as:
1
periodic
2
3
daily
constant
I need help from another person to do the following things:
Seldom
Sometimes
Often
Dress
1
2
3
Eat
1
2
3
StandUp
1
2
3
Walk
1
2
3
Climb stairs
1
2
3
Clean House
1
2
3
The pain medication that I have been taking for the last 4 weeks relieves my pain Seldom Sometimes
Often
2
1
3
The pain relief lasts for the entire time between doses
Seldom
1
Sometimes
Often
2
3
269
List any side effects or problems with the medication that you have been taking
for the last 4 weeks.
Time to walk 50 feet________________________________________________
270
References:
1.
DiPiro, J.T., Talbert, R.L., Hayes P. E., et. al.: Pharmacotherapy: A
Pathophysiologic Approach, Chapters 32 and 61. New York, New York. Elsevier
Science Publishing Co. 1989.
2.
Felson, D. T., Naimark A. , Anderson, J., et.al.: The Prevalence of Knee
steoarthritis in the Elderly: The Framingham Osteoarthritis Study. Arthritis and
Rheumatism, Vol. 30, No. 8 (August 1987). pg. 914-918.
3.
Felson, D. T.: Osteoarthritis. Epidemiology of Rheumatic Disease. Vol. 16, No. 3,
August 1990. pg. 499-510.
4.
Wilson, J. D., Braunwald, E., Isdselbacher, K. J., et. al.: Harrison's Principles of
Internal Medicine 12th Ed. Chap. 281. New York, New York. McGraw-Hill Inc.
1991.
5.
Baker, J. R. and Brandt, K. D.: Reappraisal of the Management of Patients with
Osteoarthritis. Informational handout distributed by McNeil Consumer Products
Co.
6.
Pinals, Robert S. Pharmacologic Treatment of Osteoarthritis. Clinical
Therapeutics. Vol. 14, No. 3, 1992. pg. 336-46.
7.
Arfag, Abdulrhman A. and Davis, Paul: Osteoarthritis 1991: Current Drug
Treatment Regimens. Drugs. Vol.41, No. 2, 1991. pg 193-201.
8.
Calm, Andrei: Pain and Inflammation. The American Journal of Medicine.
September 10, 1984. pg 9-15.
9.
Brandt, Kenneth D. and Bradley, John D.: Simple Analgesics versus NSAIDS for
Osteoarthritis. The Lancet. Vol. 341, March 20, 1993. pg 770-1.
10.
Amidio, P. and Cummings, D.M.: Evaluation of Acetaminophen in the
Management of Osteoarthritis of the Knee. Current Therapeutic Research. Vol.
34, No. 1,July, 1983. pg 59-66.
11.
Bradley, John D., et. al.: Comparison of an Antiinflammatory Dose of Ibuprofen,
an Analgesic Dose of Ibuprofen, and Acetaminophen in the Treatment of Patients
with Osteoarthritis of the Knee. The New England Journal of Medicine. Vol. 325,
No. 2, July 11, 1991. pg 87-91.
12.
Amadio, P.: Orally Acting Analgesics. The American Journal of Medicine.
September 10, 1984. pg 17-24.
Handbook of Drug Therapy in Liver and Kidney Disease, Chap. 3, Analgesics and
Sedative-Hypnotics. Edited by Schrier, R> W. and Gambertoglio, J. G. pg. 51.
13.
271
14.
Drug Information, 1990, Section 28:08.92 Miscellaneous Analgesics and
Antipyretics. pg. 1104-1109.
15.
Goodman and Gilman's The Pharmacologic Basis of Therapeutics, 8th edition,
Chap. 26 Analgesic-Antipyretics and Antiinflammatory Agents. pg 656-59.
16.
Handbook of Nonprescription Drugs, 9th edition. pg 71.
17.
Walker, Robert J.: Paracetamol, nonsteroidal Anti-inflammatory drugs, and
nephrotoxicity. North Carolina Medicine Journal. May 8, 1991. Leading Article.
18.
Nielsen,j.c., Bjerring, P., Arendt-Nielsen, L., and Petterson, K.J.: Analgesic efficacy
of immediate and sustained release paracetamol and plasma concentration of
paracetamol. Double-blind, placebo controlled evaluation using painful laser
stimulation. Eur. J. Clin Pharmacol (1 992)42:261-264.
19.
Strom, C., Forsberg, 0., Quidind, H., et.al.:Analgesic efficacy of acetaminophen
sustained release. J Clin Pharmacol 1990;30:654-659.
20.
Nielsen, J. C., Bjerring, P., Arendt-Nielsen, L.:A comparison of the hypoanalgesic
effect of paracetamol in slow release and plain tablets on laser-induced pain. Br J
Clinical Pharmac (1991):30:267-270.
21.
Hossain, Mohammad and Ayres, James:Pharmacokinetic and pharmacodynamics in
the design of controlled-release beads with acetaminophen as a model drug. J
Pharm Sci. Vol. 81, No. 5, May 1992:444-448.
22.
Fries, James F., Spitz, Patricia W., and Young, Donald Y.:The Dimensions of
Health Outcomes:The Health Assessment Questionnaire, Disability and Pain
Scales.J Rheum.
9:5,1982:789-793.
23.
Smith, M., Whitehead, E., O'Sullivan, G., and Reynolds, F.:A comparison of serum
and saliva paracetamol concentrations. BrJ Clin Pharmacol 1991,31:553-555.
272
APPENDIX 3C:
Copy of IND Sent to the FDA
273
December 5, 1995
Food and Drug Administration
Center for Drug Evaluation and Research
Central Document Room
5600 Fishers Lane, HFD-120
Rockville, Maryland 20852
Dear Madam/Sir,
I have enclosed three copies of an Investigational New Drug Application seeking
permission to administer acetaminophen to consenting adult, human volunteers using a
sustained release oral tablet. This will be a Phase II study conducted at Veterans Hospital
in Portland, Oregon. The Investigator for this project is Carol Keller R. Ph. The
Sponsor of this project is Dr. James Ayres. The mailing address for both the Investigator
and the Sponsor is:
Dr. James Ayres
Pharmacy Bld. 231
Oregon State University
Corvallis, OR 97331-3507
Phone:(503) 737-5787
FAX: (503) 737-3999
e-mail: ayresj@ccmail.orst.edu
Enclosed with this packet is a copy of the Certificates of Analysis for each of the
components used in the manufacture of the sustained release tablets. All chemicals used
are National Formulary/United States Pharmacopeia grade.
Also enclosed is a copy of the proposed Investigational Research Proposal from the
Veterans Hospital and the approved copy of the Investigational Research Proposal from
Oregon State University.
Thank you for your assistance.
Sincerely,
James Ayres, Ph. D., R. Ph.
Professor of Biopharmaceutics and Pharmacokinetics
Oregon State University
274
Table Of Contents
Cover Letter
Form 1571
Form 1572
1571.1 Description of Acetaminophen
1571.2 Chemical Manufacturer
1571.3 Description of Facilities
Oregon State University Pharmaceutics Manufacturing Lab
Veterans Administration Hospital
1571.4 Manufacture of Sustained Release Dosage Form
Ingredients and Excipients
Manufacturing Process
In Vitro Characterization of release of Acetaminophen
from Dosage Form
1571.5 Investigational Research Board Protocol Approved by
Oregon State University
Approval Letter
Study Protocol
In Vivo Results
1571.6 Proposed Research Protocol for the Veterans
Administration Hospital
Informed Consent
Study Protocol
1571.8 Certificates of Analysis
1571.1
275
Description of Acetaminophen
Acetaminophen: N-(4-hydroxyphenyl)acetamide
4'-hydroxyacetanilide
p-hydroxyacetanilide
p-acetamidophenol
p-acetaminophenol
p-acetylaminophenol
N-acetyl-p-aminophenol
paracetamol
Abensanil®
Doliprane®
Acamol®
Doiprone®
Acetalgin®
Dymadon®
Alpiny®
Enelfa®
Amadil®
Eneril®
Anaflon®
Eu-Med®
Anhiba®
Exdol®
Apamide®
Febrilix®
APAP®
Finimal®
Ben-u-ron®
Gelocatil®
Bickie-mol®
Hedox®
Calpol®
Homoolan®
Captin®
Korum®
Cetadol®
Lyteca®
Dafalgan®
Momentum®
Datril®
Naprinol®
Dial-a-gesic®
Nobedon®
Dirox®
Ortensan®
Disprol®
Pacemo®
Paldesic®
Panadol®
Panaleve®
Panasorb®
Panets®
Panex®
Panofen®
Parelan®
Paraspen®
Parmol®
Pasolind®
Saizone®
Tabalgin®
Tapar®
Temlo®
Tempra®
Tralgon®
Tylenol®
Valadol®
276
Method of Administration: Acetaminophen will be administered in a double
blind crossover study that compares two formulations of acetaminophen. The products
tested will include acetaminophen immediate release tablets,(2 x 500mg) and a sustained
release acetaminophen preparation (2 x 650mg). Doses of 1000mg every 6 hours or
1300mg every 12 hours will be given for 4 weeks as two separate studies separated by a 7
day "wash-out" (drug free) interval between each study. Patients age 40-75 years of age
with previously diagnosed osteoarthritis of the knee will be asked to participate.
