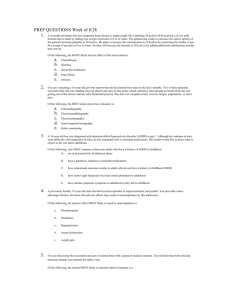
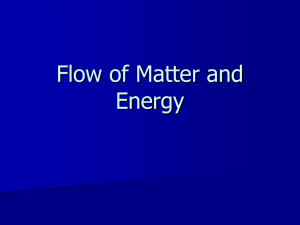
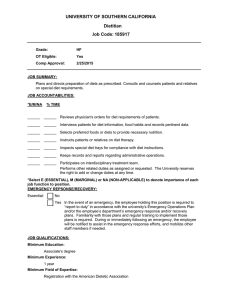
REMEDY: “Reversing menstrual dysfunction”: Examining differences in
advertisement

COLLEGE OF PUBLIC HEALTH AND HUMAN SCIENCES REMEDY: “Reversing menstrual dysfunction”: Examining differences in energy density in amenorrheic (AM) and eumenorrheic (EU) active women. Authors: W.A. Lay; T.M. Hand, RD; W.M. Sweat, MS, RD; M.M. Manore, PhD, RD, CSSD Introduction It is estimated that menstrual dysfunction, including AM, affects anywhere from 6-79% of active women1. AM is defined as the absence of a menstrual cycle lasting more than three months2. Secondary AM occurs after menarche, while primary AM is the delay of menarche until after the age of 15y2. Menstrual dysfunction can negatively impact health by reducing the achievement of peak bone mineral density (BMD) or increasing the loss of BMD5. Energy imbalance, due to insufficient energy intake to fuel high levels of exercise energy expenditure, is hypothesized as one of the primary contributors to AM in athletic women3. On contributor to lower energy intakes in active women with menstrual dysfunction may be due to the consumption of low-energy dense foods4. Energy density is a ratio of the energy (kcals) in a food and its weight (g)6. A low energy dense diet is often associated with a lower energy intake and a higher quality diet7. This type of diet is high in fruits and vegetables, low-fat dairy, and whole grains, which can be filling due to the volume of food consumed. A low energy dense diet is recommended for weight loss or maintenance due to the satiety factor of the volume of food, while being low in overall calories. Research has found that participants consume more energy when provided with energy dense food in a lab setting where ad libitum food is available for consumption6. However, for active women with high-energy needs, a low energy dense diet may not provide enough energy to fuel all their energy needs, thus, leading to AM. The purpose of this research was to measure the energy density of the diets of AM active women before and after a 6-month intervention designed to restore menstrual dysfunction and this to the diets of EU active controls. It was hypothesized that active AM athletes would have diets lower in energy density vs. active EU controls. We also hypothesized that the 6-month intervention, designed to restore menstrual function, would increase dietary energy density from pre-intervention levels. Macronutrient and micronutrient (calcium, iron, folate, vitamin B6, and vitamin B12) intakes of these women were also measured. Study Design/Methods Used This study examined the diet records of active women from the REMEDY: Reversing Menstrual Dysfunction Study8. We calculated energy density for AM (pre and post 6-month intervention) and EU active women (baseline only). The REMEDY study examined the effects of an energy replacement beverage (Gatorade Nutrition Shake; energy density 1.1 kcal/g) on reversing menstrual dysfunction in the AM women. This shake included an additional 360 kcal, 54 g of carbohydrate, 20 g of protein and 8 g of fat. Seven-day weighed food records