277
1571.2
Chemical Manufacturer
All chemicals used in the production of the sustained release product are of
National Formulary/Unites States Pharmacopeia grade. Copies of the Certificates of
Analysis for each ingredient are included with this packet. They include acetaminophen
NF/USP (Spectrum Chemical MPG. Corp., Gardena, CA) Lot JE321,
polyvinylpyrrolidone K-30 NF/USP (Spectrum Chemical MFG. Corp., Gardena, CA)
Lot KD186, magnesium stearate NF/USP (Spectrum Chemical MPG. Corp., Gardena,
CA) Lot KC502, and Methocel® K100M PREM CR brand of
hydroxypropylmethylcellulose (Dow Chemical Co. Midland, MI) Lot MM92101 105K.
Avicel® microcrystaffine cellulose NF/USP (FMC Corporation, Philadelphia, PA) Lot
Xl 29 is used in place of the acetaminophen in the placebo tablets.
The tablets will be prepared as described in section 1571.4.
Immediate release acetaminophen tablets (500mg) will be purchased at a local
retail outlet and dispensed as received. Lot numbers, retailer information, and expirations
dates will be recorded.
Ibuprofen 200mg tablets will be used as a rescue analgesic during the study. These tablets
will also be purchased at a local retail outlet and dispensed as received. Lot numbers,
retailer information, and expiration dates will be recorded.
278
1571.3
Department of Pharmaceutics Manufacturing Laboratory: College of Pharmacy, Oregon
State University, Corvallis, Oregon
The pharmaceutical manufacturing laboratory at the College of Pharmacy has been
previously used to produce melatonin products and other sustained release
acetaminophen formulations which have been evaluated in human subjects. Several USP
dissolution apparati are available for in vitro evaluation of oral dosage forms. A
friabulator and USP hardness tester are available to evaluate tablet parameters. A single
punch tableting machine is available for tablet production. High Pressure Liquid
Chromatographic (HPLC) systems equipped with a variety of columns and detectors are
available in the laboratory. UV-VIS spectrophotometry, Franz cell diffusion systems,
Perkin-Elmer DSC, gas chromatography, scintillation and gamma counters, and a
laboratory scale spray coater are available for use within the College of Pharmacy. The
handling of radioactive substances is not permitted in the manufacturing laboratory and is
not part of this investigation.
Veterans Administration Hospital: Portland, Oregon
The Hospital has provided service to thousands of U.S. Veterans throughout the years. It
continues to serve patients by providing excellent medical care and by sponsoring medical
research into prevalent conditions and afflictions. See form 1572.
279
1571.4
Manufacture of Sustained Release Tablets
Ingredients and Excipients: A licensed pharmacist at the pharmaceutics
laboratory at Oregon State University will undertake production of the sustained release
tablets. The following materials will be used in the tablets. They include acetaminophen
NF/USP (Spectrum Chemical MFG. Corp., Gardena, CA) Lot JE321,
polyvinylpyrrolidone K-30 NF/USP (Spectrum Chemical MFG. Corp., Gardena, CA)
Lot KD1 86 as a tablet binder, magnesium stearate NF/USP (Spectrum Chemical MPG.
Corp., Gardena, CA) Lot KC502 as a tableting lubricant/glidant, and Methocel® K100M
PREM CR brand of hydroxypropylmethylcellulose (Dow Chemical Co. Midland, Ivil) Lot
MM921 01105K as a sustained release matrix substrate. Avicel® microcrystalline cellulose
NF/USP (FMC Corporation, Philadelphia, PA) Lot Xl 29 is used in place of the
acetaminophen in the placebo tablets. Water used during the granulation process is
distilled and then passed through a de-ionization system.
Cleaning: All surfaces are cleaned prior to each production run. All equipment
and the surrounding area will be cleaned with Alconox®, rinsed with distilled, deionized
water, and swabbed with 95% ethanol. All surfaces will be free of soap residue or films.
The process will be attended at all times.
280
Manufacturing Process: Each tablet contains 89.0% acetaminophen, 5.0%
hydroxypropylmethylcellulose (HPMC), 5.0% polyvinylpyrrolidone (P\TP), and 1.0%
magnesium stearate by weight. The desired amount of PVP is dissolved in 0.75m1 water
per tablet. The HPMC and the acetaminophen are premixed and slowly added to the
PVP solution. The resulting thick paste is extruded into noodles onto a flat, plastic wrap
covered surface and allowed to dry overnight at room temperature. The dried noodles
are mechanically broken up into granules using a mortar and pestle and sieved through a
succession of sieves. Granules that pass through a 14 mesh sieve but are retained on a 60
mesh sieve are used. Granules not within the prescribed range are discarded. Magnesium
stearate is then added to the granules and mixed to thoroughly coat the granules. Tablets
are made from the granules by loading the mixture into a single punch tableting machine
(Chemical and Pharmaceutical Industry Co., New York, NY, Model TPK-12). Ejected
tablets are 12mm in diameter with a 4mm belly band and curved faces. One face of the
tablet is scored across the middle and bears the imprint 427 OPD. Desired tablet weight
is 730mg. Each batch produced will be assigned sequential lot numbers.
Placebo tablets are made by replacing the acetaniinophen in the tablets with
Avicel®. Granulation of the placebo tablets is not necessary as the Avicel® is already
granular. The four ingredients are dry mixed and loaded into the single punch tableting
machine to produce tablets that are identical to the study medication in appearance and
weight.
281
Labeling: Finished tablets will be stored at room temperature in amber vials until
packaging. Each vial will bear the following label:
INVESTIGATIONAL DRUG
Acetaminophen Sustained Release Tablets
650mg
Date
Lot
To help assess compliance the treatment medications will be placed in unit dose
cards. Each card holds a single weeks worth of medication. Each treatment
will
last 4
weeks. All four cards will be dispensed at once. The medication will be placed in REDIPAK® compliance cards and will be labeled for use.
OREGON STATE UNIVERSITY
COLLEGE OF PHARMACY
INVESTIGATIONAL ACETAMINOPHEN STUDY
PATIENT NUMBER 1
TREATMENT 1
WEEK 1
282
DOSE 1
DOSE 2
DOSE 3
DOSE 4
S
U
N
M
0
N
T
U
E
S
w
E
D
T
H
U
R
F
R
I
S
A
T
Patients will be randomly assigned in a crossover fashion to one of two
treatments. Each treatment involves the patient taking 2 tablets four times a day for
four weeks. After a week wash Out period each patient is crossed over to the second
treatment. For one treatment the dose packets will contain 2 X 500mg immediate release
tablets. For the other treatment the dose packets will contain two doses of the sustained
release formulation (Dose I and Dose 3) and two doses of placebo tablets (Dose 2 and
Dose 4). Neither the patient nor the investigator will know which treatment the patient is
currently taking.
283
FDA: Administration of Oral, Sustained Release Acetaminophen Delivery to
Human Subjects.
Tablet Characterization: Each batch of tablets produced will be evaluated for
hardness and friability. Tablet hardness will be measured using a Strong-Cobb hardness
tester. Tablets with hardness values of less than 4kg will be considered unacceptable and
will be discarded. Friability will be tested using a Roche Friabilator. Five tablets from
each batch will be tested for 100 rotations. Tablet samples that lose greater than 1% of
their weight will be considered to be unacceptable and will be discarded.
Each tablet batch will also be weighed and an average tablet weight recorded.
In Vitro Characterization of the Release of Acetaminophen from the Sustained
Release Dosage Form
Six tablets from each batch will be evaluated using a USP dissolution (Paddle
Method) test. For the first two hours each tablet will be exposed to 900m1 of enzymefree simulated gastric fluid (Ph = 1.4). Samples will be taken from the vessels with
replacement at 20 minutes, 40 minutes, 1 hour, 1 hour and 20 minutes, 1 hour and 40
minutes, and 2 hours. After two hours the fluid is filtered through No. 1 filter paper and
the particles retained. The particles and the filter paper will then be exposed to 900m1 of
enzyme-free simulated intestinal fluid (Ph = 7.4) for the remaining 22 hour period.
Samples will be taken with replacement at 3 hours, 4 hours, 6 hours, 9 hours, 12 hours,
and 24 hours. Samples will be diluted 1:100 with distilled, deionized water and analyzed
at 244nm in a Hewlett Packard variable wavelength UV-VTS spectrophotometer equipped
with a sipper cell. Standard solutions of acetaminophen in distilled, deionized water will
284
be used to correlate absorbance to concentration. Previous experience has indicated that
interference from polymers and or other excipients that may be present in the dissolution
medium is negligible.
Dissolution will also be performed on the commercial acetaminophen products
for comparison purposes. By design, the immediate release commercial formulation
should rapidly dissolve in the gastric fluid. Samples will therefore be taken in gastric fluid
only, unless dissolution is incomplete in the first two hours. Samples will be taken with
replacement at 5 minutes, 10 minutes, 15 minutes, 20 minutes, 25 minutes, 30 minutes, 40
minutes 60 minutes, 75 minutes, 90 minutes, 105 minutes and 120 minutes.
Figure 1 is a graph of the drug release from the immediate release acetaminophen
product (2 x 500mg) to be used in this study. Note that dissolution is essentially
complete by the 5 minutes sample time. Figure 2 is a graph of the drug release from the
sustained release acetaminophen tablet (2 x 650mg) to be used in this study.
Section 1571.5
Approved Investigational Research Protocol from Oregon State University.
571.5
Copy of Approved Investigational Research Board Proposal from Oregon State
University.
RESEARCH PROPOSAL INVOLVING HUMAN TEST SUBJECTS
This is a preliminary investigation conducted by Oregon State University College
of Pharmacy Department of Pharmaceutics to evaluate a sustained released formulation
of acetaminophen (Tylenol®). The information collected will be used to establish an in
285
vitro
in vivo
correlation for the development of a new acetaminophen formulation. An
vitro
in vivo
correlation will allow the
in vitro
in
behavior of future formulations to predict in
vivo behavior. New formulations can then be developed with a minimum of human
testing.
Acetaminophen is a widely used, over-the-counter medication for analgesia and
fever. It has been available to the general public for over 30 years. Acetaminophen is
currently given either as an immediate release product (650-1000mg every 4-6 hours) or
as an extended release product (1 300mg every 8 hours). A new sustained release
formulation developed in our laboratory would provide 1300mg every 12 hours. The
sustained release tablets are manufactured using well known procedures and are made
from Food and Drug Administration (FDA) approved ingredients.
Participants will be involved in several one (1) day test periods with a seven (7)
days wash out period between them. Participants will be asked to fast for 2 hours prior
to receiving a dose of acetaminophen. At specified time intervals after dosing,
participants will be asked to chew a one inch square of Parafilm® for 1 minute to
stimulate saliva production and to collect a saliva sample. It has been well documented in
the literature that saliva acetaminophen concentrations are directly correlated with blood
acetaminophen concentrations. All operators handling samples will wear gloves in
compliance with federal "universal precaution" recommendations. All operators are
aware of the risks of handling bio-hazardous materials including the potential for
contracting hepatitis and/or the HIV virus.
286
Justification: Currently available formulations of acetaminophen must be taken
every 4 to 8 hours to maintain adequate drug concentrations in the blood to provide pain
relief. The development of a sustained release formulation would provide extended relief
from pain while minimizing the dose, and thereby the side effects of the drug. Twelve
hour dosing intervals have also been shown to increase the compliance of patients. This
is especially important in patients who require pain relief on a long term basis (arthritis).
Although simulation and calculations may be performed to predict the behavior
of new drug formulations, there are often factors in the body that cannot be foreseen.
The ultimate test of a formulation measures the change in drug concentrations in the
body over the dosing interval. As acetaminophen saliva concentrations can be directly
correlated with plasma concentrations, saliva data can be used as a non-invasive method
of evaluating the performance of new acetaminophen formulations.
Figure 1 is a comparison of in vitro release rates of 3 acetaminophen formulations.
The diamonds represent the dissolution of 1000mg (2 x 500mg) acetaminophen
ylenol
Extra Strength®) tablets. The filled circles show a similar curve for 1300mg (2 x 650mg)
acetaminophen extended release Tylenol ER®) caplets. Note that both of these
products are completely released by 3 hours. The triangles represent the in vitro
dissolution profile of the sustained release formulation developed in our laboratory. Note
that with this product complete release is not obtained until twelve hours.
Side-Effects: Few side effects have been reported with the use of
acetaminophen in therapeutic doses (4 grams a day or less). Reported side effects of
acetaminophen are dose dependant and unlikely, but can include skin rash, hives, itching,
287
bloody or cloudy urine, difficulty in urination, sudden decrease in urine output,
unexplained sore throat or fever, unusual bleeding or bruising, or unusual tiredness or
weakness (see attached United States Pharmacopeia Drug Information sheet. Other
symptoms may occur in overdose situations but are not expected during this study as the
dosage given is below the maximum daily dose of acetaminophen (4 grams per day).
Exclusions: All test participants will be healthy, normal people with no known
medical problems. Pregnant women will be excluded, even though acetaminophen is the
drug of choice for analgesia in these patients, because of the inadvisability of taking any
medication while pregnant if not absolutely necessary. Test subjects will be excluded
from this study if any of the following are true:
1. They have shown any previous hypersensitivity to acetaminophen or to
acetaminophen combination products.
2. They have renal abnormalities or known renal dysfunction.
3. They have liver abnormalities or known liver dysfunction.
4. They are currently taking any prescription or non-prescription form of
acetaminophen or acetaminophen containing product.
5. They are currently taking any medication that might effect the elimination of
acetaminophen (i.e. phenobarbital, phenytoin)
6.
They are or expect to become pregnant during the duration of the study.
7. Persons who have ever had hepatitis B or C, who have tested positive for HIV
or any AIDS virus, who have AIDS, or who are at risk for getting and spreading
any AIDS virus. You are at risk if:
you are a man who has had sex with another man since 1977,
even one time.
you have shared a needle, even one time, to inject drugs
or medication.
288
you have taken clotting factor concentrates for a bleeding
disorder such as hemophilia.
you have ever had a positive test for any AIDS virus or
hepatitis B or C or any AIDS antibody.
you have had sex with any person described above.
you have had sex with a male or female prostitute since
1977.
Test Subjects: Test participants will be 20 healthy, normal volunteers drawn
from the Oregon State University faculty, staff and student population. Written consent
of each participant will be obtained after verbal and written information is presented by a
registered pharmacist.
Anonymity: All records will be kept confidential. The identity of the research
participants will not be released through either oral or written transmission to any
member not directly involved in the research group. Records from each subject shall be
retained in the project file for three years beyond the end date of the project.
MATERIALS AND METHODS
Materials: Acetaminophen NF/USP, lot #JE321 was obtained from Spectrum
Chemical Mfg Corp. Gardena, CA magnesium stearate NF/USP, lot #KC502 was
obtained from Spectrum Chemical Mfg Corp. Gardena, CA,
hydroxypropylmethylcellulose (Methocel® K100M PREM CR) lot #MM92101 105K was
obtained from Dow Chemical Co. Midland, MI, and polyvinylpyrrolidone NF/USP from
289
Spectrum Chemical Mfg Corp. Gardena, CA. All water used was distilled de-ionized
water.