were collected before (pre) and after (post) the 6month intervention (AM women) and at baseline for the EU women. Diets were analyzed for energy and nutrient intakes with the software program Food Processor. Calculating the energy density of a diet can be done with or without calorically dense beverages. The method used in this study included only food and liquid meal-replacement beverages as determined by Ledikwe and colleagues (2005). This method excludes all non-caloric beverages, such as water, diet sodas and most caloric beverages such as alcohol, juice, and milk. Beverages are excluded because they may show a disproportionately low energy density that may not be reflective of the individual’s actual diet6. Liquid meal replacement beverages are included in this method of calculating energy density because they can be as satiating and have a macronutrient composition similar to whole food6. Energy density was calculated from the 7-day weighed diet records of the AM active women pre- and post-intervention and the EU active women (baseline). The energy replacement beverage (82 g/d) was included in the calculation of the post-intervention AM diets. The number of servings of fruits, vegetables and low fat or fat-free dairy was determined according to the USDA’s MyPlate definitions of serving sizes. Table 2. Diet Composition and Energy Density Fruits & Vegetables Low-fat/fatfree dairy Energy from Beverages Energy Density Results For the AM group, the energy density of the diet did not change significantly due to the intervention. Energy density at baseline (pre) was 1.60 kcal/g, while energy density was 1.54 kcal/g at post-intervention. The energy density diet of the EU group was 1.84 kcal/g. For both groups, mean energy density could be categorized as medium (Energy Density: 1.5-4.0 kcal/g). Mean energy intake for the groups is given in Table 1. The intervention increased mean energy intake in the AM women from 2101 kcal/d to 2451 kcal/d, but this increase was not significantly different. The intervention added an additional 360 kcal/d to the diets of the AM women. For the EU women, mean energy intake was 2309 kcal/d, which was higher than the AM women at baseline, but not significantly different. Mean protein intake for the AM group increased from 1.3 g/kg at preintervention to 1.7 g/kg at post-intervention, with the addition of the nutrition shake that contained 20 g of protein/d. The mean protein intake in the EU group was 1.3 g/kg, which was similar to that the AM group at baseline. In Table 1, carbohydrate (g/kg) was similar for the AM group at pre and post and the EU group. Fat intake was the lowest at baseline in the pre-AM women (1.2g/kg), but similar between the AM group at post (1.4 g/kg) and the EU (1.4 g/kg) women. Fiber was the highest in the AM group at pre (13 g/1000 kcal). Pre AM Post AM EM 2.4(±2.0) 2.3(±1.6) 2.8(±1.5) 1.1(±0.8) 1.2(±0.5) 1.4(±0.7) 286(±143) 270(±202) 189(±876) 1.6(±0.2) 1.4(±0.2) 1.8(±0.3) serv/d serv/d Total Energy kcals/d Protein g/kg 1.3(±0.2) 1.7(±0.5) 1.33(±0.3) 15.5%(±8.2) 17.1%(±6.5) 14.0%(±3.5) 81(±16.0) 4.6(±1.4) 105(±24.4) 5.0(±0.9) 89(±20.7) 4.6(±1.0) % energy 52.9(±24.1) 50.98%(±18.5) 52.62%(±6.1) g/day 278(±64.1) 