Tablets: Each tablet contains 89.O% acetaminophen, 5.0%
hydroxypropylmethylcellulose (HPMC), 5.0% polyvinylpyrrolidone (PVP), and 1.0%
magnesium stearate by weight. The PVP is dissolved in 0.5m1 of water per tablet. The
HPMC and the acetatninophen are premixed and then slowly added to the PVP solution.
The resulting thick paste is extruded into noodles and dried. The dried noodles can then
be broken into granules. Magnesium stearate is added to the granules and mixed to
thoroughly coat the granules. Tablets are made by placing loading granules into a single
punch tableting machine. Desired tablet weight is 730.Omg.
Subjects: Test participants are normal, healthy volunteers who are not currently
taking any prescription or non-prescription forms of acetaminophen and have previously
fasted for 2 hours or greater prior to the dose. Fasting must continue for two hours after
taking the dose. Subjects will not be allowed to eat or drink anything 5 minutes before
each sample.
Design: A cross-over design will be used. Subjects are randomly assigned to one
of the three formulations. After a one week wash out period, a second formulation will
be given. Finally, after a second week long wash out period, the third formulation will be
given.
290
Sampling: Saliva samples will be collected at times 0.0, 0.5, 1.0, 1.5, 2.0, 3.0, 4.0,
5.0, 6.0, 9.0, 12.0 and 24.0 hours. Each participant will chew a 1 inch square of
Paraflim® for 1 minute during each sample collection to initiate adequate saliva flow.
Saliva produced during the minute of chewing will then be collected for each time point
and frozen for later analysis.
Solutions:
1. Acetaminophen standards of 0.4, 1.0, 2.0, 4.0, 6.0, 8.0, 10.0, and 16.0 tg/m1 in water
will be used. All standards were made by aliquot dilution of a 1000 tg/ml stock solution.
2. Internal standard solution of 40 tg/m1 7-beta- hydroxyethyl- theophylline.
3. Mobile phase of 30% methanol and 70% water.
Assay: All saliva samples will be frozen prior to use (-20°c). Aliquots of saliva
will be centrifuged at 14,000 rpm for 2 minutes to pelletize particulates. One hundred
fifty d of supernatant will be then pipetted into a micro centrifuge tube. One hundred
fifty pi of the internal standard (7-beta-hydroxyethyl theophyffine) will be added and the
mixture vortexed for 30 seconds.
Chromatography: Samples will be injected onto the High Pressure Liquid
Chromatograph (HPLC) using an automatic sampler (WISP 712; Waters Assoc.)
Separations of components is obtained by using a Cl 8-Reverse Phase column. The
mobile phase of 30% methanol/70% water will be delivered at a rate of 0.8m1/min (M6000A Solvent Delivery System) and samples will be monitored at 254nm with a model
440 absorbance detector. Injection volume will be set at 20 jtl.
291
Quantitation: Standard curves are run daily. Quantitation of the sample curves
is based on peak height ratios using the internal standard peak as the divisor. The
resulting calibration curve is fitted using PSI-PLOT® to a least-squared linear regression
line. The equation is then used to convert peak ratios into corresponding concentrations.
CONSENT FORM
This study is a research project conducted by the Department of Pharmaceutics,
College of Pharmacy, Oregon State University. The purpose of this study is to evaluate a
sustained release formulation of the drug acetaminophen. Acetaminophen (Tylenol®) is
a non-prescription medication that is used to treat mild pain and fever. Currently the
medication must be taken 3-4 times a day. The new formulation that you will take is
designed to release slowly over a 12 hours period.
Your participation will involve one (1) day per week for three (3) weeks (3 days
total with a 7 day wash out period between doses). You will be asked not to eat for at
least 2 hours prior to the study and after the dose, and to refrain from eating or drinking
for 5 minutes before each sample time. After dosing, you will be given a time sheet for
recording sample times, tubes in which to collect saliva samples, and 1 inch squares of
Paraflim®. You must chew the square of Paraflim® for 1 minute during each sample
collection to stimulate saliva production. A total of 12 saliva samples will be collected
over the 24 hour period.
Side Effects: If you have previous taken Tylenol® or Tylenol Extra Strength®
with no untoward effects, you should not experience any difficulty with this product. On
292
rare occasions, people taking acetaminophen develop a rash or drowsiness. Any possible
side effects or abnormal symptoms that you experience should be reported to the study
investigator immediately.
Exclusions: You are excluded from this study if you are not a normal, healthy
adult free of known liver or kidney damage or if you are pregnant or plan to become
pregnant during the study period. You are also excluded if you have ever shown any
sensitivity to acetaniinophen or acetaminophen containing products. Subjects should not
be taking any medications that might effect the elimination of acetaminophen (i.e.
phenobarbital, phenytoin, etc.)
Anonymity: All records will be kept confidential. The identity of the research
participants will not be released through either oral or written transmission to any
member outside of the research group.
Confidentiality: I have been informed that because this study involves articles
regulated by the FDA (Food and Drug Administration), the FDA may choose to inspect
records identifying me as a subject in this investigation.
Withdrawal: Participation in this study is voluntary, you may withdraw at any
time. There is no penalty if you withdraw from the study for any reason: exclusion,
competing commitments, drug reaction, loss of interest. No loss of benefits, standing, or
relationship with the research group or Oregon State University will result.
293
Questions about the research, your rights, or research related injuries should be directed
to James Ayres, Ph. D., at 737-5787, or Carol Keller at 737-5771.
I have read the consent form above and I understand the information presented. I
understand that the University does not provide a research subject with compensation or
medical treatment in the event that the subject is injured as a result of participation in the
research project. My participation is voluntary, and refusal to participate will involve no
penalty or loss or benefits to which I am otherwise entitled, and that I may discontinue
participation at any time without penalty or loss of benefits to which I am otherwise
entitled.
Signature
D
294
DATA SHEET
Please record the time of each sample collection to the nearest 5 minutes.
Time the dose was taken:_______________
Hours after dose
Time sample was taken
0.0
0.5
1.0
1.5
2.0
3.0
4.0
5.0
6.0
9.0
12.0
24.0
Date:
295
SUBJECT DATA SHEET
Data for Subject:____________________ Identifier:
Formulation:
Hours after dose
Actual time
Concentration
0.0
0.5
1.0
1.5
2.0
3.0
4.0
5.0
6.0
9.0
12.0
24.0
Signature:
Date:
'S.
Section 1571.6
Proposed Research Protocol for the Veterans Administration Hospital
Copy of Proposed Investigational Research Protocol for the Veterans
Administration Hospital.
VA RESEARCH CONSENT FORM 10-9012
DESCRIPTION OF RESEARCH BY INVESTIGATOR
Purpose: You have been asked to participate in a research study to determine if a
new long acting formulation of acetaminophen (Tylenol®) can control your osteoarthritis
(joint) pain. You have been asked to participate in this study because you have been
diagnosed with osteoarthritis and have had pain because of this disease. Acetaminophen
has been previously shown to be effective in treating pain due to osteoarthritis but it has
to be taken four times a day. A new longer acting form of the drug would allow it to be
taken only two times a day. This study is important because it will help evaluate new
form of the drug and how well it works. This study will last for 9 weeks and will require
three 1-hour visits.
Procedures: If you agree to participate in this study, you will be asked to come to
the clinics at the Veterans Administration Hospital. You will be asked to complete a
questionnaire about yourself and the type of pain that you have. In addition, you will be
asked to walk 50 feet to evaluate how well you can move.
At the first visit you will be given a study medication packet. For 4 weeks, you
will be asked to take 2 tablets of your study medication four times a day. You will be
taking either two short-acting acetaminophen tablets (500mg each) four times a day, or
297
two long acting acetaminophen tablets (650mg each) alternating with two placebo tablets.
A placebo is a tablet that contains no active drug. Neither you nor the investigators will
know which study medication you receive. Ibuprofen tablets (200mg) will be provided
for pain not relieved by the study medication. You will be asked to keep track of how
many ibuprofen tablets that you use. A maximum of 2 ibuprofen tablets twice a day will
be allowed.