312(±39.4) 304(±68.8) 1.2(±0.3) 31.7%(±12.1) 1.4(±0.5) 32.5%(±12.9) 1.4(±0.4) 36.1%(±5.9) 74.0(±15.8) 88.4(±29.6) 92.7(±26.8) 0.2(±0.2) 3.3%(±0.04) 0.2(±0.2) 2.8%(±0.04) 0.1(±0.2) 1.7%(±0.02) 11.2(±13.8) 10.6(±14.4) 6.5(±9.5) % energy g/day Carbohydrate g/kg Fat g/kg % energy g/d Alcohol g/kg % energy g/d Range: 1.522.54 kcal/g kcal/d kcal/g Range: 1.251.89 kcal/g Energy density is a ratio of the energy in kilocalories to the weight in grams. The calculation included all food and liquid meal replacement type beverages. There were no differences in energy density between groups. Serv/d = Servings/day Demographics Description v Eumen (n=10) 0-mos Mean (SD) Amen (n=8) 0-mos 6-mos Age (y) 23.1 (4.3) 22.6 (3.3) N/A Age at Menarche (y) 12.7 (1.3) 13.5 (2.0) N/A Weight (kg) 66.8 (9.3) 62.4 (7.8) 64.0 (8.0) Lean Body Mass (kg) 48.5 (4.7) 46.2 (4.4) 46.1 (4.7) Fat Free Mass (kg) 51.0 (5.0) 48.5 (4.6) 48.4 (4.8) Body Mass Index (kg/m2) 23.2 (2.8) 22.3 (2.5) 22.9 (2.5) Body Fat (%) 23.2 (4.4) 22.0 (4.7) 24.1 (3.9) Exercise >4.0 METs (h/wk) 7.4 (3.6) 7.4 (3.2) 7.1 (3.4) Table 4. Examples of Very Low, Low-, Medium-, and HighEnergy-Dense Foods N/A Summary/Conclusion In conclusion, active women with amenorrhea consumed diets lower in energy density compared to their EU counterparts, but these differences were not significantly different. Both groups consumed energy intakes at the low end of the ‘medium’ energy density food category (1.5-4.0 kcal/g). It has been hypothesized that AM women may consume diets lower in energy density, which may contribute to their lower energy intakes4. We did not find this to be true. At post-intervention, the diets of the AM women did not increase, which may have been due to the increased satiety from the nutrition shake consumed daily in the intervention. It may be necessary to recommend that active women with menstrual dysfunction consume a more energy dense diet to fuel their high-energy expenditure. This may decrease their risk for developing amenorrhea and its negative health effects N/A N/A N/A References 1. Fiber g/1000kcal g/d 13.0(±3.2) 27.8(±10.3) 10.7(±4.1) 25.1(±8.6) 12.1(±11.4) 2. 28.6(±3.3) Calcium mg/d 2313(±581) 1423(±499) 1210(±385) 1000 mg 3. 4. Magnesium mg/d 243(±109) 286(±78) 364(±194) 310 mg 5. Iron mg/d 29(±14) 21(±6) 23(±9) 18 mg 6. Folate Vitamin B6 mcg/d mg/d 517(±467) 3.4(±2.8) 404(±234) 16.4(±40.1) 449(±207) 3.4(±2.3) 400 mcg 1.3 mg 7. Vitamin B12 mcg/d 13.3(±25.0) 6.2(±3.7) 8.0(±5.2 2.4 mcg 316(±308) 303(±296) 385(±314) 600 IU Vitamin D IU % en = % of energy Range: 1.271.82 kcal/g Table 3. Participant Demographics (mean ±SD) Table 1. Energy and Nutrient Information Pre AM Post AM EM RDA/DRI 2101(±309) 2451(±483) 2309(±472) N/A Figure 1. Energy Density of Amenorrheic active women at Pre- and Post-Intervention and Eumenorrheic Active Women at baseline (pre) 8. Adapted from: Sweat, W., Manore, M. (2012). Low Energy-Dense Diets: Can you really eat more and lose weight? ACSM Health & Fitness Journal, 16, 1-7. 9. 10. Beals KA, Manore MM. Disorders of the female athlete triad among collegiate athletes. Internation Journal of Sport Nutrition and Exercise Metabolism. 