After the four week period you will be asked to return to the center and repeat
the questionnaire and walking test. In addition, you will be asked to provide a saliva
sample. The saliva samples will tell us how much medication is in the blood without
having to actually draw blood. At this visit, you will be provided with the other type of
medication to take for a second four week period. You must wait a week for the effects
of the first medication to wear off before you begin taking the second medication.
Ibuprofen will be provided for pain relief during the week between medications. Again,
at the end of the four week period you will be asked to repeat the questionnaire and
walking test.
Risks and Discomforts: There may be adverse reactions involved in
participating in this study. The most common reaction is sleepiness. Very rarely,
acetaminophen can result in a rash or hives. This means that you are allergic to the
medication. You should stop taking the medication and immediately inform one of the
study investigators. Your symptoms will be treated and the study will be stopped.
Acetaminophen can cause liver problems, nausea, vomiting, and kidney problems. The
doses in this study are much less than the doses that cause these problems doses, but if
298
nausea or vomiting develop, you may be unusually sensitive to the medication and the
study will be stopped.
Benefits: You may benefit from your participation in this study in that the pain
due to your osteoarthritis may be reduced or eliminated. It is also possible that you pain
will not be controlled by the use of this medication, and it will then be necessary to take
the ibuprofen which has been provided for additional pain control.
Alternative Treatments: If you do not choose to participate in this study, other
drugs are available for the treatment of osteoarthritis. They include non-steroidal-antiinflammatory medication like ibuprofen, aspirin, naprosyn and narcotic pain relievers
such as Darvocet N-100®, Vicodin®, and Tylenol #3®.
Exclusions: You should not participate in this study if you have shown previous
side effects from Tylenol® or other acetaminophen containing combinations. You
should not participate in this study if you have shown previous side effects to Motrin®,
Advil®, or other forms of ibuprofen. You should not participate in this study if you have
had recent (last 3 months) trauma to the affected joint or injections into the joint.
Pregnant women will not be allowed to participate in this study. Although the
medication will not harm the child, it is not a good idea to be taking any un-needed
medication if you are pregnant. You should be able to walk 50 feet without assistance or
assistive devices (canes, walkers, etc.)
299
Your participation in this study is voluntary, and you may withdraw from this
study at any time without prejudice to yourself or to any future medical care with this
institution or with the Department of Veterans Affairs(VA).
You may be removed from the study without your consent if your doctor decides
that this is in your best interest, or if you fail to follow the study schedule (such as not
taking your assigned medication). Follow-up visits may still be recommended after your
withdrawal.
Costs: The investigators will pay any medication costs involved in this study.
You will not be charged for your participation in this study.
Compensation: Your participation in this study is free of charge. You will
receive no money for participating in this study.
Liability: Every reasonable effort to prevent any injury that could result from this
study will be taken. In the event of physical injury resulting from the study, medical care
and treatment will be available at this institution. For eligible veterans, compensation
damages may be payable under 38 Usc 251 or, in some circumstances, under Federal
Tort claims Act. For non-eligible veterans and non-veterans, compensation would be
limited to situations where negligence occurred and would be controlled by the
provisions of the Federal Tort claims Act. For clarification of these laws, contact
District counsel at (503)326-2441. You have not waived any legal rights or released the
hospital or its agents from liability for negligence by signing this form.
300
Confidentiality: The results of your participation in this study may be used for
publication or for scientific purposes, but your identity will not be disclosed unless you
give separate, specific consent to this, or unless required by law.
Other: Registered Pharmacists Theresa Bianco, Pharm. D. (273-5398) and Carol
Keller, R. Ph. (737-7776) have offered to answer any questions that you may have.
You will receive a copy of this consent form. Your signature below indicates that you
have read the foregoing and agree to participate in the study.
Name
Da
301
RDIS ABSTRACT VA FORM 10-1436
Objective: The specific aim of this study is to compare the effectiveness of a
new sustained release formulation of acetaminophen with currently available
acetaminophen products for the relief of pain due to osteoarthritis.
Research Plan: This study is a randomized, double blind, placebo controlled
cross-over study. The study population will consist of patients with previously diagnosed
osteoarthritis of the knee.
Methodology: After signed consent is obtained and inclusion/exclusion criteria
are met, patients will undergo an initial evaluation. A history and disease characterization
will be performed including height, weight, and age. An initial evaluation of the type and
duration of pain in the patient will be assessed using modified Stanford Health
Assessment Questionnaire (HAQ) pain scores and time to walk 50 feet.
Enrolled patients will be randomly assigned to one of two groups. Each group
will be asked to take two tablets four times a day. Group I will take two 500mg
acetaminophen tablets four times a day. Group 2 will take two 650mg sustained release
tablets twice a day with 2 identical placebo tablets for the remaining two doses. Doses
will be individually packaged to help assess compliance. Patients will be asked to
continue the dosing regimen for four weeks. Compliance will be assessed by tablet count.
Ibuprofen 200mg tablets will be provided to patients as a rescue analgesic. Patients will
be asked to record their usage of the rescue analgesic. A maximum of 400mg of
ibuprofen every 6 hours may be taken. At the end of the four week study period, patients
302
will be asked to repeat the initial evaluation of their pain. Patients will also be asked to
provide a saliva sample at the time of reassessment just prior to the final dose of the
medication to assess compliance and to evaluate the relationship of saliva acetaminophen
concentrations to pain control. After a 7 day washout period, patients will then be
crossed over to the other treatment for an additional 4 weeks. Reassessment will be
repeated after the second four-week period.
Laboratory Analysis: Saliva samples will be collected in 10m1 plastic sample
tubes and immediately frozen at 4°c until analysis. Samples are then thawed, centrifuged
at 3000 rpm for 10 minutes, and the supernatant refrozen. Samples are re-thawed, re-
centrifuged, and 1 50l of the supernatant is transferred to a microcentrifuge tube. A
1 50d aliquot of 7-beta-hydroxyethyl-theophyffine 40jtg/ml is added as an internal
standard. Samples will be analyzed in duplicate using high pressure liquid
chromatography to determine acetaminophen concentrations.
303
EVALUATION OF A CONTROLLED RELEASE ACETAMINOPHEN
TABLET FOR ANALGESIA IN OSTEOARTHRITIS PATIENTS
A PILOT STUDY
Principal Investigators
Theresa M. Bianco, Pharm. D.
Carol A. Keller, R. Ph.
Introduction: An estimated 40.5 million adults in the United States suffer from
some form of osteoarthritis (OA)1. With a steadily aging population, that number is
expected to increase in the coming years. The disease is age associated and the
prevalence ranges from 4% in people age 18-24 years old to 85% in patients 75-79 years
old.1'2
The incidence of OA is higher in women and in some racial
types.1'3
The specific
aim of this study is to assess the effectiveness of a novel sustained release formulation of
acetaminophen in relieving pain in these patients.
The symptoms of osteoarthritis vary with the duration of the disease and the
number of joints that are involved. The predominant symptom is a localized deep,
aching pain in the affected joint(s). Early in the course of the disease, the pain is present
when the affected joint is first used and is relieved when the joint is at rest or when
weight is removed from the joint. As the disease progresses, the pain can become present
with minimal movement and at rest. In addition to pain, patients may experience loss of
range-of-motion (ROM), stiffness, and physical deformities.1
No cure exists for OA. Treatment is aimed at reducing pain, maintaining
mobility, and minimizing disability.4 Historically, OA has been treated much like
rheumatoid arthritis, with non-steroidal-anti-inflammatory medications
(NSAIDS).57
Although effective, these medications present several problems in the elderly population
304
with OA. The NSAIDS cause significant gastric distress and ulceration, increase
prothrombin time, and have uricosuric activity.5 Recently, it has been shown that since
OA does not involve an inflammatory component, that pure analgesic medication, such
as acetaminophen, are equally effective as NSAIDS in the relief of the pain and stiffness
these patients experience without some of the side
effects.5'812
Acetaminophen has been safely used for over 30 years as an over-the-counter
analgesic. In therapeutic doses of less than 4 grams per day, it does not cause gastric
distress, changes in prothrombin times, or uricosuric activity. The major problem with
using acetaminophen for chronic pain relief has been the fact that traditional immediate
release formulation must be taken every 4-6 hours to maintain analgesic effect. The
immediate release preparations do not provide lasting relief for these patients and the
potential exists for patients to take excessive doses in an effort to maintain analgesia for a
longer period of time. Chronic ingestion of greater then 4 grams per day primarily
manifests as hepatic necrosis that is characterized by nausea, vomiting, and abdominal
pain that can progress to methemoglobinemia, vascular collapse, hepatic coma and death
if left untreated.1'1316 In addition, chronic abuse can also result in renal papillary necrosis
and interstitial nephritis. Oliguria, hematuria, and renal insufficiency can result if left
untreated.13'16'17
There is a great need for a longer lasting product that would maintain
sufficient blood levels of the drug for analgesia, while minimizing the overall daily dose
and maximizing convenience to the patient. Studies have shown the efficacy of
immediate release acetaminophen in osteoarthritis patients.20'1' This study was designed
to evaluate a novel sustained release formulation of acetan-iinophen for chronic pain relief
in osteoarthritis patients.