2002; 12: 281-293. Nattiy A, Loucks AB, Manore MM, Sanborn CF, Sundgot-Borgen J, Warren MP. Position Stand: The Female Athlete Triad. American College of Sports Medicine. 2007. Manore MM. Dietary recommendations and athletic menstrual dysfunction. Sports Med. 2002; 32:887-901. De Souza MJ, Maguire MS, Maresh CM, Kraemer WJ, Rubin KR, Loucks AB. Adrenal activation and the prolactin response to exercise in eumenorrheic and amenorrheic runners. Journal of Applied Physiology. 1991; 70: 2378-2387. Drinkwater BL, Nilson K, Chesnut CH, et al. Bone mineral content of amenorrheic and eumenorrheic athletes. N Engl J Med. 1984; 311: 277-81. Ledikwe JH, Blanck HM, Khan LK, Serdula MK, Seymour JD, Tohill BC, Rolls BJ. Dietary energy density determined by eight calculation methods in a nationally representative United States population. J. Nutr. 2005; 135: 273-278. Ledikwe JH, Blanck HM, Khan LK, Serdula MK, Seymour JD, Tohill BC, Rolls BJ. Low-energy-density diets are associated with high diet quality in adults in the United States. J Am Diet Assoc. 2006; 106:1172-1180. Kam LC. Reversing Menstrual Dysfunction (REMEDY): The impact of menstrual status on musculoskeletal and hormonal health. Corvallis, OR: Oregon State University; 2011. Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Micronutrients. Washington, DC: National Academy Press, 2010. Sweat, W., Manore, M. (2012). Low Energy-Dense Diets: Can you really eat more and lose weight? ACSM Health & Fitness Journal, 16, 1-7. Demographics Description Age (y) Age at Menarche (y) Weight (kg) Lean Body Mass (kg) Fat Free Mass (kg) Body Mass Index (kg/m2) Body Fat (%) Exercise >4.0 METs (h/wk) Mean (SD) Eumen (n=10) Amen (n=8) Pre AM Fruits & Vegetables serv/d 2.4(±2.0) 0-mos 0-mos 6-mos Low-fat/fat-free dairy serv/d 1.1(±0.8) 23.1 (4.3) (3.3) N/A 286(±143) Energy from Beverages 22.6 kcal/d Energy Density kcal/g 1.6(±0.2) 12.7 (1.3) 66.8 (9.3) 13.5 (2.0) 62.4 (7.8) N/A 64.0 (8.0) 48.5 (4.7) 51.0 (5.0) 46.2 (4.4) 48.5 (4.6) 46.1 (4.7) 48.4 (4.8) 23.2 (2.8) 23.2 (4.4) 22.3 (2.5) 22.0 (4.7) 22.9 (2.5) 24.1 (3.9) 7.4 (3.6) 7.4 (3.2) 7.1 (3.4) Post AM 2.3(±1.6) 1.2(±0.5) 270(±202) 1.4(±0.2) EM 2.8(±1.5) 1.4(±0.7) 189(±876) 1.8(±0.3) v Pre AM Total Energy Protein Carbohydrate Fat Alcohol Fiber Calcium Magnesium Iron Folate Vitamin B6 Vitamin B12 Vitamin D kcals/d g/kg % energy g/day g/kg % energy g/day g/kg % energy g/d g/kg % energy g/d g/1000kcal g/d mg/d mg/d mg/d mcg/d mg/d mcg/d IU Post AM 2101(±309) 1.3(±0.2) 15.5%(±8.2) 81(±16.0) 4.6(±1.4) 52.9(±24.1) 278(±64.1) 1.2(±0.3) 31.7%(±12.1) 74.0(±15.8) 0.2(±0.2) 3.3%(±0.04) 11.2(±13.8) 13.0(±3.2) 27.8(±10.3) 2313(±581) 243(±109) 29(±14) 517(±467) 3.4(±2.8) 13.3(±25.0) 316(±308) EM 2451(±483) 1.7(±0.5) 17.1%(±6.5) 105(±24.4) 5.0(±0.9) 50.98%(±18.5) 312(±39.4) 1.4(±0.5) 32.5%(±12.9) 88.4(±29.6) 0.2(±0.2) 2.8%(±0.04) 10.6(±14.4) 10.7(±4.1) 25.1(±8.6) 1423(±499) 286(±78) 21(±6) 404(±234) 16.4(±40.1) 6.2(±3.7) 303(±296) v RDA/DRI 2309(±472) 1.33(±0.3) 14.0%(±3.5) 89(±20.7) 4.6(±1.0) 52.62%(±6.1) 304(±68.8) 1.4(±0.4) 36.1%(±5.9) 92.7(±26.8) 0.1(±0.2) 1.7%(±0.02) 6.5(±9.5) 12.1(±11.4) 28.6(±3.3) 1210(±385) 364(±194) 23(±9) 449(±207) 3.4(±2.3) 8.0(±5.2 385(±314) N/A N/A N/A N/A N/A 1000 mg 310 mg 18 mg 400 mcg 1.3 mg 2.4 mcg 600 IU