305
Results to Date: Preliminary pharmacokinetic calculations were performed using
published
parameters.21
The pharmacokinetics goal is to maintain Cp> 5.Omg/L for the
full 12 hours. Initial in vitro evaluation of the drug product were completed and release
factors were optimized. Pharmacokinetic in
vivo
evaluation is currently underway and the
release characteristics of the formulation will be finalized based on the correlation
developed between the in vitro and in
vivo
results.
Research Design
Goal: To evaluate the effectiveness of a novel sustained release preparation of
acetaminophen in the relief of pain in osteoarthritis patients.
Study Design: This is a randomized, double blind, placebo controlled study in a
crossover design.
Inclusion criteria: Patients with chronic mechanical-type knee pain and
previous diagnosis of osteoarthritis of the knee. Age is 18-75 years inclusive. Lack of
trauma to the affected joint(s) or intra-articular corticosteroid injections in the last three
months.
Exclusion criteria: Previous history of sensitivity to acetaminophen or
acetaminophen combination products. Previous history of sensitivity to ibuprofen.
History of trauma or intra-articular corticosteroid injections in the affected joint(s) in the
last 3 months. Patients with any other medical condition which would limit ability to
walk 50 feet including but not limited to, angina pectoris, congestive heart failure, chronic
obstructive pulmonary disease, peripheral vascular disease, fibromyalgia, bursitis,
306
inflammatory arthritis, or other musculoskeletal conditions of the leg which could cause
concomitant leg pain. Patients must be able to walk 50 feet without assistance or assistive
devices. Patient with renal insufficiencies, gastric ulceration, undergoing thrombolytic
therapy, or any medical condition in which non-steroidal anti-inflammatory medications
would be contra-indicated will also be excluded from this study.
Sample size justification: Sample size calculations were performed using data
published by Bradley et a111. Bradley compared two treatments for osteoarthritis in a
parallel design using a modified HAQ test and time to walk 50 feet. Using his published
data, within-subject estimates of treatment differences and standard deviations were
calculated. After adjusting for the crossover design and setting = 0.1 and power = 80%
a sample size of 40 was calculated.
Methods and Procedures: After signed consent is obtained and
inclusion/exclusion criteria are met, patients will undergo an initial evaluation. A history
and disease characterization will be performed including height, weight, and age. An
initial evaluation of the type and duration of pain in the patient will be assessed using
modified Stanford Health Assessment Questionnaire (HAQ) pain scores (Appendix A)
and time to walk 50 feet.
Enrolled patients will randomly assigned to one of two groups. Each group will
be asked to take two tablets four times a day. Group 1 will take two 500mg
acetaminophen tablets four times a day. Group 2 will take two 650mg sustained release
tablets twice a day alternating with 2 identical placebo tablets for the remaining two doses
per day. Doses will be unit dosed to help assess compliance. Patients will be asked to
307
continue the dosing regimen for four weeks. Compliance will be assessed by tablet count.
Ibuprofen 200mg tablets will be provided to patients as a rescue analgesic. Patients will
be asked to record their usage of the rescue analgesic. A maximum of 400mg of
ibuprofen may be taken every 6 hours. At the end of the four week study period, patients
will be asked to repeat the initial evaluation of their pain. Patients will also be asked to
provide a saliva sample at the time of reassessment just prior to the final dose of the
medication to assess compliance and to evaluate the relationship of saliva acetaminophen
concentrations to pain control.21'23 After a 7 day washout period, patients will be crossed
over to the second treatment. After a 4 week period, the patients will return for a third
and final evaluation.
Laboratory analysis: Saliva samples will be collected in lOmi plastic sample
tubes and immediately frozen at 4°C until analysis. Samples are then thawed, centrifuged
at 3000 rpm for 10 minutes, and the supernatant refrozen. Samples are re-thawed, re-
centrifuged, and I 50tl of the supernatant is transferred to a microcentrifuge tube. A
1 5OpJ aliquot of 7-beta-hydroxyethyl-theophylline is then added as an internal standard.
The samples are centrifuged a third time and transferred to lml high pressure liquid
chromatography (HPLC) tubes for analysis. Samples
will
be run in duplicate to verify
acetaminophen concentrations.
Data Analysis: Data collected on pain control will be analyzed using analysis of
variance. Data will be analyzed as a randomized block design with factors included in the
model for treatment order and carryover effects. Correlation between saliva
acetaminophen concentrations and pain control will also be analyzed using an analysis of
variance.
308
Appendix A
Initial Demographic Information
Visit 1
To be administered by the Investigator
N
Age
Sex
Height
Weight
lbs.
How long have you been diagnosed with osteoarthritis?
Which joint(s) are affected by the osteoarthritis?
Do you usually have pain associated with your illness?,
What medication do you normally take to relieve this pain?
Does this product adequately relieve your pain?
Have you taken Tylenol® or Tylenol® containing products in the
last 7 days?
309
Have you ever had any problems or side effects while taking Tylenol® or
Tylenol® containing products? YES
NO
If so, what?
Have you ever had any problems or side effects while taking Advil®, Motrin®,
or ibuprofen containing products? YES NO
If so, what?
What medications have you taken in the past for your
osteoarthritis?
What prescription medications do you currently take?,
What non-prescription medication do you take. Include vitamin
preparations.
310
Inclusion/Exclusion Criteria
Do you have a history of:
1. Trauma to the affected joint in the last 3 months
YES NO
2. Corticosteroid injections in the last 3 months
YES NO
3. Angina
YES NO
4. Congestive Heart Failure
YES NO
5. Chronic Obstructive Pulmonary Disease
YES NO
6. Peripheral Vascular Disease
YES NO
7. Fibromyalgia
YES NO
8. Bursitis
YES NO
9. Rheumatoid Arthritis
YES NO
10. Kidney Problems
YES NO
11. Ulcers
YES NO
Pain Evaluation Visit
2
1
3
Subject
Treatment
How would you rate your overall pain during the last 4 weeks?
1
mild
2
3
mod
severe
How would you describe the change in your pain in the last 4 weeks?
1
2
better
no change
3
worse
My pain is best described as:
1
2
3
periodic
daily
constant
311
I need help from another person to do the following things:
Seldom
Dress
1
Sometimes
Often
2
3
Eat
1
2
3
Standup
1
2
3
Walk
1
2
3
Climb stairs
1
2
3
Clean House
1
2
3
The pain medication that I have been taking for the last 4 weeks relieves my pain Seldom
Sometimes
2
1
Often
3
The pain relief lasts for the entire time between doses
Seldom
1
Sometimes
2
Often
3
List any side effects or problems with the medication that you have been taking
for the last 4 weeks.
Time to walk 50 fe
312
References:
1.
DiPiro, J.T., Talbert, R.L., Hayes P. E., et. al.: Pharmacotherapy: A
Pathophysiologic Approach, Chapters 32 and 61. New York, New York. Elsevier
Science Publishing Co. 1989.
2.
Felson, D. T., Naimark A. Anderson, J., et. al..: The Prevalence of Knee
Osteoarthritis in the Elderly: The Framingham Osteoarthritis Study. Arthritis and
Rheumatism, Vol. 30, No. 8 (August 1987). pg. 914-918.
3.
Felson, D. T.: Osteoarthritis. Epidemiology of Rheumatic Disease. Vol. 16, No. 3,
August 1990. pg. 499-510.
4.
Wilson, J. D., Braunwald, E., Isdselbacher, K. J., et. al.: Harrisons Principles of
Internal Medicine 12th Ed. Chap. 281. New York, New York. McGraw-Hill Inc.
1991.
5.
Baker,J. R. and Brandt, K. D.: Reappraisal of the Management of Patients with
Osteoarthritis. Informational handout distributed by McNeil Consumer Products
Co.
6.
Pinals, Robert S. Pharmacologic Treatment of Osteoarthritis. Clinical
Therapeutics. Vol. 14, No. 3, 1992. pg. 336-46.
7.
Arfag, Abdulrhman A. and Davis, Paul: Osteoarthritis 1991: Current Drug
Treatment Regimens. Drugs. Vol.41, No. 2, 1991. pg. 193-201.
8.
Calm, Andrei: Pain and Inflammation. The American Journal of Medicine.
September 10, 1984. pg. 9-15.
9.
Brandt, Kenneth D. and Bradley, John D.: Simple Analgesics versus NSAIDs for
Osteoarthritis. The Lancet. Vol. 341, March 20, 1993. pg. 770-1.
10.
Amidio, P. and Cummings, D.M.: Evaluation of Acetaminophen in the
Management of Osteoarthritis of the Knee. Current Therapeutic Research. Vol.
34, No. 1,July, 1983. pg. 59-66.
11.
Bradley, John D., et. al.: Comparison of an Antiinflammatory Dose of Ibuprofen,
an Analgesic Dose of Ibuprofen, and Acetaminophen in the Treatment of Patients
with Osteoarthritis of the Knee. The New England Journal of Medicine. Vol. 325,
No. 2, July11, 1991. pg. 87-91.
12.
Amadio, P.: Orally Acting Analgesics. The American Journal of Medicine.
September 10, 1984. pg. 17-24.
313
13.
Handbook of Drug Therapy in Liver and Kidney Disease, Chap. 3, Analgesics and
Sedative-Hypnotics. Edited by Schrier, R> W. and Gambertoglio, J. G. pg. 51.
14.
Drug Information, 1990, Section 28:08.92 Miscellaneous Analgesics and
Antipyretics. pg. 1104-1109.
15.
Goodman and Gilman's The Pharmacologic Basis of Therapeutics, 8th edition,
Chap. 26 Analgesic-Antipyretics and Antiinflammatory Agents. pg. 656-59.
16.
Handbook of Nonprescription Drugs, 9th edition. pg. 71.
17.
Walker, RobertJ.: Paracetamol, nonsteroidal Anti-inflammatory drugs and
nephrotoxicity. North Carolina Medicine Journal. May 8, 1991. Leading Article.
18.
Nielsen,j.c., Bjerring, P., Arendt-Nielsen, L., and Petterson, K.J.: Analgesic efficacy
of immediate and sustained release paracetamol and plasma concentration of
paracetamol. Double-blind, placebo controlled evaluation using painful laser
stimulation. Eur. J. Clin Pharmacol (1992)42:261-264.
19.
Strom, C., Forsberg, 0., Quidind, H., et.al.: Analgesic efficacy of acetaminophen
sustained release. J Clin Pharmacol 1990;30:654-659.
20.
Nielsen, J. C., Bjerring, P., Arendt-Nielsen, L.:A comparison of the hypoanalgesic
effect of paracetamol in slow release and plain tablets on laser-induced pain. Br J
Clinical Pharmac (1991):30:267-270.
21.
Hossain, Mohammad and Ayres, James: Pharmacokinetic and pharmacodynaniics
in the design of controlled-release beads with acetaminophen as a model drug. J
Pharm Sci. Vol 81, No. 5, May 1992:444-448.
22.
Fries, James F., Spitz, Patricia W., and Young, Donald Y.: The Dimensions of
Health Outcomes: The Health Assessment Questionnaire, Disability and Pain
Scales. J Rheum. 9:5,1982:789-793.
23.
Smith, M., Whitehead, E., O'Sullivan, G., and Reynolds, F.:A comparison of serum
and saliva paracetamol concentrations. Br J Clin Pharmacol 1991,31:553-555.
314
APPENDIX 3D:
Raw Data From Questionnaires
315
Question I: Overall Pain Rating
Patient
Evaluation
Tx #2
After Tx
________ After Tx 2
Evaluation
Baseline
Fvi1iiation
Tx #1
1
2
JR
1
SR
I
2
2
SR
I
JR
2.5
3
3
SR
3
JR
1
4
3
JR
2
SR
I
5
2.5
SR
3
JR
2
6
3
JR
2.5
SR
3
7
3
JR
3
SR
I
8
2
JR
SR
I
9
2.5
SR
10
1
SR
11
1
JR
12
1
SR
13
2
SR
2
JR
1
14
1
IR
1
SR
1
15
2
SR
16
2.5
SR
17
1.5
SR
18
2
SR
19
3
SR
JR
20
2
SR
JR
21
2
JR
SR
22
1
JR
SR
23
1
JR
SR
24
2.5
JR
2
SR
2
25
3
JR
2
SR
I
26
3
JR
1
SR
2
27
1
SR
I
JR
2
28
2
JR
1
SR
29
30
3
I
1
JR
JR
1
SR
I
JR
JR
2
JR
2
JR
2
JR
SR
JR
SR
JR
2
316
Question 2: Change in Pain
Patient
Baseline
Tx #1
Evaluation
Tx #2
Evaluation
After Tx 2
After Tx I
Evabipi-inn
1
2
JR
1
SR
I
2
2
SR
1
JR
2
3
1
SR
2
JR
2
4
2
JR
2
SR
I
5
2
SR
2
JR
1
6
3
JR
2
SR
3
7
2
JR
3
SR
I
8
3
JR
2
SR
1
9
2
SR
1
JR
10
2
SR
11
2
JR
12
2
SR
13
3
SR
2
JR
1
14
2
JR
I
SR
2
15
2
SR
16
2
SR
17
2
SR
18
2
SR
19
2
SR
JR
20
2
SR
JR
21
2
JR
SR
22
2
JR
SR
23
2
JR
SR
24
2
JR
1
SR
1
25
2
JR
1
SR
2
26
2
JR
2
SR
3
27
1
SR
1
JR
I
28
2
JR
SR
SR
JR
SR
JR
29
30
1
JR
2
SR
2
JR
JR
I
JR
I
JR
3
JR
2
317
Question 3: Description of Pain
Patient #
Baseline Tx #1
Evaluation
Fvi1iitip
After Tx
Tx #2
Evaluation
After Tx 2
1
1
3
JR
3
SR
3
2
2
SR
1
JR
1
3
1
SR
3
JR
3
4
3
JR
I
SR
2
5
3
SR
1
JR
3
6
3
JR
3
SR
3
7
3
JR
3
SR
3
8
3
JR
3
SR
2
9
1
SR
1
JR
10
1
SR
11
2
JR
12
3
SR
13
3
SR
2
JR
2
14
1
JR
1
SR
1
15
2
SR
16
3
SR
17
3
SR
18
2
SR
19
3
SR
JR
20
3
SR
JR
21
1
JR
SR
22
1
JR
SR
23
1
JR
SR
24
2
JR
1
SR
I
25
2
JR
3
SR
3
26
2
JR
I
SR
1
27
1
SR
3
JR
3
28
3
JR
SR
SR
JR
SR
JR
29
30
3
JR
1
SR
1
JR
JR
3
JR
3
JR
3
JR
2
318
Question 4: Disability Dressing
Patient #
Baseline
Tx #1
Evaluation
After Tx
Fvaliiition
Tx #2
Evaluation
After Tx 2
1
1
1
JR
I
SR
1
2
1
SR
1
JR
1
3
1
SR
1
JR
I
4
1
JR
1
SR
I
5
2
SR
1
JR
I
6
1
JR
I
SR
1
7
2
JR
1
SR
I
8
1
JR
1
SR
I
9
1
SR
1
JR
10
1
SR
11
1
JR
12
1
SR
13
1
SR
I
JR
1
14
1
JR
1
SR
1
15
1
SR
16
1
SR
17
1
SR
18
1
SR
19
1
SR
JR
20
1
SR
JR
21
1
JR
SR
22
1
JR
SR
23
1
JR
SR
24
1
JR
1
SR
2
25
1
JR
1
SR
I
26
1
JR
1
SR
I
27
1
SR
1
JR
1
28
1
JR
SR
SR
JR
SR
IR
29
30
1
JR
1
SR
1
JR
IR
1
JR
I
JR
1
JR
1
319
Question 5: Disability Eating
Patient #
___________
Baseline
Tx #1
Evaluation
After Tx
Fvaliiatip
Tx #2
Evaluation
After Tx 2
1
1
1
JR
I
SR
2
1
SR
I
JR
1
3
1
SR
1
JR
1
4
1
JR
1
SR
1
5
1
SR
1
JR
I
6
1
JR
I
SR
I
7
1
JR
1
SR
I
8
1
JR
1
SR
I
9
1
SR
1
JR
10
1
SR
11
1
JR
12
1
SR
13
1
SR
1
JR
1
14
1
JR
1
SR
1
15
1
SR
16
1
SR
17
1
SR
18
1
SR
19
1
SR
JR
20
1
SR
JR
21
1
JR
SR
22
1
JR
SR
23
1
IR
SR
24
1
JR
I
SR
1
25
1
JR
I
SR
I
26
1
JR
I
SR
1
27
1
SR
1
JR
1
28
1
JR
SR
SR
JR
SR
JR
29
30
1
JR
I
SR
1
JR
JR
1
JR
I
JR
1
JR
I
320
Question 6: Disability Stand Up
Patient #
Baseline
Fva1uitio
Tx #1
Evaluation
Tx #2
Evaluation
After Tx 2
After Tx 1
1
1
IR
I
SR
I
2
1
SR
I
JR
1
3
2
SR
I
JR
1
4
2
JR
1
SR
1
5
2
SR
I
IR
I
6
2
JR
1
SR
1
7
1
JR
1
SR
I
8
1
JR
1
SR
1
9
1
SR
1
JR
10
2
SR
11
1
JR
12
1
SR
13
2
SR
I
JR
1
14
1
JR
1
SR
I
15
1
SR
16
1
SR
17
1
SR
18
1
SR
19
2
SR
JR
20
1
SR
JR
21
1
JR
SR
22
1
JR
SR
23
1
IR
SR
24
3
JR
3
SR
2
25
1
JR
I
SR
I
26
1
JR
I
SR
1
27
2
SR
2
JR
2
28
2
JR
SR
SR
JR
SR
JR
29
30
1
JR
1
SR
1
JR
JR
1
IR
1
JR
1
JR
I
321
Question 7: Disability Walking
Patient
Baseline
Tx #1
Evaluation
Tx #2
After Tx 2
After Tx 1
Evahiarion
Evaluation
1
1
JR
I
SR
I
2
1
SR
I
JR
1
3
2
SR
I
JR
I
4
1
JR
I
SR
I
5
1
SR
I
JR
2
6
1
JR
I
SR
I
7
1
JR
I
SR
1
8
1
JR
I
SR
I
9
1
SR
I
JR
10
1
SR
11
1
JR
12
1
SR
13
2
SR
I
JR
1
14
1
JR
I
SR
1
15
1
SR
16
2
SR
17
1
SR
18
1
SR
19
1
SR
JR
20
1
SR
JR
21
1
JR
SR
22
1
JR
SR
23
1
JR
SR
24
1
JR
1
SR
2
25
1
JR
1
SR
I
26
1
JR
I
SR
I
27
1
SR
I
JR
1
28
2
JR
SR
SR
JR
SR
JR
29
30
2
JR
I
SR
I
JR
JR
2
JR
2
JR
I
JR
1
322
Question 8: Disability Climbing Stairs
Patient #
Tx #2
Evaluation
Baseline
Evi1iiitinn
Tx #1
1
1
JR
I
SR
2
2
1
SR
2
JR
1
3
1
SR
1
JR
1
4
1
JR
2
SR
1
5
2
SR
I
JR
1
6
1
JR
1
SR
2
7
3
JR
3
SR
1
8
2
JR
2
SR
I
9
1
SR
I
JR
10
1
SR
11
1
JR
12
1
SR
13
3
SR
2
IR
1
14
1
JR
1
SR
1
15
1
SR
16
3
SR
17
1
SR
18
1
SR
19
2
SR
JR
20
3
SR
JR
21
1
JR
SR
22
1
JR
SR
23
1
JR
SR
24
3
JR
3
SR
3
25
1
JR
1
SR
I
26
1
IR
1
SR
1
27
1
SR
2
JR
1
28
1
JR
SR
SR
JR
SR
JR
29
30
2
Evaluation
After Tx 2
Aftt'r Tx 1
JR
1
SR
I
JR
JR
2
JR
2
JR
I
JR
1
323
Question 9: Disability Clean House/Everyday Chores
Patient #
Tx #2
Evaluation
Baseline
Evaluation
Tx #1
1
1
JR
I
SR
I
2
1
SR
I
JR
I
3
1
SR
I
JR
1
4
1
JR
I
SR
1
5
1
SR
1
JR
I
6
1
IR
2
SR
1
7
1
JR
1
SR
1
8
1
JR
1
SR
1
9
1
SR
1
JR
10
1
SR
11
1
JR
12
1
SR
13
2
SR
1
JR
1
14
1
JR
1
SR
I
15
1
SR
16
2
SR
17
1
SR
18
1
SR
19
1
SR
JR
20
1
SR
JR
21
1
JR
SR
22
1
JR
SR
23
1
JR
SR
24
3
JR
3
SR
3
25
1
JR
1
SR
1
26
1
JR
1
SR
1
27
1
SR
1
JR
2
28
1
JR
SR
SR
JR
SR
JR
29
30
1
Evaluation
After Tx 2
After Tx 1
JR
1
SR
1
JR
JR
2
JR
2
IR
1
JR
1
324
Question 10: Pain Relief from Medication
Patient #
Tx #2
Evaluation
Baseline
Evaluation
Tx #1
1
2
JR
3
SR
2
2
2
SR
3
JR
3
3
2
SR
I
JR
2
4
1
JR
I
SR
2.5
5
I
SR
I
JR
3
6
1
JR
I
SR
I
7
3
JR
2
SR
2
8
1
JR
3
SR
3
9
2
SR
3
JR
10
3
SR
II
2
JR
12
13
Evaluation
JR
2
14
SR
1
JR
SR
1
After Tx 2
After Tx 1
SR
2
JR
3
JR
3
SR
3
JR
15
3
SR
16
2
SR
17
2
SR
18
1
SR
19
1
SR
JR
20
3
SR
JR
21
2
JR
SR
22
3
JR
SR
23
3
JR
SR
24
1
JR
3
SR
2
25
2
JR
3
SR
3
26
3
JR
3
SR
3
27
2
SR
3
IR
3
28
3
JR
SR
SR
JR
SR
JR
29
30
3
3
JR
3
JR
1
JR
2
325
Question 11: Pain Relief Duration
Patient #
Baseline
Tx #1
Evl11IatHm _________
Evaluation
Tx #2
Evaluation
After Txt
_________
After T'c 2
1
2
JR
3
SR
3
2
2
SR
2
JR
3
3
1
SR
I
JR
1
4
3
IR
2
SR
3
5
1
SR
I
JR
2
6
1
JR
2
SR
1
7
3
JR
3
SR
2
8
1
JR
2
SR
2
9
2
SR
2
JR
10
3
SR
11
1
JR
12
13
JR
2
14
I
JR
SR
1
SR
SR
3
JR
3
JR
2
SR
3
JR
15
3
SR
16
1
SR
17
1
SR
18
1
SR
19
1
SR
JR
20
3
SR
JR
21
2
JR
SR
22
2
JR
SR
23
3
JR
SR
24
1
JR
1
SR
2
25
2
JR
2
SR
3
26
1
JR
3
SR
3
27
1
SR
2
JR
2
28
3
JR
SR
SR
JR
SR
JR
29
30
I
2
JR
3
JR
1
JR
I